
This report is the first to describe the contemporaneous onset of localized PVNS of the bilateral knee.
Dr. Hiroki Okamura, Department of Orthopedic Surgery, Nihon Koukan Hospital, 1-2-1 Koukandori, Kawasaki-ku, Kanagawa 210-0852, Japan. E-mail: 99okamu99@gmail.com
Abstract
Introduction: Localized pigmented villonodular synovitis (PVNS) is a rare and benign condition of synovial tissue proliferation that affects the joints, tendon sheaths, and bursae. This case report is the first to describe a patient with a diagnosis of localized PVNS of the knee after presentation with bilateral and simultaneous onset of associated knee pain.
Case Report: A 28-year-old Japanese woman presented to our hospital with a 1-year history of bilateral knee pain and right knee locking that started 1 month ago. Magnetic resonance imaging demonstrated a mass lesion in both the anterior compartment of the right knee and in the posterior compartments of the left knee. Arthroscopic resection of the lesions was performed, and the diagnosis of localized PVNS was made by pathological analysis. At the 6-month follow-up, no evidence of recurrence was noted.
Conclusion: This case report describes localized PVNS of the bilateral knee, which is extremely rare. PVNS is a disease requiring surgical resection and should not be overlooked. It should be treated with the possibility of bilateral occurrence in mind.
Keywords: Knee, pigmented villonodular synovitis, arthroscopy, popliteus tendinitis.
Pigmented villonodular synovitis (PVNS) is a rare and benign condition of synovial tissue proliferation that affects the joints, tendon sheaths, and bursae. The typical age of onset is 20–40 years [1]. The etiology is unknown, and whether PVNS should be considered an inflammatory condition or a neoplasm is controversial [1]. Intra-articular PVNS often occurs in the large joints, and 66–80% of the cases occur in the knee joint [2,3]. The condition is classified as either the diffuse type or localized type [4]. The incidence of PVNS is 1.8 cases in 1 million; the localized type accounts for 6% of all cases [2]. To date, six cases of bilateral PVNS have been reported, and one of these cases was the localized type, which is extremely rare [5,6,7,8]. To the best of our knowledge, this case report is the first to describe a patient with bilateral localized PVNS of the knee with simultaneous onset. Patient presentation and diagnosis are discussed in detail. Moreover, this report is a valuable addition to the literature because it documents localized PVNS in the posterior compartment of the knee that could be arthroscopically removed using only the anterior portal.
A 28-year-old woman was referred to our hospital because of bilateral knee pain. The patient reported that her pain started approximately 1 year ago in both the knees, and the feeling of locking in her right knee started 1 month ago. She had no trauma history. Her medical history included thrombocytopenia in early childhood. An orthopedic physical examination of the right knee revealed tenderness from the patella tendon to the anterolateral joint line. Watson-Jones test was positive. Joint effusion, ligament instability, and the McMurray test were all negative. The range of motion was restricted between 0 and 145 degrees because deep extension or flexion exacerbated the pain. The knee injury and osteoarthritis score (KOOS) [9] was 49.4 points. An orthopedic physical examination of the left knee revealed tenderness at the popliteal fossa. The McMurray test was positive for pain, whereas joint effusion and ligament instability were negative. The range of motion was restricted between 0 and 145 degrees because deep extension or flexion exacerbated the pain. The KOOS score was 84.5 points. Imaging studies were performed with plain radiography, including the total length of the lower limbs with weight-bearing, frontal and lateral views of the bilateral knee, and magnetic resonance imaging (MRI) of the bilateral knee. Plain radiography showed normal results bilaterally. For the right knee, MRI showed a mass-like lesion, measuring 24 × 9 mm in the anterior compartment. Homogeneous low-signal foci were detected on T1-weighted scans (Fig. 1a), and heterogeneous low-signal foci with clear borders were depicted on T2-weighted scans at the same site (Fig. 1b). For the left knee, MRI showed a mass-like lesion, measuring 26 × 10 mm in the posterior compartment. Relatively, homogeneous low-signal foci were detected on T1-weighted scans (Fig. 2a), and heterogeneous low-signal foci with clear borders were depicted on T2-weighted scans at the same site (Fig. 2b).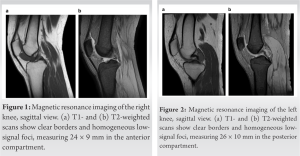
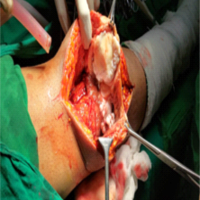
Arthroscopic resection of the right knee lesion was performed using the anterolateral and anteromedial portals. A yellow-brown mass was found in the anterior compartment; this mass had an irregular surface and was continuous to the infrapatellar fat pad (Fig. 3). The continuous part was cut and removed in one piece, and total synovectomy was performed after the removal of the mass. The removed specimen was tested for pathology. The patient was allowed to lead a normal life from the day after the surgery.
Subsequently, 1 month after the right knee surgery, arthroscopic resection of the left knee lesion was performed using the anterolateral and anteromedial portals. A yellow-brown mass was found in the posterior compartment, which had an irregular surface (Fig. 4). One part of the mass was removed; the rest of the mass was shaved and removed. Total synovectomy was performed after the removal of the mass. The removed specimen was tested for pathology. From the day after the procedure, the patient was allowed to continue his or her routine functions. Neither radiotherapy nor chemotherapy was used. Pathologic analysis showed hemosiderin deposits, multinucleated giant cells, histiocytic cells or spindle cells, and lipid-laden macrophages in the bilateral knee lesions (Fig. 5). These results confirmed the diagnosis of bilateral PVNS.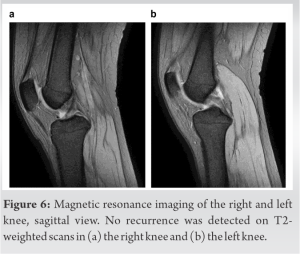
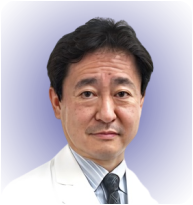
At a 6-month follow-up, pain in the bilateral knees had improved, and there was no recurrence of locking symptoms. Furthermore, no recurrence was observed on MRI (Fig. 6). The KOOS score was 82.1 points for the right knee and 86.3 points for the left knee.
PVNS is a synovial proliferative disorder that often occurs in the large joints, especially the knee joint [2,3]. Histologically, PVNS is characterized by lipid-laden macrophages, multinucleated giant cells, and deposits of hemosiderin within a fibrous stroma, with polyhedral histiocytic or spindle cells and proliferation of round cells [10]. The frequency of PVNS is rare, with 1.8 cases in 1 million [2]. The two categories of PVNS are the diffuse type and localized type, the latter accounting for 6% of cases [3]. Thus far, six cases of bilateral PVNS have been reported – only one of these cases was of the localized type, to our best knowledge [5,6,7,8]. In that case, the pain was localized to the suprapatellar sac bilaterally; symptoms occurred first in the right knee and then in the left knee 4 years later [8]. In our case, the lesions manifested in the anterior and posterior compartments, and symptoms appeared simultaneously and bilaterally. This report is the first case of bilateral PVNS in which symptoms appeared in the anterior and posterior compartments. Clinical findings in PVNS show a presentation with various symptoms, especially for the localized type, which resembles a free body or meniscus tear [11,12,13]. Landon. examined 25 cases of diffuse and localized PVNS and reported that patients had pain (80%), swelling (76%), limited range of motion (52%), locking (16%), and a palpable mass (12%) [11]. Kim et al. examined 11 cases of localized PVNS and reported that patients had locking (64%), swelling (55%), pain (100%), limited range of motion (45%), a palpable mass (64%), and giving way (36%) [12]. In our study, the patient showed joint locking, tenderness at the joint line, and Watson-Jones test positivity in the right knee, which was suspicious for a meniscus injury. For imaging studies, MRI is useful for detecting the area of inflammation with hemosiderin deposits, and lesions have a low intensity on T1-and T2-weighted images for both the diffuse and localized types [14]. However, the diagnosis cannot be made on the basis of MRI alone, and differential diagnosis includes hemangioma, fibroxanthoma, synovial chondromatosis, amyloid or hemophilic arthropathy, and desmoid tumors [10]. Pathologic examination is required for definitive diagnosis [13]. In our case, localized PVNS was diagnosed on the basis of pathology. Untreated PVNS has been reported to cause joint deformity and destruction [15]. The treatment goals are to remove all abnormal synovial tissue, relieve pain, and minimize joint deformity changes. Synovectomy (open, arthroscopic, or both), arthroplasty, and radiation are the common treatments for PVNS [16]. In particular, excision by arthroscopy is useful for the localized type, and even lesions in the posterior compartment can be excised using the posteromedial and posterolateral portals, which is a useful minimally invasive approach [4]. However, use of the posteromedial and posterolateral portals creates a risk of neurovascular damage. A report by Jack et al. was the first to describe localized PVNS in the posterior compartment of the knee that was removed using only the anterior portal by bending the shaver, with no recurrence at 6-month follow-up [17]. Similarly, we were able to achieve complete removal using only anteromedial and anterolateral portals without bending the shaver. This case is one of a few valuable reports of localized PVNS in the posterior compartment of the knee that could be removed using only the anterior portal. Furthermore, in the present case, the tumor and synovial growth were localized and could be completely resected arthroscopically; hence, chemotherapy or radiation therapy was not required.
Bilateral and localized PVNS is extremely rare. Furthermore, to the best of our knowledge, this report is the first to describe contemporaneous onset of localized PVNS of the bilateral knee.
The diagnosis of PVNS can be overlooked because it is rare and presents with a variety of symptoms. In addition, clinicians should be aware that PVNS can be bilateral and should be diagnosed and treated accordingly.
References
- 1.Verspoor FG, van der Geest IC, Vegt E, Veth RP, van der Graaf WT, Schreuder HW. Pigmented villonodular synovitis: Current concepts about diagnosis and management. Future Oncol 2013;9:1515-31. [Google Scholar | PubMed]
- 2.Myers BW, Masi AT. Pigmented villonodular synovitis and tenosynovitis: A clinical epidemiologic study of 166 cases and literature review. Medicine (Baltimore) 1980;59:223-38. [Google Scholar | PubMed]
- 3.Ottaviani S, Ayral X, Dougados M, Gossec L. Pigmented villonodular synovitis: A retrospective single-center study of 122 cases and review of the literature. Semin Arthritis Rheum 2011;40:539-46. [Google Scholar | PubMed]
- 4.Shekhar A, Patil SS, Dixit C, Tapasvi SR. Localized pigmented villonodular synovitis of posterior compartment of the knee. J Orthop Surg (Hong Kong) 2017;25:2309499017727923. [Google Scholar | PubMed]
- 5.Soubai RB, Tahiri L, Ibrahimi A, Chbani L, Harzy T. Bilateral pigmented villonodular synovitis of the knee. Joint Bone Spine 2011;78:219-21. [Google Scholar | PubMed]
- 6.Klammer G, Betz M, Delaloye B, Farshad M, Peter KP. Bilateral diffuse pigmented villonodular synovitis of the knee. J Knee Surg 2013;26(Suppl 1):S67-71. [Google Scholar | PubMed]
- 7.Shah SH, Porrino JA, Green JR, Chew FS. Bilateral pigmented villonodular synovitis of the knee. Rad Case Rep 2015;10:56-60. [Google Scholar | PubMed]
- 8.Fernandes TL, Videira LD, Sasaki SU, Natalino RJ, Almeida AM, Pedrinelli A, et al. Bilateral localized pigmented villonodular synovitis of the knee: Case report and review. Acta Ortop Bras 2018;26:183-6. [Google Scholar | PubMed]
- 9.Roos EM, Lohmander LS. The knee injury and osteoarthritis outcome score (KOOS): From joint injury to osteoarthritis. Health Qual Life Outcomes 2003;1:64. [Google Scholar | PubMed]
- 10.Flandry F, Hughston JC. Pigmented villonodular synovitis. J Bone Joint Surg Am 1987;69:942-9. [Google Scholar | PubMed]
- 11.Landon GC. Pigmented villonodular synovitis of the knee. The results of total arthroscopic synovectomy, partial arthroscopic synovectomy, and arthroscopic local excision. J Bone Joint Surg Am 1992;74:952. [Google Scholar | PubMed]
- 12.Kim SJ, Shin SJ, Choi NH, Choo ET. Arthroscopic treatment for localized pigmented villonodular synovitis of the knee. Clin Orthop Relat Res 2000;379:224-30. [Google Scholar | PubMed]
- 13.Bouguennec N, Meyer A, Graveleau N. Localized form of pigmented villonodular synovitis of the knee: The meniscal mime. Orthop Traumatol Surg Res 2014;100:251-4. [Google Scholar | PubMed]
- 14.Kim RS, Lee JY, Lee KY. Localized pigmented villonodular synovitis attached to the posterior cruciate ligament of the knee. Arthroscopy 2003;19:E32-5. [Google Scholar | PubMed]
- 15.Brahmi M, Vinceneux A, Cassier PA. Current systemic treatment options for tenosynovial giant cell tumor/pigmented villonodular synovitis: Targeting the CSF1/CSF1R axis. Curr Treat Options Oncol 2016;17:10. [Google Scholar | PubMed]
- 16.Stephan SR, Shallop B, Lackman R, Kim TW, Mulcahey MK. Pigmented villonodular synovitis: A comprehensive review and proposed treatment algorithm. JBJS Rev 2016;4:e3. [Google Scholar | PubMed]
- 17.Daoud J, Aouad D, Hassan Y, El Rassi G. Localized pigmented villonodular synovitis of the posterior knee compartment with popliteal vessel compression: A case report of arthroscopic resection using only anterior knee portals. Case Rep Orthop 2018;2018:7532358. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 October 10, 2022 Knee Tuberculosis Presenting As Pigmented villonodular Synovitis
October 10, 2022 Knee Tuberculosis Presenting As Pigmented villonodular Synovitis August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report
August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report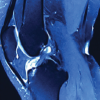 August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain
August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain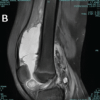 July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates
July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates