
The symptomatic coracoclavicular joint should always be ruled out while examining a painful shoulder and it can be managed conservatively too with intra-articular steroids.
Dr. Harmeet Kaur, Department of Radiodiagnosis, All India Institute of Medical Sciences, Bathinda, Punjab, India. E-mail: kaurh28@yahoo.com
Introduction: Actual coracoclavicular (CC) joint is a rare finding and usually incidental. It is mostly asymptomatic, but few cases have been reported in which there was associated shoulder pain and even brachial plexus neuralgia. It is not to be confused with CC ligament which is a well-known anatomical entity.
Case Report: Here, we present a case of symptomatic CC joint treated at our hospital. A 50-year-old man presented to the outdoor patient department of our hospital with a history of acute on chronic pain in the left shoulder. The pain used to be dull/aching, occurring after some activity and usually relieved on rest. On local examination, mild tenderness was present around the coracoid process. The pain was aggravated on flexion and external rotation of the shoulder. X-ray of the shoulder revealed the presence of a CC joint. It was confirmed by non-contrast computed tomography of the shoulder. Ultrasound-guided injection of local anesthetic and steroid was given in the CC joint, providing instant pain relief to the patient. At 1-year follow-up, the patient is asymptomatic and continuing his daily routine activities.
Conclusion: Although CC Joint is a rare entity, its role in causing symptoms is unrefutable. Conservative treatment should be tried before surgical excision. More awareness regarding this joint and its pathology is required for identification and diagnosis.
Keywords: Coracoclavicular joint, shoulder pain, coracoclavicular ligament.
Coracoclavicular (CC) joint is a rare and often incidental finding and was considered an asymptomatic entity for a long time [1]. It is a diarthrodial joint, present between the Conoid process on the undersurface of the clavicle above and the superior projection of the coracoid process below. The prevalence of this joint ranges from 2.7% to 7%, depending on the type of study, that is, radiological, skeletal, and cadaveric [2, 3]. As per a morphometric study, the prevalence of CC joint in India is 5.6% [4]. Although the CC joint is asymptomatic in most cases, recent literature suggests otherwise [5, 6]. Here, we present an interesting case of symptomatic CC joint that we encountered in our hospital.
A 50-year-old man presented to the outdoor patient department of our hospital with a history of chronic pain in the left shoulder for 5 years. The pain used to be dull/aching, occurring after some activity and usually relieved on rest. The patient did not seek any medical consultation for it. The pain in the shoulder was now aggravated after the patient tried doing push-ups 10 days back as part of a friendly bet. He went to a physical therapist and was diagnosed with muscle strain and was advised Ice packs, NSAIDs, and rest for 1 week. He did not get any relief and then presented to us. The patient did not have any comorbidities including diabetes mellitus. On local examination, mild tenderness was present around the coracoid process. The pain was aggravated on flexion and external rotation of the shoulder and was terminally restricted. An X-ray of the shoulder was done, which revealed the presence of the CC joint (Fig. 1).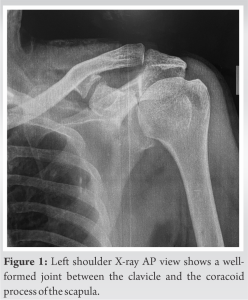 It was followed by non-contrast computed tomography of the shoulder, and on 3D reconstruction, degenerative changes could be appreciated in the joint (Fig. 2).
It was followed by non-contrast computed tomography of the shoulder, and on 3D reconstruction, degenerative changes could be appreciated in the joint (Fig. 2). Ultrasound-guided injection of local anesthetic and steroid (10 mg triamcinolone) was given in the CC joint, providing instant pain relief to the patient [7]. At 1-year follow-up, the patient is asymptomatic and continuing his daily routine activities without any restriction in shoulder movements.
Ultrasound-guided injection of local anesthetic and steroid (10 mg triamcinolone) was given in the CC joint, providing instant pain relief to the patient [7]. At 1-year follow-up, the patient is asymptomatic and continuing his daily routine activities without any restriction in shoulder movements.
The clinical implications of the CC joint are not mentioned in primary textbooks. Hence, there is a dearth of knowledge about its presence in the radiodiagnosis and orthopedic community. Therefore, many such cases go undiagnosed, thus leading to the under-reporting of this entity Although now this joint has been studied extensively globally, there is no case of symptomatic CC joint reported from India. Many mechanisms have been suggested that can cause symptoms in the case of CC Joint. It may hamper the shoulder joint dynamics, which are otherwise maintained due to the laxity of the CC ligament complex [8]. Reduced space between the acromion and supraspinatus due to the decreased upward movement of the acromion can cause impingement symptoms such as painful arc [9]. The most prevalent pathology was brachial plexus involvement, followed by CC Joint osteoarthritis and supracoracoid impingement, according to a meta-analysis that included 17 case reports with problematic CC joints [5]. In our case, the shoulder pain of the patient was unresponsive to NSAIDS and ice therapy. Administration of intra-articular steroid injection in the CC joint provided instantaneous and long-lasting pain relief to the patient. Hence, the pathology can be attributed to the arthritic changes in the CC joint. Although most reports suggest surgical excision to be the definitive treatment modality for the resolution of symptoms [10], a trial of conservative methods must be done before surgery. We recommend more research and reporting of symptomatic cases of CC Joints so that the spectrum of clinical manifestations of this joint can be explored and the burden of undiagnosed cases can be reduced.
Although CC joint is a rare entity but its role in causing symptoms is unrefutable. Conservative treatment should be tried before surgical excision. More awareness regarding this joint and its pathology is required for identification and diagnosis.
The CC joint can be one of the rare sources of shoulder pain. Although the CC joint is asymptomatic in most cases, sometimes arthritic changes may develop in it and cause pain. It merits a trial of conservative methods, like intra-articular steroids before the joint excision surgery.
References
- 1.Cockshott WP. The coracoclavicular joint. Radiology 1979;131:313-6. [Google Scholar]
- 2.Yammine K, Assi C. The coracoclavicular joint. A systematic review and meta-analysis. Homo 2016;67:150-62. [Google Scholar]
- 3.Nehme A, Tricoire JL, Giordano G, Rouge D, Chiron P, Puget J. Coracoclavicular joints. Reflections upon incidence, pathophysiology and etiology of the different forms. Surg Radiol Anat 2004;26:33-8. [Google Scholar]
- 4.Das SS, Mahajan A, Vasudeva N. Morphometric study of clavicular facet of coracoclavicular joint in adult Indian population. J Clin Diagn Res 2016;10:AC08-11. [Google Scholar]
- 5.Singh VK, Singh PK, Trehan R, Thompson S, Pandit R, Patel V. Symptomatic coracoclavicular joint: Incidence, clinical significance and available management options. Int Orthop 2011;35:1821-6. [Google Scholar]
- 6.Spinnato P, Chiesa AM. Coracoclavicular joint: The other joint in the shoulder. Rheumatolog y (Oxford) 2021;keab491. [Google Scholar]
- 7.Schuh A, Seehaus F, Onyemaechi NO, Hönle W. Osteoarthritis in a symptomatic coracoclavicular joint. Glob Med Ther 2018;3:1000106. [Google Scholar]
- 8.Frassetto F. Three cases of articulation coraro-clavicolare watchlist radiographically on living. Chir Organi Mov 1921;5:116-24. [Google Scholar]
- 9.Faraj AA. Bilateral congenital coracoclavicular joint. Case report and review of the literature. Acta Orthop Belg 2003;69:552-4. [Google Scholar]
- 10.Gibbs S, Merriman JA, Sorenson E, Hatch GF 3rd. Surgical excision of a symptomatic congenital coracoclavicular joint. Orthopedics 2014;37:e836-8. [Google Scholar]






