
Although rare osteochondroma should be considered as an differential fiagnosis in young patients presenting with painless or painful swelling over scapula.
Dr. Vasu Jindal, Department of Orthopaedics, MGM Hospital, Navi Mumbai - 410 209, Maharashtra, India. E-mail: vasujindalmzn@gmail.com
Abstract
Introduction: Osteochondroma is a type of cartilaginous tumor. It is the most common benign tumor of axial skeleton usually arising around the knee, proximal humerus, and pelvis. Solitary osteochondroma of the scapula is relatively rare and usually incidental finding accompanied by pain and dysfunction. These lesions can easily be followed radiographically with plain radiograph. Computed tomography (CT) is used to determine the precise location and its relationship with the surrounding soft tissues and enable accurate surgical removal.
Case Report: In this report, we present a rare case of a symptomatic scapular osteochondroma in a 18-year-old male who presented with the complaints of swelling over the left scapula. X-ray showed a bony outgrowth along the posteromedial border of the left scapula. CT scan was done to know extent of the growth. MRI was performed to rule out soft-tissue involvement. Despite the young age of the patient, surgical excision was performed. The outcome was good, the patient noticed disappearance of swelling and a normal profile of the scapula was gained.
Conclusion: We have described a rare case of scapular osteochondroma associated with different signs, symptoms, and positive radiological findings. This lesion was removed surgically, and a follow-up indicated complete symptom relief with no history of recurrence. By reporting this case, we aim to increase the awareness of unusual manifestations of osteochondroma, particularly in terms of site, age of onset, and atypical presenting signs and symptoms.
Keywords: Osteochondroma, scapula, tumor
Osteochondroma are most common benign tumor of bone. They account for 35–46% of all benign tumors of bone [1]. Osteochondromas are usually found on metaphyseal region of long bones such as distal femur, tibia, humerus, and pelvis but are rarely seen on flat bones [2,3,4]. Most common benign tumor of scapula is osteochondroma. About 14.4% of scapular tumors are diagnosed as Osteochondromas and scapula account for 3–4.6% of all osteochondromas [5]. Osteochondromas are usually found in second decade of life when cartilage solidifies into bone and growth generally ceases when skeletal maturity is reached. Incidence of osteochondroma under the age of 30 is more common in males as compared to females [1]. Osteochondroma of ventral aspect of scapula is more common than dorsal aspect of scapula. Osteochondromas are generally asymptomatic but severity ranges from mild pain to severe neurovascular compression depending on the size, location, fracture, bursa formation, and impingement of various structures such as adjacent tendon, blood vessel, nerves, and spinal cord. It is characterized as cartilage-capped osseous stalk with a bone marrow cavity in continuity to underlying bone [6]. There are two different morphological types of osteochondromas: Sessile and pedunculated. The risk for malignant transformation into chondrosarcoma is <1%. Osteosarcoma transformation is very uncommon [3]. The choice of treatment for osteochondroma is surgical excision. Following excision symptoms disappearance and fully recovered functions are generally expected [7]. Here, we report a rare case of atypical, large, solitary, pedunculated, and asymptomatic osteochondroma of dorsal aspect of scapula in a 18 year young male.
A healthy 18-year-old male presented to outpatient clinic with chief complaints of painless protrusion on the left side of his upper back for the past 4 years. Protrubence was first noted by his mother at the age of 13 years which had slowly grown in size till the age of 17 years after which it arrested. No history of trauma was reported. There were no constitutional symptoms of fever or any other illness. He reported that his main reason for visiting was cosmesis. On examination, there was no visible wound, hematoma, scars, or sinuses over the back. The swelling was uniform, rounded, and protrubent, seen, and palpated in the posteromedial region of the left scapula just caudal to medial end of spine (Fig. 1). 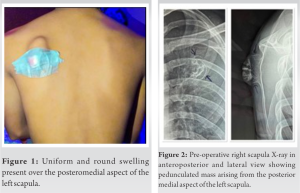 There was no tenderness and local rise of temperature on palpation. There was no restriction in range of movements. There was no evidence of winging of scapula. Neurovascular structures were intact on examining both the upper limbs. Radiograph of the leftscapula was taken in both anterior-posterior view and lateral view was suggestive of bony outgrowth in the posteromedial border of scapula (Fig. 2). Computed tomography (CT) was done to know the extent of the growth (Fig. 3). MRI revealed hyper-intense pedunculated osseous lesion on T2-weighted images measuring 45 × 40 × 40 mm (craniocadual × anteroposterior x transverse) over posteromedial aspect of the left scapula (Fig. 4). Imaging showed solitary protuberance of cortical and medullary bone from the underlying bone which was pathognomonic but histopathology was done to confirm the diagnosis. Histology findings were consistent of osteochondroma. Surgical excision of the swelling was planned for cosmetic reasons and future mechanical complaints. Patient was operated under general anesthesia in prone position. A longitudinal incision parallel to medial scapular border was taken where the protrusion was most prominent. Sharp dissection was carried out to the level of fascia of trapezius muscle and fivers of rhomboid muscles were splitter bluntly for full exposure of the protuberance (Fig. 5). The stalk was excised at the base with osteotome. There was no free body in the space or palpable indurations over the wall (Fig. 6).
There was no tenderness and local rise of temperature on palpation. There was no restriction in range of movements. There was no evidence of winging of scapula. Neurovascular structures were intact on examining both the upper limbs. Radiograph of the leftscapula was taken in both anterior-posterior view and lateral view was suggestive of bony outgrowth in the posteromedial border of scapula (Fig. 2). Computed tomography (CT) was done to know the extent of the growth (Fig. 3). MRI revealed hyper-intense pedunculated osseous lesion on T2-weighted images measuring 45 × 40 × 40 mm (craniocadual × anteroposterior x transverse) over posteromedial aspect of the left scapula (Fig. 4). Imaging showed solitary protuberance of cortical and medullary bone from the underlying bone which was pathognomonic but histopathology was done to confirm the diagnosis. Histology findings were consistent of osteochondroma. Surgical excision of the swelling was planned for cosmetic reasons and future mechanical complaints. Patient was operated under general anesthesia in prone position. A longitudinal incision parallel to medial scapular border was taken where the protrusion was most prominent. Sharp dissection was carried out to the level of fascia of trapezius muscle and fivers of rhomboid muscles were splitter bluntly for full exposure of the protuberance (Fig. 5). The stalk was excised at the base with osteotome. There was no free body in the space or palpable indurations over the wall (Fig. 6).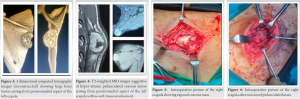 Wound wash was given, fascia of divided muscle was sutured, skin was subsequently closed, and sterile dressing was done. Post-operative course was uneventful and sutures were removed on post-operative day 14. Patient returned to pre-operative normal life 2 weeks after the procedure. On examination, scapulothorasic rythm was symmetrical, no limitations of active range of movements (Fig. 7), or any associated crepitus. Six-month follow-up showed no signs of tumor recurrence both clinically and radiologically. CT showed no residual mass (Fig. 8).
Wound wash was given, fascia of divided muscle was sutured, skin was subsequently closed, and sterile dressing was done. Post-operative course was uneventful and sutures were removed on post-operative day 14. Patient returned to pre-operative normal life 2 weeks after the procedure. On examination, scapulothorasic rythm was symmetrical, no limitations of active range of movements (Fig. 7), or any associated crepitus. Six-month follow-up showed no signs of tumor recurrence both clinically and radiologically. CT showed no residual mass (Fig. 8).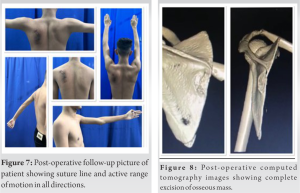
Osteochondromas are benign tumors that commonly affect the proximal humerus, pelvis, and knee but are rarely seen on flat bones like scapula. They are usually asymptomatic and present with cosmetic complaints our difficulty while sleeping in supine position. Osteochondroma is defined as cartilage-capped osseous stalk that arises from the external surface of bone, contains marrow cavity, and grows through endochondral ossification beneath the periosteum [8]. Although osteochondroma of scapula is a rare finding, it accounts for 3–4.6% of all the cases mostly occurring in second decade of life. Ventral surfaces are more commonly involved than dorsal surface. Osteochondroma follows course of bone growth until the closure of physis [6]. Nathan et al. performed a retrospective review of all osteochondroma excisions at their institution from 1994 to 2007. They found that out of eight reported patients, only two patients had lesion arising from dorsal aspect of scapula, five from ventral aspect, and one from inferior acromian. A single patient reported with signs of recurrence and underwent two additional surgical procedures [9]. Salgia et al. presented a case of osteochondroma of dorsal surface of scapulawhose main concern was cosmetic appearance [10]. Nekkanti et al. presented two patients with osteochondroma on the dorsal surface of the scapula. CT scan of the shoulder revealed pedunculated osteochondroma [11]. Our patient presented with dorsal surface scapular osteochondroma with only cosmetic complaints with pedunculated appearance on CT scan and when growth had seized after 17 years of age, for which surgical excision was planned after confirming with clinical, radiological, and histological parameters. Osteochondromas in pediatric age group should be monitored carefully and managed conservatively. Conservative management includes immobilization, physiotherapy, anti-inflammatory, and local anesthetic injections [12]. Osteochondromas which cannot be managed conservatively should be managed by open or arthroscopic excision of tumor. Malignant changes in osteochondroma are very rare but sudden growth may warrant malignant suspicion and should be managed appropriately [5].
We have described a rare case of asymptomatic osteochondroma of dorsal side of scapula with a recognizable protuberance. The lesion was removed surgically, and follow-up indicated no history of recurrence. By reporting this case, we aim to increase awareness regarding unusual manifestation of osteochondroma regarding site and its atypical manifestations.
Diagnosing osteochondroma at an unusual location such as the dorsal aspect of scapula can be challenging and an operative line of management must be undertaken only once the diagnosis is confirmed after a detailed clinical, laboratory, and radiological evaluation. Although it is a rare finding, it is recommended to include osteochondroma in differential diagnosis of swelling and pain over scapula.
References
- 1.Hakim DN, Pelly T, Kulendran M, Caris JA. Benign tumours of the bone: A review. J Bone Oncol 2015;4:37-41. [Google Scholar | PubMed]
- 2.Alabdullrahman LW, Byerly DW. Osteochondroma. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2022. [Google Scholar | PubMed]
- 3.Beauchamp-Chalifour P, Pelet S. Osteochondroma of the scapula with accessory nerve (XI) compression. Case Rep Orthop 2018;2018:7018109. [Google Scholar | PubMed]
- 4.Murphey MD, Choi JJ, Kransdorf MJ, Flemming DJ, Gannon FH. Imaging of osteochondroma: Variants and complications with radiologic-pathologic correlation. Radiographics 2000;20:1407-34. [Google Scholar | PubMed]
- 5.Shahid O, Shahid M, Shaik L, Masud M, Ranjha S. Rare case of osteochondroma on the dorsal aspect of the scapula. Cureus 2021;13:e17051. [Google Scholar | PubMed]
- 6.Fletcher CD, Unni KK, Mertens F, editors. Pathology and Genetics of Tumours of Soft Tissue and Bone. Vol. 4. Lyon, France: IARC Press; 2002. [Google Scholar | PubMed]
- 7.Tepelenis K, Papathanakos G, Kitsouli A, Troupis T, Barbouti A, Vlachos K, et al. Osteochondromas: An updated review of epidemiology, pathogenesis, clinical presentation, radiological features and treatment options. In Vivo 2021;35:681-91. [Google Scholar | PubMed]
- 8.Thompson KG, Dittmer K. Tumors of bone. In: Tumors in Domestic Animals. Hoboken: John Wiley and Sons, Inc.; 2016. p. 356-424. [Google Scholar | PubMed]
- 9.Ratra R, Peshin C. Rare presentation of benign osteochondroma: A case report. J Orthop Case Rep 2020;9:82-5. [Google Scholar | PubMed]
- 10.Frost NL, Parada SA, Manoso MW, Arrington E, Benfanti P. Scapular osteochondromas treated with surgical excision. Orthopedics 2010;33:804. [Google Scholar | PubMed]
- 11.Yadkikar SV, Yadkikar VS. Osteochondroma on dorsal surface of the scapula in 11 year-old child: A case report. Int J Med Res Health Sci 2013;2:305-8. [Google Scholar | PubMed]
- 12.Nekkanti S, Moogali A, Meka A, Nair M. An unusual presentation of osteochondroma on the dorsal surface of the scapula: A review of two patients. J Orthop Case Rep 2018;8:38-41 [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report
February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report December 1, 2025 A Heavy Burden on the Back: Surgical Excision of a Massive Scapular Osteochondroma – A Case Report
December 1, 2025 A Heavy Burden on the Back: Surgical Excision of a Massive Scapular Osteochondroma – A Case Report August 6, 2024 Dorsal Scapular Osteochondroma in a Young Male: A Case Report and Literature Review
August 6, 2024 Dorsal Scapular Osteochondroma in a Young Male: A Case Report and Literature Review