The administration of teriparatide in addition to VFG can possibly help achieve complete spinal fusion in patients with neurofibromatosis type 1-associated cervical deformity.
Dr. Yohei Kakuta, Department of Orthopaedic Surgery, Gunma University Graduate School of Medicine, 3-39-22, Showa, Maebashi, Gunma 371-8511 Japan. E-mail: m1620020@gunma-u.ac.jp
Introduction: Cervical kyphosis is sometimes observed in neurofibromatosis Type 1 (NF-1). If NF-1-associated cervical deformity is progressive, surgical intervention is needed to prevent further deterioration of the deformity. The rate of nonunion after spinal fusion is high in NF-1, especially dystrophic NF-1.
Case Report: We experienced a 33-year-old woman with cervical kyphosis induced by NF-1. She was treated by two-stage circumferential bone fusion with a vascularized free fibula followed by teriparatide administration and achieved complete spinal fusion with this approach.
Conclusion: We administered the teriparatide after spinal fusion surgery for NF-1 associated cervical deformity and obtained complete bony fusion. The administration of teriparatide may be useful to achieve complete bone fusion in patients with NF-1-associated cervical deformity.
Keywords: Teriparatide, cervical kyphosis, neurofibromatosis Type 1.
Neurofibromatosis Type 1 (NF-1) is sometimes associated with spinal deformities, including scoliosis and cervical kyphosis [1, 2] If NF-1-associated cervical deformity is progressive, surgical intervention is needed to prevent further deterioration of the deformity [3]. Single posterior instrumented fusion for cervical deformities due to NF-1 has been shown to result in a high rate of pseudoarthrosis and correction loss (63%) [4]. To date, many researchers have shown an interest in drug treatment promoting bone fusion after spinal surgery [5, 6, 7]. However, only a few studies have reported the usefulness of such treatments for bone fusion [6], and there are no guidelines for the treatment at present. We herein report a case of cervical kyphosis induced by NF-1 treated by two-stage circumferential spinal fusion with an autologous vascularized fibula graft followed by the administration of teriparatide.
A 33-year-old woman visited our hospital due to neck pain and cervical kyphotic deformity. She had a history of NF-1 and her neurological findings were normal at her first visit. X-ray of the cervical spine showed severe wedged deformity of the vertebral body at the C3 and C4 levels and the kyphotic angle was 56° (Fig. 1a). Magnetic resonance imaging of the spine showed neither spinal cord compression nor spinal cord tumor (Fig. 1b). We performed the initial surgery of O-T2 posterior spinal fusion after halo traction for one week (Fig. 2). We then performed the second surgery of anterior spinal fusion from C3 to C6 using an autologous vascularized fibular graft 3 weeks after the initial surgery. After performing corpectomy of the C4 and C5 vertebral bodies, the vessels of the fibular graft were anastomosed to the superior thyroid artery and vein under a microscope. The cervical kyphotic angle improved from 56° to 0° on X-ray (Fig. 3a and b).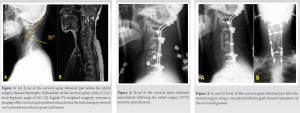 We placed the patient in a halo vest for 1 month and additionally started teriparatide treatment 20 µg/day for coexisting bone fragility 1 week after the second surgery. Follow-up computed tomography (CT) 3–7 months after surgery demonstrated a trend toward bony fusion and partial bony fusion of the grafted fibula, respectively (Fig. 4a and b). Furthermore, CT findings showed complete bony fusion 12 months after surgery (Fig. 4c). Seven years after the surgery, her neurological condition was normal despite slight neck stiffness and cervical spine X-ray showed maintenance of alignment immediately after surgery (Fig. 5). In the present case, complete bony fusion was achieved within 12 months after two-stage circumferential spinal fusion using an autologous vascularized free fibula and teriparatide administration. The rate of non-union after spinal fusion is high in NF-1, especially dystrophic NF-1 [4, 8]. A vascularized fibular graft is recognized as an option for the surgical management of NF-1-associated cervical kyphosis. Asazuma et al. performed anterior and posterior spinal fixation for a patient with cervical kyphosis induced by neurofibromatosis. They used a vascularized free fibula for anterior fixation, which resulted in complete bone fusion [9], whereas Saika et al. reported that bone union was not achieved in 30% of the patients who underwent anterior spinal fusion surgery even when a vascularized fibular graft was used [10]. We also used a vascularized free fibula in the anterior surgery of the present patient following posterior instrumented fusion and obtained complete anterior fusion, but we additionally started teriparatide treatment for bone fragility after the two-stage surgery. Recently, it has been reported that teriparatide promotes fusion in spinal fusion surgery [11] and fracture healing [7, 12]. Lehman et al. showed that the histologic intertransverse process fusion rate differed significantly between the teriparatide group and controls (86.7% vs. 50%) in a rabbit model [13]. Furthermore, Sugiura et al. also reported that teriparatide enhanced bone healing and bone fusion in rats [14]. In humans, the use of teriparatide has a positive effect on improving the rate of bone fusion. Seki et al. demonstrated the advantages of teriparatide for bone fusion after surgery for adult spinal deformity in osteoporotic patients [11]. Ohtori investigated the effect of teriparatide on bone fusion after lumbar spinal fixation. The bone fusion rate was greater in the teriparatide group than in the bisphosphonate group (82% vs. 68 %) [6]. Furthermore, the mean time to fusion was shorter in the teriparatide group than in the bisphosphonate group (8 vs. 10 months) [6]. In the present study, we administered the teriparatide for bone fragility after spinal fusion for NF-1-associated cervical deformity and obtained complete bony fusion, although we also used an autologous vascularized fibular graft to promote bone fusion. We speculate that not only the use of a vascular fibular graft but also the administration of teriparatide for bone fragility may be associated with complete fusion after surgery based on the findings of the previous studies concerning the effect of teriparatide on spinal fusion.
We placed the patient in a halo vest for 1 month and additionally started teriparatide treatment 20 µg/day for coexisting bone fragility 1 week after the second surgery. Follow-up computed tomography (CT) 3–7 months after surgery demonstrated a trend toward bony fusion and partial bony fusion of the grafted fibula, respectively (Fig. 4a and b). Furthermore, CT findings showed complete bony fusion 12 months after surgery (Fig. 4c). Seven years after the surgery, her neurological condition was normal despite slight neck stiffness and cervical spine X-ray showed maintenance of alignment immediately after surgery (Fig. 5). In the present case, complete bony fusion was achieved within 12 months after two-stage circumferential spinal fusion using an autologous vascularized free fibula and teriparatide administration. The rate of non-union after spinal fusion is high in NF-1, especially dystrophic NF-1 [4, 8]. A vascularized fibular graft is recognized as an option for the surgical management of NF-1-associated cervical kyphosis. Asazuma et al. performed anterior and posterior spinal fixation for a patient with cervical kyphosis induced by neurofibromatosis. They used a vascularized free fibula for anterior fixation, which resulted in complete bone fusion [9], whereas Saika et al. reported that bone union was not achieved in 30% of the patients who underwent anterior spinal fusion surgery even when a vascularized fibular graft was used [10]. We also used a vascularized free fibula in the anterior surgery of the present patient following posterior instrumented fusion and obtained complete anterior fusion, but we additionally started teriparatide treatment for bone fragility after the two-stage surgery. Recently, it has been reported that teriparatide promotes fusion in spinal fusion surgery [11] and fracture healing [7, 12]. Lehman et al. showed that the histologic intertransverse process fusion rate differed significantly between the teriparatide group and controls (86.7% vs. 50%) in a rabbit model [13]. Furthermore, Sugiura et al. also reported that teriparatide enhanced bone healing and bone fusion in rats [14]. In humans, the use of teriparatide has a positive effect on improving the rate of bone fusion. Seki et al. demonstrated the advantages of teriparatide for bone fusion after surgery for adult spinal deformity in osteoporotic patients [11]. Ohtori investigated the effect of teriparatide on bone fusion after lumbar spinal fixation. The bone fusion rate was greater in the teriparatide group than in the bisphosphonate group (82% vs. 68 %) [6]. Furthermore, the mean time to fusion was shorter in the teriparatide group than in the bisphosphonate group (8 vs. 10 months) [6]. In the present study, we administered the teriparatide for bone fragility after spinal fusion for NF-1-associated cervical deformity and obtained complete bony fusion, although we also used an autologous vascularized fibular graft to promote bone fusion. We speculate that not only the use of a vascular fibular graft but also the administration of teriparatide for bone fragility may be associated with complete fusion after surgery based on the findings of the previous studies concerning the effect of teriparatide on spinal fusion.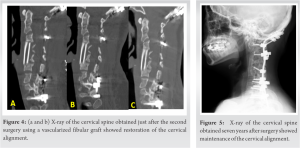
We experienced a case of cervical kyphosis induced by NF-1 that was treated with two-stage circumferential spinal fusion with a vascularized free fibula followed by teriparatide treatment for bone fragility and obtained complete spinal fusion with this treatment approach.
Cervical kyphosis is sometimes observed in NF-1. The rate of nonunion after spinal fusion is high in NF-1, especially dystrophic NF-1. The administration of teriparatide in addition to VFG can possibly help to achieve complete spinal fusion in patients with NF-1-associated cervical deformity.
References
- 1.Crawford AH, Herrera-Soto J. Scoliosis associated with neurofibromatosis. Orthop Clin North Am 2007;38:553-62. [Google Scholar]
- 2.Gabriel KR. Neurofibromatosis. Curr Opin Pediatr 1997;9:89-93. [Google Scholar]
- 3.Kawabata S, Watanabe K, Hosogane N, Ishii K, Nakamura M, Toyama Y, et al. Surgical correction of severe cervical kyphosis in patients with neurofibromatosis Type 1. J Neurosurg Spine 2013;18:274-9. [Google Scholar]
- 4.Parisini P, Di Silvestre M, Greggi T, Paderni S, Cervellati S, Savini R. Surgical correction of dystrophic spinal curves in neurofibromatosis. A review of 56 patients. Spine (Phila Pa 1976) 1999;24:2247-53. [Google Scholar]
- 5.Chaudhary N, Lee JS, Wu JY, Tharin S. Evidence for use of teriparatide in spinal fusion surgery in osteoporotic patients. World Neurosurg 2017;100:551-6. [Google Scholar]
- 6.Ohtori S, Orita S, Yamauchi K, Eguchi Y, Ochiai N, Kuniyoshi K, et al. More than 6 months of teriparatide treatment was more effective for bone union than shorter treatment following lumbar posterolateral fusion surgery. Asian Spine J 2015;9:573-80. [Google Scholar]
- 7.Liu Y, Levack AE, Marty E, Or O, Samuels BP, Redko M, et al. Anabolic agents: What is beyond osteoporosis? Osteoporos Int 2018;29:1009-22. [Google Scholar]
- 8.Kim YH, Reoyan GN, Ha KY, Kim CK. Pseudarthrosis repair using autologous cultured osteoblasts in complex Type-1 neurofibromatosis spinal deformity: A case report and review of the literature. Spine (Phila Pa 1976) 2016;41:E1372-8. [Google Scholar]
- 9.Asazuma T, Yamagishi M, Nemoto K, Amako M, Osada M, Fujikawa K. Spinal fusion using a vascularized fibular bone graft for a patient with cervical kyphosis due to neurofibromatosis. J Spinal Disord 1997;10:537-40. [Google Scholar]
- 10.Saika M, Kawai S, Doi K, Sakai K, Itou H. Free vascularized fibula graft for anterior cervical fusion. Cent Jpn J Orthop Traumat 1992;35:681-2. [Google Scholar]
- 11.Seki S, Hirano N, Kawaguchi Y, Nakano M, Yasuda T, Suzuki K, et al. Teriparatide versus low-dose bisphosphonates before and after surgery for adult spinal deformity in female Japanese patients with osteoporosis. Eur Spine J 2017;26:2121-7. [Google Scholar]
- 12.Aspenberg P, Genant HK, Johansson T, Nino AJ, See K, Krohn K, et al. Teriparatide for acceleration of fracture repair in humans: A prospective, randomized, double-blind study of 102 postmenopausal women with distal radial fractures. J Bone Miner Res 2010;25:404-14. [Google Scholar]
- 13.Lehman RA Jr., Dmitriev AE, Cardoso MJ, Helgeson MD, Christensen CL, Raymond JW, et al. Effect of teriparatide [rhPTH(1,34)] and calcitonin on intertransverse process fusion in a rabbit model. Spine (Phila Pa 1976) 2010;35:146-52. [Google Scholar]
- 14.Sugiura T, Kashii M, Matsuo Y, Morimoto T, Honda H, Kaito T, et al. Intermittent administration of teriparatide enhances graft bone healing and accelerates spinal fusion in rats with glucocorticoid-induced osteoporosis. Spine J 2015;15:298-306. [Google Scholar]