
C1 double-door laminoplasty with atlantoaxial fusion acts as a combinatory option for correcting cervical stenosis in an elderly population.
Dr. Jun S Kim, 425 West 59th Street, New York - 10019, United States. E-mail: Jun.Kim@mountsinai.org
Abstract
Introduction: This report describes a novel approach for spinal cord decompression using C1–C2 atlantoaxial fusion with bilateral C1 hinge laminoplasty. Hypothetically, this approach ensures that the stenotic spine is decompressed while simultaneously retaining C1 density for subsequent fixation. Similar techniques have been used in previous case reports for revision procedures or for fusions beyond the atlantoaxial joint.
Case Report: Here, an 83-year-old man with psoriatic arthritis, instability, paresthesia, and motor dysfunction regained strength without symptom progression at 7 months follow-up from cervical spine surgery. This patient had no prior surgical interventions at C1–C2. The pre-operative modified Japanese Orthopedic Association scale score was a 9 preoperatively and a 10 at final post-operative follow-up.
Conclusion: This case provides an alternative to anterior cervical discectomy with fusion, laminectomy, or laminoplasty for progressive myelopathy relief in the geriatric population. Neurosurgeons and orthopedic spine surgeons alike may benefit from utilizing this technique, potentially reducing the occurrence of reoperations or revisions due to instability and or cervical stenosis.
Keywords: Laminoplasty, double-door, laminectomy, atlantoaxial, elderly.
It is imperative that we fully understand the optimal treatment for an aging population, as it is anticipated that older patients with advanced spinal degeneration will increasingly require surgery. For progressive cervical myelopathy, traditional surgical approaches include anterior cervical discectomy with fusion (ACDF), laminectomy, or laminoplasty. While these procedures can provide significant stability and symptom relief, they do have limitations [1,2]. For example, ACDF is associated with adjacent disc degeneration, while laminoplasty is associated with high rates of recurrent stenosis [3,4]. Alternatively, laminectomy removes bone stock at C1–C2 necessitating allograft or occipital cervical fusion (OCF). For these reasons, the development of a fusion with laminoplasty approach has been explored, where C1 density is retained for fusion, providing adequate bone mass for fixation while simultaneously decompressing the stenosis. This technique has been studied extensively for expansive multilevel fusions of lower cervical vertebrae; however, only case reports have analyzed laminoplasty with fusion at the atlantoaxial joint [5,6]. The present study describes the clinical presentation, operative technique, and follow-up of an 83-year-old man who underwent C1 laminoplasty with C1–C2 fusion. To the best of our knowledge, this patient is the oldest individual in the current literature to have successfully undergone this procedure. His consent was obtained for publication.
Pre-operative presentation
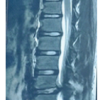
An 83-year-old man with psoriatic arthritis presented with persistent and progressive gait instability, impaired motor dexterity, and hand numbness for 2 months. He underwent C3-C5 laminoplasty for myelopathy with multilevel cervical stenosis and a L2-L4 laminectomy for radiculopathy with lumbar stenosis 4 and 3 years prior, respectively. The patient spent 5 months in a wheelchair prior to consultation due to multiple falls. Examination revealed 4/5 bilateral strength in his deltoids, shoulder external/internal rotators, wrist flexors/extensors, abductor/flexor pollicis brevis, finger extensors, and opponens. He had full biceps/triceps strength bilaterally with intrinsic wasting in his dominant left-hand; left forearm and upper arm showed atrophy. Hand and finger numbness noted bilaterally with positive Hoffmann’s signs. His brachioradialis reflex was inverted bilaterally and biceps/triceps reflexes were brisk (3+). Meniscal and Achilles reflexes could not be elicited and clonus was absent. Babinski signs were equivocal. Light touch sensation was present bilaterally from L1-S1. Lower extremity strength was recorded bilaterally for his gastrocnemius (5/5), quadriceps (5/5), iliopsoas (4/5), tibialis anterior (4/5), and extensor hallucis longus (3/5). The patient’s pre-operative modified Japanese Orthopedic Association (mJOA) scale score was a 9. Cervical spine magnetic resonance imaging revealed an eccentric right pannus posterior to his C1 arch causing cord compression to a 6–7 mm space. A ponticulus posticus was absent and the C1 lateral mass had sufficient height for fusion. Vertebral arteries entered at C6 with normal codominant courses. The subaxial spine was open from prior laminoplasty (Fig. 1).
Surgical summary
Given the presentation, surgical intervention was indicated. A microsurgical C1 laminoplasty and decompression with posterior C1–C2 atlantoaxial fusion (AAF) was performed (Pre-operative Planning-Fig. 2). The patient was placed in the prone position with his head elevated. A midline incision was made from the skull base down to the C2 spinous process with dissection at the midline raphae sparing the extensor muscles. The C1 lamina was exposed and dissected using curettes and Cobb elevators protecting the vertebral arteries superior to the C1 lamina. Next, a translaminar C1 lateral mass screw was drilled to 28 mm (2 mm increments) and a ball-tip probe was used to ensure the lateral mass walls and floors were not violated; a 3.5 mm screw was placed. This process was repeated contralaterally to obtain lateral mass fixation and placement was confirmed (Fig. 3b). The C2 pars were then dissected to the C1–C2 joint. The joint was decorticated bilaterally and demineralized bone matrix was placed into the space to promote facet fusion. The pedicles were then cannulated bilaterally and two 3.5 mm screws (26 mm) were placed into the C2 pedicles. Proper screw placement was confirmed intraoperatively and postoperatively (Fig. 3b-d). Attention was, then, turned to decompressing the spinal cord through laminoplasty at the C1 arch; to visualize this portion of the procedure see additional file 1: Movie 1. Bilateral hinges were made on either side of the C1 lamina while protecting the vertebral arteries. A midline defect was made in the lamina and both sides of the lamina were hinged open. A custom allograft bone block was placed to hold the hinges open which was secured with suturing; both sutures were tied down on either side through a small bone tunnel made on both sides of the hinge. A 3.5 mm titanium rod was then placed across the lateral mass with a pedicle screw between C1 and C2 bilaterally. Set screws were placed, completing the C1–C2 fixation. The remaining marginal C1 lamina and the C2 spinous process, lamina, and pars were decorticated. A combination of autograft, BMP, and demineralized bone matrix were placed across the decorticated bone.
Our patient was discharged on post-operative day 3. After 3 weeks, he presented to clinic in a wheelchair with 4/5 strength in has deltoids, intrinsics, and fingers bilaterally with full strength biceps/triceps, shoulder rotators, and wrist flexors/extensors; brisk reflexes (+3) bilaterally in triceps/biceps with inverted brachioradialis reflex bilaterally. Anteroposterior and lateral radiographs showed properly positioned C1–C2 instrumentation. At 7 weeks follow-up, he noted improvements in strength but had persistent balance issues. Upper extremity strength improved to 5/5 on the right and 4/5 on the left for all muscles with no reflex changes bilaterally. Lower extremities displayed bilateral 5/5 strength for iliopsoas, quadriceps, gastrocnemius, and hamstrings. His tibialis anterior was 5/5 on the right and 4/5 on the left, extensor hallucis longus showed 4/5 strength bilaterally. 4 months postoperatively, his strength continued to improve; he progressed to a walker and began physical therapy. At 7 months, the patient reported no progression of symptoms experienced before his decompression and had improved strength. The final post-operative mJOA score was a 10. Radiographic examination revealed instrumentation in good positioning with signs of fusion (Fig. 4).
Laminoplasty is a widely accepted procedure for spinal cord decompression. To date, there has been a focus on laminoplasty without fusion or with extensive cervical fusion that does not include the atlantoaxial joint. Only two studies, to our knowledge, have focused on laminoplasty with fusion at C1 [5,6]. ACDF, laminectomy, and laminoplasty are the main procedures for correcting C1 stenosis. A paucity of literature has compared these approaches for C1 maladies or for single level fusions. In meta-analyses, multilevel laminectomy with fusion and laminoplasty was shown to have similar post-operative JOA and visual analog pain scores [7,8]. Similarly, multilevel ACDF and laminoplasty resulted in comparable post-operative JOA scores and complication rates [1,9]. However, C1 laminectomy in particular can be unstable, with associated risks for atlas fracture [10]. This is exacerbated by the fact that removing portions of the C1 posterior arch could disrupt the transverse ligament and cervical muscles. Further, an anterior approach at C1 is complicated by complex cervical anatomy with increased morbidity risk. Laminoplasty is not without its disadvantages (e.g., lordosis loss) [2]. However, at the atlas the surgical decision becomes complicated by the anatomy, which is especially true for laminectomy which compromises the C1 posterior arch. The previous studies show that fusion to the occiput reduces range of motion (ROM) [11,12]. Hypothetically, combining C1 arch sparing decompression with fusion for instability correction could stabilize the spine while relieving stenotic symptoms. Kim et al. introduced this approach when they revised a C1–C2 fusion with C1 double-door laminoplasty in a 66-year-old man presenting with myelopathy [5]. Using a posterior bone graft, they fused C1–C2 and at 1-year follow-up their patient achieved marked improvements in pain and paresthesia. Zhu et al. explored a comparable option in a 70-year-old man with numbness and weakness induced by posterior atlantoaxial dislocation that underwent C1 single door laminoplasty with C1–C3 posterior fusion [6]. At 3-years follow-up, he regained cervical ROM (±10° flexion-extension, ±25° rotation) and no longer necessitated ambulation aid. In our intervention, the utilization of C1 laminoplasty with AAF resulted in improved strength and an increased mJOA score at 7-months follow-up for an 83-year-old gentleman. The geriatric population has been shown to have reduced cervical ROM in a healthy state, making the development of a ROM sparing technique following fusion and decompression worthwhile [13]. This point is enhanced by the findings of Yang et al. who demonstrated that OCF patients (n = 483) had increased 30-day complication and predicted revision rates at 1-year and 2-years as compared to AAF (n = 737) patients [14]. However, in a study by Wenning et al., where 44 patients and 52 patients underwent OCF and AAF fusion for fracture, respectively, no differences in Neck Disability Index scores were noted (OCF: 37.4%, AAF: 21.4%; P < 0.05) [15]. Alternatively, in a study analyzing Jefferson fractures, AAF had increased patient reported satisfaction rates compared to patients corrected with OCF; 2/48 and 20/20 AFF; and OCF patients, respectively, reported restricted cervical rotation, flexion, and extension (28-months follow-up) [11]. Further, OCF requires careful planning and execution as it can exacerbate dysphagia if too much flexion is fused. The benefit of our approach is the preservation of C1 bone stock, which can help reduce the need for an occiput-C2 fusion. However, we do acknowledge that a more robust fixation method for the C1 arch (i.e., plate and screw) may provide increased structural stability compared to the suture technique used here. Ultimately, further research into this surgical approach is needed to draw definitive conclusions on its efficacy.
This report demonstrates a novel corrective approach for cervical myelopathy. While technically demanding, C1 laminoplasty with AAF should be considered a strong option for stenosis and instability correction through end of life. Ultimately, fusion with laminoplasty may reduce the need for potential reoperations for progressive instability or stenosis in a vulnerable elderly population.
Cervical myelopathies are a debilitating condition within the elderly population. A combination of AAF with hinge laminoplasty may provide a viable option for instability correction through end of life.
References
- 1.Montano N, Ricciardi L, Olivi A. Comparison of anterior cervical decompression and fusion versus laminoplasty in the treatment of multilevel cervical spondylotic myelopathy: A meta-analysis of clinical and radiological outcomes. World Neurosurg 2015;130:530-6.e2. [Google Scholar | PubMed]
- 2.Cho SK, Kim JS, Overley SC, Merrill RK. Cervical laminoplasty: Indications, surgical considerations, and clinical outcomes. J Am Acad Orthop Surg 2015;26:e142-52. [Google Scholar | PubMed]
- 3.Luo J, Wang H, Peng J, Deng Z, Zhang Z, Liu S, et al. Rate of adjacent segment degeneration of cervical disc arthroplasty versus fusion meta-analysis of randomized controlled trials. World Neurosurg 2015;113:225-31. [Google Scholar | PubMed]
- 4.Weinberg DS, Rhee JM. Cervical laminoplasty. Indication, technique, complications. J Spine Surg 2020;6:290. [Google Scholar | PubMed]
- 5.Kim SW, Lee JH, Lee HW, Oh JK, Kwak YH. New technique for C1 double-door laminoplasty using allograft spacers and titanium miniplate screw fixation: Technical report. J Neurol Surg A Cent Eur Neurosurg 2016;77:155-60. [Google Scholar | PubMed]
- 6.Zhu Y, Wu XX, Jiang AQ, Li XF, Yang HL, Jiang WM. Single door laminoplasty plus posterior fusion for posterior atlantoaxial dislocation with congenital malformation: A case report and review of literature. World J Clin Cases 2020;8:6136-43. [Google Scholar | PubMed]
- 7.Phan K, Scherman DB, Xu J, Leung V, Virk S, Mobbs RJ. Laminectomy and fusion vs laminoplasty for multi-level cervical myelopathy: A systematic review and meta-analysis. Eur Spine J 2017;26:94-103. [Google Scholar | PubMed]
- 8.Liu FU, Yang SD, Huo LS, Wang T, Yang DL, Ding WY. Laminoplasty versus laminectomy and fusion for multilevel cervical compressive myelopathy: A meta-analysis. Medicine (Baltimore) 2016;95:e3588. [Google Scholar | PubMed]
- 9.Xu L, Sun H, Li Z, Liu X, Xu G. Anterior cervical discectomy and fusion versus posterior laminoplasty for multilevel cervical myelopathy. A meta-analysis. Int J Surg 2017;48:247-53. [Google Scholar | PubMed]
- 10.Shimizu T, Otsuki B, Fujibayashi S, Kumamoto S, Hijikata Y, Shimizu Y, et al. Incidence and risk factors of anterior arch fracture of the atlas following C1 laminectomy without fusion. Spine (Phila Pa 1976) 2018;43:667-74. [Google Scholar | PubMed]
- 11.Hu Y, Yuan ZS, Kepler CK, Dong WX, Sun XY, Zhang J. Comparison of occipitocervical and atlantoaxial fusion in treatment of unstable Jefferson fractures. Indian J Orthop 2017;51:28-35. [Google Scholar | PubMed]
- 12.Hidalgo-García C, Lorente AI, López-de-Celis C, Lucha-López O, Malo-Urriés M, Rodríguez-Sanz J, et al. Effects of occipital-atlas stabilization in the upper cervical spine kinematics: An in vitro study. Sci Rep 2021;11:10853. [Google Scholar | PubMed]
- 13.Kuhlman KA. Cervical range of motion in the elderly. Arch Phys Med Rehabil 1993;74:1071-9. [Google Scholar | PubMed]
- 14.Yang DS, Patel SA, DiSilvestro KJ, Li NY, Daniels AH. Postoperative complication rates and hazards-model survival analysis of revision surgery following occipitocervical and atlanto-axial fusion. N Am Spine J 2020;3:100017. [Google Scholar | PubMed]
- 15.Wenning KE, Hoffmann MF. Does isolated atlantoaxial fusion result in better clinical outcome compared to occipitocervical fusion? J Orthop Surg Res 2020;15:8. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Adolescent Cauda Equina Secondary to Traumatic Lumbar Disc Herniation: A Rare Case Report with Review of Literature
August 1, 2026 Adolescent Cauda Equina Secondary to Traumatic Lumbar Disc Herniation: A Rare Case Report with Review of Literature April 1, 2026 A Clinical Experience in Treating Myelopathy Caused by Floating Lamina Resulting from Re-close of the Lamina and Pseudarthrosis at the Lateral Gutter after Cervical Laminoplasty
April 1, 2026 A Clinical Experience in Treating Myelopathy Caused by Floating Lamina Resulting from Re-close of the Lamina and Pseudarthrosis at the Lateral Gutter after Cervical Laminoplasty February 1, 2026 Minimally Invasive Double Loop Suture Technique for Recurrent Acromioclavicular Joint Ganglion Cyst in an Elderly Female: A Case Report
February 1, 2026 Minimally Invasive Double Loop Suture Technique for Recurrent Acromioclavicular Joint Ganglion Cyst in an Elderly Female: A Case Report February 1, 2026 Clinico-Laboratory Correlates of Inflammatory Markers in Elderly Knee Osteoarthritis
February 1, 2026 Clinico-Laboratory Correlates of Inflammatory Markers in Elderly Knee Osteoarthritis