
Removal of transverse process at L2 and L3 can provide access to the anterior structures, thereby limiting the need for dual exposure for resection of the mass.
Dr. Munis Ashraf, Department of Orthopaedics, Saveetha Medical College and Hospitals, Thandalam, Chennai, Tamil Nadu, India E-mail: munis6@gmail.com
Abstract
Introduction: Ganglioneuroma (GN) is a rare benign tumor of neural crest origin mostly found in the abdomen, but may occasionally present at sites including the cervical, lumbar, or sacral spine. GN of lumbar spine is a rare occurrence.
Case Report: A 52-year-old man presented with GN in the L1 nerve root, who underwent successful resection of the tumor and stabilization of spine using a single posterior approach.
Conclusion: GN should be considered as a differential in any case of paraspinal mass. A high index of clinical suspicion and correlation with radiological findings is necessary in differentiating a large benign tumor from a malignant growth. Complete surgical excision is the treatment of choice; however, the approach to the mass is dictated by the tumor size and location.
Keywords: Spinal tumor, ganglioneuroma, single approach, stabilization.
Ganglioneuroma (GN) is a rare benign tumor which originates from neural crest cells of sympathetic ganglia or adrenal medulla [1], and it usually presents in the retroperitoneum (mostly in the presacral space), posterior mediastinum, or adrenal gland, and occasionally in unusual locations [2]. We report a giant dumbbell-shaped GN of L1 extending into the retroperitoneum which was resected en mass posteriorly without the need for an additional retroperitoneal exposure.
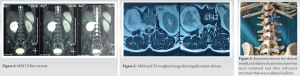
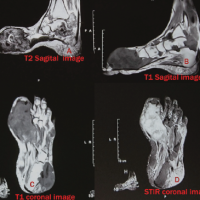
A 52-year-old male, tailor by profession, presented with mid/low back ache for the past 5 months. The patient had no history of trauma or lifting weights. The patient had dull aching pain which aggravated on exertion and forward flexion. There were no history of fever, loss of weight, or appetite. The patient had no motor or sensory deficits. There was no radiating pain, symptoms did not settle after trying analgesics and physiotherapy. On admission, X-ray was taken and showed scalloping of the L1 vertebral body, increased canal diameter, and thinning of L1 pedicle. Computed tomography (CT) lumbosacral spine showed extramedullary mass measuring 5.6 × 5.9 × 6.9 (AP × TR × CC) epicentered at the level of L1-2 right foraminal level extending laterally to lie within right psoas muscle. Magnetic resonance imaging LS spine with contrast showed an extramedullary T1 isointense, T2 heterogeneously hyperintense lesion measuring 5.6 × 5.9 × 6.9 epicenter at the level of L1-L2 right foraminal level extending laterally to lie within psoas muscle, and anteriorly causing indentation of posterior aspect of the right kidney. Lesion appears as dumbbell shaped and causes neural foraminal widening (19 mm), mild displacement of the cord posterolaterally. Post-contrast images show heterogeneous contrast enhancement with non-enhancing necrotic components (Fig. 1, 2, 3, 4, 5). A CT-guided biopsy was taken to confirm the diagnosis.
Surgical Technique
The initial plan was a two staged procedure with stabilization of spine posteriorly and then to dissect the tumor in the retroperitoneal space through retroperitoneal approach in the left lateral position. Under GA, the patient in prone position, midline incision was made. Soft-tissue dissection done. Paraspinal muscles elevated subperiosteally. Three pedicle screws applied on left D12, L1, L2; in D12 and L2 on the right side. Right L1 hemi-laminectomy was performed and right L1 nerve root ligated and sacrificed near the dura. To access the full extent of the tumor in the retroperitoneal space, transverse processes of L2 and L3 on the right side broken with thumb pressure alone. This helped to reach the most anterolateral corner of the tumor, by blunt finger dissection (Fig. 6). At this juncture, we realized that the tumor was accessible from the posterior approach itself and hence avoided the additional exposure to reach the retroperitoneum. Intraoperatively, tumor of size 9 × 6 × 5 cm arising from the right L1 nerve root visualized. Tumor was found to be scalloping and compressing L1 right pedicle and vertebral body (Fig. 7). Tumor excised en masse by marginal resection and the sample was sent for histopathology examination. Contoured connecting rods applied bilaterally and nuts tightened. Bone grafts placed lateral to rods (Fig. 8 and 9).
Histopathological examination revealed a well-circumscribed capsulated neoplasm composed of cells with scant to moderate eosinophilic cytoplasm and uniform elongated spindled wavy nuclei arranged in fascicles. In few areas, the cells are separated by abundant myxoid and hyalinized stroma. Presence of scattered lymphocytes and few mast cells and occasional foamy macrophages were noted. One area in the periphery shows scattered mature ganglion cells with abundant eosinophilic cytoplasm and uniform round nuclei. The features were suggestive of GN. The post-operative period was uneventful and was mobilized from post-operative day 1. At the end of 6-month follow-up, he is pain free and was able to return to his job and performs his activities of daily living independently.

GN is a rare, benign, slow-growing, and well-differentiated tumor composed of ganglion cells and Schwann cells [3]. GNs are a class of peripheral neuroblastic tumors that include three subgroups depending on cellular and extracellular differentiation: Neuroblastomas (most immature, undifferentiated, and with the most malignant potential), ganglioneuroblastomas (intermediate malignant potential), and GNs (fully differentiated, most benign) [4]. Central nervous system GNs are less prevalent and most often occurs in children and young adults [5]. The treatment of choice is surgical resection. Adjuvant systemic chemotherapy and radiotherapy have limited roles due to their benign nature [6]. The long-term prognosis is excellent regardless of tumor location as long as total tumor excision is performed. The surgical approach to the lesion needs to be planned well, dual exposures can be minimized, because of the high morbidity associated with it [7]. Anterior approach has a high risk of injury to the renal vasculature and vena cava. This case report demonstrates the avoidance of a second approach to access the anterolateral aspect of tumor using a posterior exposure to stabilize as well as resect the tumor which was facilitated by removal of L2 and L3 transverse process. The local recurrence has been reported after surgical resection, so regular radiologic follow-up with neurologic examination and radiologic evaluation is necessary even after complete excision [4,8,9].
This report describes a rare case of right L1 nerve root GN of the lumbar spine with retroperitoneal extension. GNs should be considered in the differential diagnosis of a paraspinal mass. Surgical resection is the treatment of choice. Careful surgical planning can reduce the morbidity associated with radical surgical procedures.
Removal of transverse process at L2 and L3 can provide access to anterior structure, thereby limiting the need for dual exposure for resection of the mass.
References
- 1.Geoerger B, Hero B, Harms D, Grebe J, Schiedhauer K, Berthold F. Metabolic activity and clinical features of primary ganglioneuromas. Cancer 2001;91:1905-13. [Google Scholar | PubMed]
- 2.Cugati G, Singh M, Pande A, Ramamurthi R, Balasubramanyam M, Sethi SK, et al. Primary spinal epidural lymphomas. J Craniovertebr Jun Spine 2011;2:3-11. [Google Scholar | PubMed]
- 3.Jeong M, Lee S, Joo KB, Jang KS, Bae J. Ganglioneuroma of lumbar nerve root: A case report. J Korean Soc Radiol 2013;68:153-6. [Google Scholar | PubMed]
- 4.Sun WS, Jung YT, Kim SC, Sim JH. A dumbbell-shaped thoraco-lumbar extradural ganglioneuroma: Case report. J Korean Neurosurg Soc 2002;32:481-4. [Google Scholar | PubMed]
- 5.Pang BC, Tchoyoson Lim CC, Tan KK. Giant spinal ganglioneuroma. J Clin Neurosci 2005;12:967-72. [Google Scholar | PubMed]
- 6.Shephard RH, Sutton D. Dumb-bell ganglioneuromata of the spine with a report of four cases. Br J Surg 1958;45:305-17. [Google Scholar | PubMed]
- 7.Ikard RW. Methods and complications of anterior exposure of the thoracic and lumbar spine. Arch Surg 2006;141:1025-34. [Google Scholar | PubMed]
- 8.Alimoglu O, Caliskan M, Acar A, Hasbahceci M, Canbak T, Bas G. Laparoscopic excision of a retroperitoneal ganglioneuroma. JSLS 2012;16:668-70. [Google Scholar | PubMed]
- 9.Huang Y, Liu L, Li Q, Zhang S. Giant ganglioneuroma of thoracic spine: A case report and review of literature. J Korean Neurosurg Soc 2017;60:371-4. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2025 Gouty Arthritis with Massive Tophaceous Deposits Involving Bilateral Metatarsophalangeal Joints, Surgical Treatment with Excision and Reconstruction – A Case Report
April 1, 2025 Gouty Arthritis with Massive Tophaceous Deposits Involving Bilateral Metatarsophalangeal Joints, Surgical Treatment with Excision and Reconstruction – A Case Report July 30, 2019 The Intraneural Ganglion Cyst of the Tibial Nerve: A Case Report and Review of Literature
July 30, 2019 The Intraneural Ganglion Cyst of the Tibial Nerve: A Case Report and Review of Literature May 10, 2020 Giant Intramuscular Myxoma of Thigh– A Rare Case Report
May 10, 2020 Giant Intramuscular Myxoma of Thigh– A Rare Case Report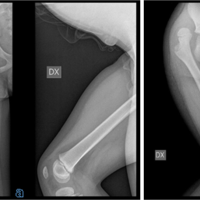 November 10, 2021 Five-years Control after a Delayed Diagnosis of a Traumatic Posterior Hip Dislocation in a 5 years Old Boy- A Case Report
November 10, 2021 Five-years Control after a Delayed Diagnosis of a Traumatic Posterior Hip Dislocation in a 5 years Old Boy- A Case Report