
When treating elderly patients with gross instability following a traumatic shoulder dislocation, physicians should consider concomitant fractures which may result in shoulder instability
Dr. Ian J Wellington, Department of Orthopaedic Surgery, University of Connecticut Health center, 120 Dowling Way, Farmington, CT, 06034, USA. E-mail: iwellington@uchc.edu
Abstract
Introduction: Traumatic shoulder dislocations in elderly patients can result in significant shoulder pathology. Rotator cuff tears and recurrent instability are common complications follow a dislocation event, while axillary nerve injury is less common. While there have been rare cases of recurrent shoulder instability with concomitant axillary nerve injury, there have been no prior cases, in which concurrent fracture fragmentation resulted in the initial gross instability.
Case Report: A 68-year-old male with painful gross instability presents following a traumatic dislocation. The patient sustained an axillary nerve injury to the ipsilateral side resulting in a non-functioning deltoid. Pre operative X-rays showed recurrent chronic glenohumeral dislocation, computerized tomography imaging showed a greater tuberosity fracture, and magnetic resonance imaging showed a massive cuff tear with retraction and atrophy. Given the level of instability and deltoid dysfunction, the patient was treated with shoulder arthrodesis. Intraoperatively, a large fragment of greater tuberosity with ligamentous attachments was found adhered to the anterior glenoid. After arthrodesis, the patient’s pain and function improved significantly.
Conclusion: When treating elderly patients with gross instability following a traumatic dislocation, surgeons should keep in mind the high likelihood of concomitant avulsion fracture, and that migratory cortical fragments can be a nidus for a patient’s instability. When selected for appropriately, these patients can be effectively treated with shoulder arthrodesis with excellent improvements of pain and functionality.
Keywords: Arthrodesis, Shoulder, Fusion
Traumatic shoulder dislocation in elderly patients can involve extensive soft -tissue injuries to the capsule, labrum, rotator cuff, brachial plexus, and axillary nerve. Axillary nerve injuries are a relatively uncommon complication in young patients but occur about 9.3% of the time in patients over 60- years – old [1] Older patients are also predisposed to rotator cuff injury following a primary dislocation, with rates of approximately 63% in those over 50 years of age [2]. While older patients with large cuff injuries can be treated with reverse total shoulder arthroplasty (rTSA), patients with pre-operative axillary neuropathy treated with rTSA have poor forward flexion and worse Constant constant scores compared to those with a functioning axillary nerve [3]. For these patients, shoulder arthrodesis remains a viable alternative. In the proper patient, shoulder arthrodesis can offer significant pain relief, while maintaining most of the functional goal of the shoulder joint, which is to position the hand in space [4,5,6]. In Aadditionally, older patients may develop gross instability following traumatic dislocation. In this population, the instability can be secondary to rotator cuff tear, humeral head fracture, or glenoid fracture. Diminished bone quality makes elderly patients more susceptible to a concomitant humeral head fracture, particularly of the greater tuberosity [7]. We present a case of traumatic anterior shoulder dislocation with massive rotator cuff tear, uniquely significant painful gross global instability, and a complete axillary nerve palsy visible on both clinical examination and post-injury imaging (Fig. 1). The patient was treated with a glenohumeral arthrodesis as a salvage procedure. Intraoperatively, a large piece of greater tuberosity with attached supraspinatus and infraspinatus, and biceps tendon was found interposed on the glenoid. This fragment was determined to be a contributing factor to the patient’s gross instability. Post-operatively, the patient had significant improvement of his pain and function.
Medical history and presentation
The patient is a 68-year-old left-hand dominant male who initially presented to the clinic 2 months after a traumatic right anterior shoulder dislocation after falling from his car with persistent pain and feelings of instability. He underwent successful closed reduction under conscious sedation at an outside emergency department. He had continued pain and instability following his initial dislocation and endorsed that his shoulder was spontaneously dislocating and reducing. X-ray and computerized tomography (CT) imaging showed continued massive instability of the glenohumeral joint with bony fragmentation suggestive of a greater tuberosity fracture with marked widening of the glenohumeral joint space (Fig. 1a and b). An magnetic resonance imaging was obtained by his primary care provider 1 month from his initial injury, which demonstrated anterior dislocation of the glenohumeral joint and complete tear of all rotator cuff muscles with retraction (Fig. 2).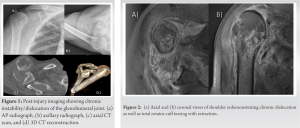
Physical examination
Two months from the initial injury, the patient presented to our orthopedic clinic for evaluation. His shoulder was exceptionally unstable; any motion of his elbow would cause a dislocation with subsequent spontaneous reduction. These dislocation events were exquisitely painful for him. In addition, he had no cutaneous sensation within the axillary nerve distribution, and his deltoid was non-contractile. He could accomplish 10° of forward elevation and 10° of abduction, as well as 20° of extension.
Additional examinations/diagnosis
Given clinical concern for axillary nerve palsy, he was evaluated by a neurologist, and an EMG was obtained, which demonstrated severe right axillary neuropathy with denervation of the right deltoid. A CT scan was also obtained showing chronic dislocation of the glenohumeral joint with a sclerotic appearance of the humeral head suggestive of avascular necrosis (Fig. 1c and d).
Interventions
While a patient with a massive rotator cuff tear and continued pain would normally benefit from rTSA, his axillary nerve injury and complete lack of deltoid function made him an inappropriate candidate for this procedure. Unfortunately, the remaining option was a shoulder fusion, to stabilize the shoulder in a functional position while limiting instability and pain. The patient was placed in a modified beach chair position. A 25 cm incision centered over the anterior one-third of the deltoid was made from the spine of the scapula, over the acromion, and to the midshaft humerus. The approach was continued until the spine of the scapula, acromion, and the raphae between the anterior and middle thirds of the deltoid muscle were visualized. The axillary nerve was identified and protected distally. The deltoid was then dissected off the anterior and lateral acromion and tagged for later repair (Fig. 3a). A large fragment of the greater tuberosity with attachments to the supraspinatus, infraspinatus, and biceps tendon was interposed between the humeral head and glenoid. This piece was determined to be a contributing factor to the patient’s gross recurrent instability. Dissection through the supraspinatus, infraspinatus, and subscapularis was carried out until full access to the glenoid was achieved (Fig. 3c). Using an osteotome and a high-speed burr, cartilage was removed from the glenoid and the humeral head, and the undersurface of the acromion was decorticated to ensure bony apposition to enhance fusion potential (Fig. 3b). The shoulder was positioned in approximately 10 to 20° of abduction, 20° of flexion, and 30 to 40° of internal rotation. The glenohumeral joint was reduced and two 7.3 mm partially threaded cannulated screws were placed from the lateral humerus into the glenoid under fluoroscopic guidance (Fig. 4). 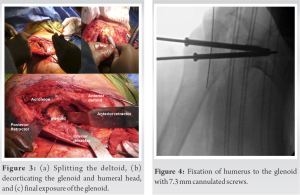 A 12-hole 4.5 mm heavy recon plate (DePuy Synthes, West Chester, PA) was applied. The plate was pre-bent to match the contour of the spine of the scapula, over the acromion, and down to lateral humerus on a cadaveric specimen the evening before surgery (Fig. 5a). After pre-contouring, the plate was appropriately sterilized for use in the procedure. Small adjustments were made to contour the plate using plate-bending instruments (Fig. 5b). The plate was then applied (Fig. 5c), and appropriate placement was confirmed fluoroscopically (Fig. 5d).
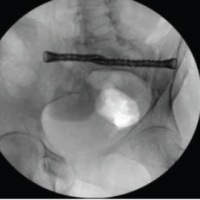
A 12-hole 4.5 mm heavy recon plate (DePuy Synthes, West Chester, PA) was applied. The plate was pre-bent to match the contour of the spine of the scapula, over the acromion, and down to lateral humerus on a cadaveric specimen the evening before surgery (Fig. 5a). After pre-contouring, the plate was appropriately sterilized for use in the procedure. Small adjustments were made to contour the plate using plate-bending instruments (Fig. 5b). The plate was then applied (Fig. 5c), and appropriate placement was confirmed fluoroscopically (Fig. 5d). Initial fixation was achieved using 4.5 mm screws, and then, three 6.5 mm partially threaded cancellous screws were placed through the plate, into the acromion, and into the humeral head. Another 6.5 mm screw was placed laterally into the plate, through the humeral head, and into the glenoid (Fig. 6). 15 cc of cancellous bone allograft was then packed into the glenohumeral joint to aid in fusion. Iliac crest autograft may also be used; however, this was deferred given the patient’s body habitus. After the wound was irrigated, the deltoid was repaired to the lateral edge of the acromion using #2 FiberWire (Arthrex, Naples, FL) (Fig. 7). The anterior and middle thirds of the deltoid were approximated using #2 FiberWire. The remainder of the wound was closed in the usual fashion.
Initial fixation was achieved using 4.5 mm screws, and then, three 6.5 mm partially threaded cancellous screws were placed through the plate, into the acromion, and into the humeral head. Another 6.5 mm screw was placed laterally into the plate, through the humeral head, and into the glenoid (Fig. 6). 15 cc of cancellous bone allograft was then packed into the glenohumeral joint to aid in fusion. Iliac crest autograft may also be used; however, this was deferred given the patient’s body habitus. After the wound was irrigated, the deltoid was repaired to the lateral edge of the acromion using #2 FiberWire (Arthrex, Naples, FL) (Fig. 7). The anterior and middle thirds of the deltoid were approximated using #2 FiberWire. The remainder of the wound was closed in the usual fashion.
Outcomes
Postoperatively, the patient was made non-weight-bearing in a sling but allowed the use of his hand and wrist and allowed elbow ROM. Serial x-rays were performed at 6 days, 6 weeks, and 12 weeks which showed maintained alignment. After 12 weeks, the patient was allowed to work on scapular exercises. Physical therapy consisted of scapulothoracic range of motion exercises as well as strengthening. The patient worked twice weekly with an outpatient physical therapist after the 12 weeks post-operative period for 10 weeks. The patient noted significant improvement of his pre-operative symptoms with no residual pain or feelings of instability. Radiographs at 6 months showed excellent fusion consolidation of the glenohumeral joint (Fig. 8). He was able to obtain 60° of abduction and 60° of forward elevation from scapulothoracic motion. He was able to reach his mouth/face with the affected limb without pain or difficulty. The patient was able to perform activities of daily living such as eating, dressing, and self-hygiene without issue.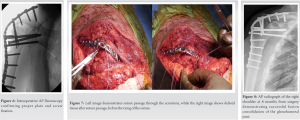
Instability of the glenohumeral joint and massive rotator cuff tears of the shoulder are commonly encountered pathologies in the world of shoulder surgery. These issues compounded with axillary nerve palsy and a non- functioning deltoid significantly complicate management. In the elderly patient with a massive/irreparable rotator cuff tear, a rTSA is an excellent option; however, it is contraindicated in patients with a non-functioning deltoid. Glenohumeral joint arthrodesis is an end-stage salvage procedure used to address pain and instability of the shoulder. Indications include brachial-plexus injury, chronic recalcitrant instability, salvaging a radical tumor resection, and combined rotator cuff and deltoid paralysis [5]. Furthermore, while anatomic and rTSA have become the primary and generally definitive treatment of glenohumeral arthritis, fusion serves as an option when arthroplasty fails or is contraindicated. Severe bone loss of the glenoid or humerus after multiple procedures, chronic infection, rotator cuff, and deltoid dysfunction are all indications for glenohumeral joint arthrodesis in patients with primary arthritis. The precise positioning of the fused shoulder joint is an important consideration to maximize a patient’s function. As the functional goal of the shoulder is to position the hand in space, positioning the glenohumeral joint during arthrodesis must optimize the shoulder’s ability to fulfill this role. There are various theories regarding optimal arm position in glenohumeral arthrodesis [8,9]. Proper positioning of the arm in space to maximize function is balanced by the need for adequate fixation, stabilization, and bony contact to obtain union and success of the arthrodesis. In 1997, Groh et al. reviewed patients necessitating revision of their fusion secondary to malposition and recommended a position of 10–15° of abduction and flexion and 40–60° of internal rotation [9]. While this patient underwent arthrodesis of his non-dominant extremity, had this injury been in the dominant extremity, it would have been fused in a similar position. This is because this position allows for the greatest degree of function regardless of hand dominance. The goal of shoulder arthrodesis is to provide stability and relieve pain while still allowing for some ability to complete activities of daily living. Adequate fixation does generally provide reliable pain relief. In a small case series, Rouholamin et al. reported that ten out of 15 patients at a mean follow-up of 32 months gained excellent and sustained pain relief [10]. Similarly, Cofield et al. reported that more than 60% of their 65 person cohort were pain-free or had mild pain postoperatively [8]. Precise positioning of the shoulder can sometimes be counterproductive to achieving adequate fixation and stabilization of the shoulder joint, but it is paramount to a satisfactory functional outcome. Groh et al. performed corrective osteotomy in a series of 9 patients whose original positioning was outside their parameters (10–15° of abduction/flexion, 40–60° internal rotation) and was able to demonstrate improved functioning in activities of daily living [9].
The pain, gross instability, and lack of deltoid function made this patient an appropriate candidate for shoulder fusion. Surgeons treating older patients with traumatic shoulder dislocations should be aware of the risks of rotator cuff tearing, axillary nerve injury, and concomitant fracture. Shoulder arthrodesis can successfully treat pain and instability in patients with this pathology.
To date, there have been no cases of instability caused by a greater tuberosity fragment adherent to a glenoid with concomitant rotator cuff tearing and complete axillary nerve palsy. While this pathology is rare, it presents one of the few remaining indications for glenohumeral arthrodesis. Physicians managing patients with recurrent painful instability with a non-functioning deltoid should consider arthrodesis as a predictable and successful method for treatment.
References
- 1.Gumina S, Postacchini F. Anterior dislocation of the shoulder in elderly patients. J Bone Joint Surg Br 1997;79:540-3. [Google Scholar | PubMed]
- 2.Ribbans WJ, Mitchell R, Taylor GJ. Computerised arthrotomography of primary anterior dislocation of the shoulder. J Bone Jt Surg Br 1990;72:181-5. [Google Scholar | PubMed]
- 3.Garofalo R, Flanagin B, Castagna A, Calvisi V, Krishnan SG. Massive irreparable rotator cuff tear and associated deltoid tear. Does the reverse shoulder arthroplasty and deltoid repair be a possible option of treatment? J Orthop Sci 2016;21:753-8. [Google Scholar | PubMed]
- 4.Kamineni S, Ankem H, Patten DK. Anatomic relationship of the radial nerve to the elbow joint: Clinical implications of safe pin placement. Clin Anat 2009;22:684-8. [Google Scholar | PubMed]
- 5.Safran O, Iannotti JP. Arthrodesis of the shoulder. J Am Acad Orthop Surg 2006;14:145-53. [Google Scholar | PubMed]
- 6.Clare DJ, Wirth MA, Groh GI, Rockwood CA Jr. Shoulder arthrodesis. J Bone Joint Surg Am 2001;83:593-600. [Google Scholar | PubMed]
- 7.Shin SJ, Yun YH, Kim DJ, Yoo JD. Treatment of traumatic anterior shoulder dislocation in patients older than 60 years. Am J Sports Med 2012;40:822-7. [Google Scholar | PubMed]
- 8.Cofield RH, Briggs BT. Glenohumeral arthrodesis. Operative and long-term functional results. J Bone Joint Surg Am 1979;61:668-77. [Google Scholar | PubMed]
- 9.Groh GI, Williams GR, Jarman RN, Rockwood CA Jr. Treatment of complications of shoulder arthrodesis. J Bone Joint Surg Am 1997;79:881-7. [Google Scholar | PubMed]
- 10.Rouholamin E, Wootton JR, Jamieson AM. Arthrodesis of the shoulder following brachial plexus injury. Injury 1991;22:271-4. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2025 Stealth Navigation with iFuse-TORQ Implant for Sacroiliac Joint Fusion Technique Guide
February 1, 2025 Stealth Navigation with iFuse-TORQ Implant for Sacroiliac Joint Fusion Technique Guide December 1, 2024 The Journey of an Ankylosed Hip: A 20 Year Long-Term Follow-up of an Hip Arthrodesis using Cobra Plate – The Present Day Relevance
December 1, 2024 The Journey of an Ankylosed Hip: A 20 Year Long-Term Follow-up of an Hip Arthrodesis using Cobra Plate – The Present Day Relevance August 1, 2026 Isolated Calcific Deposition in the Subacromial Bursa: A Rare Case Report and Arthroscopic Management
August 1, 2026 Isolated Calcific Deposition in the Subacromial Bursa: A Rare Case Report and Arthroscopic Management August 1, 2026 Why the Ilizarov Ring Fixator Remains the Preferred Technique for Knee Arthrodesis in Complex Knee Conditions: A Case Series
August 1, 2026 Why the Ilizarov Ring Fixator Remains the Preferred Technique for Knee Arthrodesis in Complex Knee Conditions: A Case Series