
Synovial hemangioma is a benign lesion, and for good clinical outcome enbloc excision is considered as gold standard.
Dr. Nandlal Bharwani, Department of Orthopaedics, Dr. S. N Medical College, Jodhpur, Rajasthan, India. E-mail: nandlalbharwani21@gmail.com
Abstract
Introduction: Synovial hemangioma is a benign soft-tissue tumor of vascular origin. The knee joint is most common joint affected and with highest incidence noted till date. For diagnosis, of such rare presentation radiological investigations such as digital radiograph and magnetic resonance imaging are of utmost importance, and magnetic resonance imaging being considered as investigation of choice. The gold standard treatment being complete excision of the growth.
Case 1: A 13-year-old boy presented in out-patient clinic with chief complaint of right sided anterior knee pain since 10 months and patient had history of trauma in past. Magnetic resonance imaging of knee joint showed well circumscribed lesion in infra-patellar area (Hoffa’s fat pad), with internal septations present within lesion.
Case 2: A 25-year-old female presented to out-patient clinic with chief complaint of left sided anterior knee pain since 2 year, with no history of prior injury. The magnetic resonance imaging of knee joint showed ill-defined lesion around anterior patella-femoral articulation adherent to quadriceps tendon, internal septations present within lesion. For both cases, en bloc excision was performed and good functional outcome was achieved.
Conclusion: Knee joint synovial hemangioma is rare presentation to orthopedic outdoors, has slight female predominance with pre-existing history of trauma. In the present study, both cases were of patella-femoral type (anterior and infra-patellar fat pad). For such lesions, en bloc excision is gold standard procedure to prevent recurrence, same procedure was followed in our study, and good functional outcome was achieved.
Keywords: Synovial hemangioma, knee joint, soft-tissue tumor, patello-femoral region.
Synovial hemangioma is a benign soft-tissue tumor of vascular origin. Of all the primary tumor of skeleton, hemangioma constitutes merely 1% of all lesions in bone and mostly as an incidental finding. In 1856, Bouchut was first one to present a case of synovial hemangioma, after which in 1973 Moon mentioned 137 patients followed by Price in 1997 mentioned 170 patients showing its rarity [1]. Although, it can be seen at many locations such as ankle, elbow, temporomandibular, interphalangeal joints, and tendon sheaths, but knee joint is most common joint affected and with highest incidence noted till date [2]. The basic pathology in cases of synovial hemangioma being hamartomatous growth or vascular malformations of congenital origin [3,4]. These lesions typically presents with pain, swelling, and limitation of range of motionat later stages [5]. For diagnosis, of such rare presentation radiological investigations such as digital radiograph and magnetic resonance imaging are of utmost importance, and magnetic resonance imaging being considered as investigation of choice [6,7,8]. Although, varied treatment modalities such as arthroscopic laser ablation, excision, embolization, and open en bloc excision. The gold standard treatment being complete excision of the growth [9,10]. In this case series, we present two cases with synovial hemangioma around knee that where managed with total synovectomy in department of orthopedics.
A 13 year old boy presented in out-patient clinic with chief complaint of the right-sided anterior knee pain since 10 months, which gets aggravated with prolong standing, walking, squatting, and cross-leg sitting. The patient had history of trauma 2 years back while playing. On physical examination, soft swelling noted around anterior aspect of knee, with normal range of motion and test for collaterals, meniscus, and cruciate ligaments were inconclusive and no venous engorgement, raised skin temperature limblength discrepancy and effusion were noted. Digital radiograph of knee joint (Antero-posterior and lateral views) (Fig. 1) was inconclusive, thereafter magnetic resonance imaging of knee joint (Fig. 2) showed well circumscribed lesion in infra-patellararea (Hoffa’s fat pad), with internal septations present within lesion. On T1-weighted imaging low to intermediate signal noted whereas on T2-weighted imaging bright signals were noted pain get relived by NSAID’s.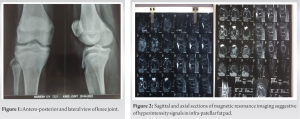
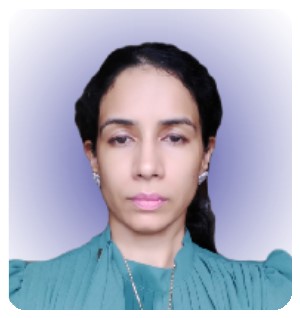
A 25-year-old female presented to out-patient clinic with chief complaint of the left-sided anterior knee pain since 2 year, which gets aggravated with activities of daily routine, squatting, and cross-leg sitting. The patient had no history of trauma. On physical examination, soft swelling noted around anterior aspect of knee, with restricted range of motion (flexion around 90° and test for collaterals, meniscus, and cruciate ligaments were inconclusive) and no limb length discrepancy and effusion were noted. Digital radiograph of knee joint (Antero-posterior and lateral views) (Fig. 3) was inconclusive, thereafter magnetic resonance imaging of knee joint (Fig. 4) showed ill-defined lesion around anterior patella-femoral articulation adherent to quadriceps tendon, internal septations present within lesion. On T1-weighted imaging low to intermediate signal noted whereas on T2-weighted imaging bright signals were noted.  Symptomatic relief was seen after taking NSAID’s. The routine lab investigations in both cases were with in normal limits. For above mentioned case sceniaro’s, open total synovectomy was planned using “medial parapatellar approach” under neuraxial anesthesia and excised sample (Figs. 5 and 6) were sent for histopathological examination (Fig. 7) for confirmatory diagnosis. Informed consent was taken before undergoing any invasive procedure (Table 1).
Symptomatic relief was seen after taking NSAID’s. The routine lab investigations in both cases were with in normal limits. For above mentioned case sceniaro’s, open total synovectomy was planned using “medial parapatellar approach” under neuraxial anesthesia and excised sample (Figs. 5 and 6) were sent for histopathological examination (Fig. 7) for confirmatory diagnosis. Informed consent was taken before undergoing any invasive procedure (Table 1).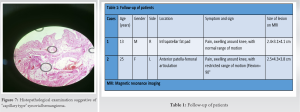
Synovial hemangioma is a form of rare entity, which is not commonly encountered by orthopedic surgeons in outdoors; therefore, delay in definitive diagnosis is commonly seen [11]. Not uncommon in routine clinical practice, second decade of life is a common age group of presentation and seen among young children and adolescents whereas in our study one case with adolescent age group and other with adult age group were present [8,9]. Females are more commonly affected then males, whereas in the present study one male (50%) and one female (50%) were affected [9]. For this condition, trauma was considered as a significant factor after which synovial hemangioma was seen among several studies and in the study by Moon [9] showed that 35% of patients had a history of injury in past and was noted among one (50%) out of two in our study [12]. In our study, characteristic presentation of this condition pain, swelling, and limitation of motion around knee joint all was seen, and none of atypical features of recurrent effusion, hemarthrosis, and leg length discrepancy were noted [9,13]. For preoperative diagnosis, magnetic resonance imaging is of utmost importance showing characteristic appearance of synovial hemangioma that is low/isointense signal changes on T1-wt and hyperintense/bright signal changes on T2-wt images with extent of tumor and involvement of surrounding structures, radiographs in most cases where inconclusive or with nonspecific findings [6,7,8]. In our study, one case with patella-femoral extension was ill defined and that to adherent to overlying quadriceps tendon and second case presented with well circumscribed lesion in Hoffa’s fat pad region, whereas some studies stated that patella-femoral presentation had well circumscribed lesion [14]. For these condition’s, utility of computed tomography (CT)-scan is to rule out bony involvement and none of our cases showed extension into bone; therefore, CT-scan was not performed [15]. For these condition, treatment of choice being en bloc excision of growth and advantages are less chances of recurrence, bleed can be controlled more effectively in comparison to arthroscopic removal and visualization of complete of extent of growth being better with open procedure [7,9,10]. Therefore, prompt diagnosis with radiological investigations, histopathological examination, and open excision holds the key for preventing degenerative joint changes by these lesions [5,9,16]. Till date, data presented by Farkas et al. [5,6,17] showed that open en bloc excision of growth along with synovectomy being the most effective way to prevent recurrence of such rare condition and none of our cases had recurrence [9]. Therefore, same procedure was undertaken in present series using medial parapatellar approach.
Knee joint synovial hemangioma is rare presentation to orthopedic outdoors, has slight female predominance with pre-existing history of trauma. The classification for synovial hemangioma has three forms based on the location popliteal, patella-femoral, and diffuse type and in our study both cases were of patella-femoral type (anterior and infra-patellar fat pad). For such lesions, en bloc excision is gold standard procedure to prevent recurrence, same procedure was followed in our study and good functional outcome was achieved.
The presentation of synovial hemangioma is rare in orthopedic clinics, en bloc excision is considered as the gold standard to decrease the chances of recurrence.
References
- 1.Bouchut E. Tumor erectile de 1’ articulation du genou. Gaz Hop 1856;29:379-81. [Google Scholar | PubMed]
- 2.Bruns J, Eggers-Stroeder G, von-Torklius D. Synovial hemangioma- a rare beingn synovial tumor. Report of four cases. Knee Surg Sports Traumatol Arthrosc 1994;2:186-9. [Google Scholar | PubMed]
- 3.Dalmonte P, Granata C, Fulcheri E, Vercellino N, Gregorio S, Magnano G. Intra-articular venous malformations of the knee. J Pediatr Orthop 2012;32:394-8. [Google Scholar | PubMed]
- 4.Kroner K, Fruensgaard S. Synovial hemangioma of the knee joint. Arch Orthop Trauma Surg 1989;108:253-4. [Google Scholar | PubMed]
- 5.Cotten A, Flipo RM, Herbaux B, Gougeon F, Lecomte-Houcke M, Chastanet P. Synovial hemangioma of the knee: A frequently misdiagnosed lesion. Skeletal Radiol 995;24:257-61. [Google Scholar | PubMed]
- 6.Greenspan A, McGahan JP, Vogelsang P, Szabo RM. Imaging stratergies in the evaluation of soft-tissue hemangiomas of the extremities: Correlation of the findings of plain radiography, angiography, CT, MRI and ultrasonography in 12 histologically proven cases. Skeletal Radiol 1992;21:11-8. [Google Scholar | PubMed]
- 7.Pinar H, Bozkurt M, Baktiroglu L, Karaoglan O. Intra-articular hemangioma of the knee with meniscal and bony attachment. Arthroscopy 1997;13:507-10. [Google Scholar | PubMed]
- 8.Price NJ, Cundy PJ. Synovial hemangioma of the knee. J Pediatr Orthop 1997;17:74-7. [Google Scholar | PubMed]
- 9.Moon NF. Synovial hemangioma of the knee joint. A review of previously reported cases and inclusion of two new cases. Clin Orthop 1973;90:183-90. [Google Scholar | PubMed]
- 10.Aynaci O, Ahmetoglu A, Reis A, Turhan AU. Synovial hemangioma in the Hoffa’s fat pad (case report). Knee Surg Sports Traumatol Arthrosc 2001;9:355-7. [Google Scholar | PubMed]
- 11.Akgun I, Kesmezacar H, Ogut T, Dervisoglu S. Intra-articular hemangioma of the knee. Arthroscopy 2003;19:E17. [Google Scholar | PubMed]
- 12.Neel MD, Toy PC, Kaste SC, Jenkins JJ, Daw N, Rao BN. Painfull limp in a 10-year old boy. Clin Orthop 2003;410:326-33. [Google Scholar | PubMed]
- 13.Okahashi K, Sugimoto K, Iwai M, Tanaka M, Fujisawa Y, Takakura Y. Intra-articular synovial hemangioma; a rare cause of knee pain and swelling. Arch Orthop Trauma Surg 2004;124:571-3. [Google Scholar | PubMed]
- 14.Maeyama A, Sacki K, Hamasaki M, Kato Y, Naito M. Deformation of the patella-femoral joint caused by synovial hemangioma: A case report. J Pediatr Orthop B 2014;23:346-9. [Google Scholar | PubMed]
- 15.Greenspan A, Azouz EM, Matthews J, Decarie JC. Synovial hemangioma: Imaging features in eight histologically proven cases, review of the literature, and differential diagnosis. Skeletal Radiol 1995;24:583-90. [Google Scholar | PubMed]
- 16.Del Notaro C, Hug T. Intra-articular hemangioma of the knee as a cause of knee pain. Arthroscopy 2003;19:E12-4. [Google Scholar | PubMed]
- 17.Farkas C, Morocz I, Szappanos L, Szepesi K. The importance of arthroscopy in diagnosing synocial hemangioma of the knee joint. Acta Chir Hung 1998;37:17-22. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 November 10, 2023 Two Discrete Intra-articular Synovial Hemangiomas of a Knee Joint Presenting as Chronic Knee Pain
November 10, 2023 Two Discrete Intra-articular Synovial Hemangiomas of a Knee Joint Presenting as Chronic Knee Pain August 1, 2026 Not All Red Flags Indicate Malignancy: A Case Report of a Benign Lipoma Mimicking Soft-tissue Sarcoma
August 1, 2026 Not All Red Flags Indicate Malignancy: A Case Report of a Benign Lipoma Mimicking Soft-tissue Sarcoma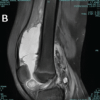 July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates
July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates July 1, 2026 Atypical Presentation of MRSA Septic Arthritis with Concurrent Pyomyositis of the Calf Muscles in an Immunocompetent Adult
July 1, 2026 Atypical Presentation of MRSA Septic Arthritis with Concurrent Pyomyositis of the Calf Muscles in an Immunocompetent Adult