
Alternate types of treatment available for neck pain like high velocity low amplitude manipulation should be done only by professional registered chiropractors and should be avoided in cases of patients who already have an underlying disc degeneration and patients with clinically proven spondylitis.
Dr. Vishnu Vikraman Nair, Department of Orthopaedics and Spine Surgery, Bombay Hospital and Medical Research Institute, Mumbai, Maharashtra, India. E-mail: vishnunair212@gmail.com
Abstract
Introduction: In this case report, we question the safety associated with high velocity manipulations of the cervical spine. These procedures do not frequently cause catastrophic adverse effects but few and rare case reports like this make us aware about the possible complications of the maneuvers.
Case Report: This case report presents an uncommon presentation of acute neurodeficit to a 57-year-old male following a neck manipulation by a barber in the saloon which recovered partially with Intravenous steroid therapy but required active intervention surgically to treat his complete symptomatology. The magnetic resonance imaging (T2-weighted) showed a high signal intensity within the spinal cord at the C4C5 level (cord edema). Here, we discuss the possible mechanism of injury and the need to educate the lesser common risks of performing such sudden and forceful maneuvers.
Conclusion: This case report is a reminder that people should be careful while trying alterative types of therapy which use forceful neck manipulations to relieve pain as this maneuver could cause injuries to the disc complex especially when the patient already has a disc prolapse which is asymptomatic, causing the disc to fail again making it symptomatic.
Keywords: Manipulation, neurodeficit, cervical spine, paraparesis.
Manipulation of the cervical spine is a very common procedure done professionally by chiropractors and by non-skilled people like barbers especially in India. Cervical spine manipulation is considered relatively safe when performed by registered Chiropractors as mentioned in a study performed in UK [1]. These procedures do not frequently cause catastrophic adverse effects but few and rare case reports like this make us aware about the possible complications of the maneuvers. In this case report, we present a rare case of paraparesis following neck manipulation by a non-registered person.
A 57-year-old male presented to the outpatient ward with complaints of tingling numbness in upper and lower limbs with mild progressive gait imbalance for 2 weeks. On further history taking, it was established that the patient was apparently alright 2 weeks back when he visited the local barber for a head massage and toward the end of the massage the barber had manipulated his neck sideways with rotation and lateral flexion forcefully after which he experienced an electric shock like sensation along his upper and lower back. Patient was unable to use his upper and lower limbs to full power after which he visited a hospital and was given intravenous steroid (Methylprednisolone). On his presentation to us, neurological examination of cranial nerves and lower limb was normal but upper limb motor examination showed weakness in hand and wrist extension bilaterally. On sensory testing, there was a patchy level of paresthesia along the right upper arm along C5 dermatome and a patch of hyperesthesia in the right lower limb. Reflexes were normal in both upper and lower limb. He had neck pain and gait imbalance on presentation to us in the outpatient department with a VAS score of 8/10. Imaging The magnetic resonance imaging (MRI) (Fig. 1) of the cervical spine revealed multilevel degenerative changes and multiple osteophytes from C3 to C7 level. There was indentation on the cord with an annular tear and disc extrusion at the level of C4-C5 level with a high signal change in the cord at the C4-C5 level. X-rays showed loss of cervical lordosis and degenerative changes (Fig. 2).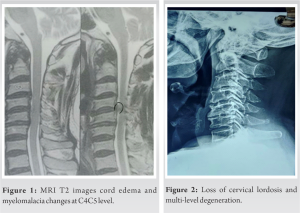 No other significant findings were seen in the whole spine screening imaging. MRI brain was also unremarkable. Management Patient was planned for a single level anterior cervical decompression and cage placement at C4-C5 level for the symptoms persisting and to decompress the spinal cord to prevent any clinical neurological deterioration. After an anterior discectomy and decompression, two huge fragments of extruded disc were found to be lying behind the posterior longitudinal ligament and inside the spinal canal indenting on the spinal cord (Fig. 3). Those fragments were removed safely, and a stand-alone titanium cage was placed with locally harvested autograft from marginal osteophytes to enhance fusion at the C4–C5 level after discectomy (Fig. 4). The patient was stable vitally after surgery and within a week had a normal gait while walking and was able to do all daily activities.
No other significant findings were seen in the whole spine screening imaging. MRI brain was also unremarkable. Management Patient was planned for a single level anterior cervical decompression and cage placement at C4-C5 level for the symptoms persisting and to decompress the spinal cord to prevent any clinical neurological deterioration. After an anterior discectomy and decompression, two huge fragments of extruded disc were found to be lying behind the posterior longitudinal ligament and inside the spinal canal indenting on the spinal cord (Fig. 3). Those fragments were removed safely, and a stand-alone titanium cage was placed with locally harvested autograft from marginal osteophytes to enhance fusion at the C4–C5 level after discectomy (Fig. 4). The patient was stable vitally after surgery and within a week had a normal gait while walking and was able to do all daily activities.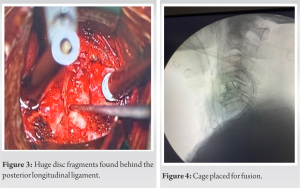
Forceful neck manipulation is done commonly by barbers and some massage therapists to provide rapid relief in pain. High velocity low amplitude (HVLA) is also performed by chiropractors to give relief in neck pain after which patients usually do not experience any adverse effects most of the time even though the risks of this procedure have been mentioned in the literature [2,3,4,5,6]. Thiel et al. described in a prospective study on patients of chiropractors that the immediate risk after the treatment was development of lightheadedness, dizziness, and fainting [1]. Tingling and numbness were more common adverse effects after 7 days of the HVLA treatment. Gouveia et al. [5] also mentioned chiropractic treatment caused only mild transient adverse effects and nothing more. This case gives a rarer outlook into the treatment taken by large number of people to avoid taking medications while they can be treated in a systematic manner. Motor weakness in upper limb, gait imbalance, paresthesia, and hypoesthesia present had to be treated with utmost care. The literature mentions about Brown Sequard type of incomplete injury to the cord following chiropractic care, out of which two also had an epidural bleed injury [6]. The most practical explanation for what happened with our case is that, in a degenerative spine with spondylosis features, when an asymmetric force in the form of flexion and rotation is applied, it could cause failure of the anterior and middle columns in the spine causing the annulus to rupture and cause the fragmented disc to get retro pulsed posteriorly into the spinal canal. This can be confirmed with our MRI findings and intraoperative findings. Existing spinal canal stenosis and the sagittal diameter of the canal are a predisposing factor for cord compression and myelopathy [7,8,9]. Many authors also mention about how cervical spondylosis can also be a preexisting risk factor for developing neurodeficit [10,11].
This case report is a reminder that people should be careful while trying alterative types of therapy which use forceful neck manipulations to relive pain as this maneuver could cause injuries to the disc complex especially when the patient already has a disc prolapse which is asymptomatic, causing the disc to fail under tension, making it symptomatic. Patients could develop neurovascular injuries which might require to be managed with steroid injections and in a few patients with an anterior discectomy and fusion procedure to further prevent any compression on the spinal cord.
Treatment of neck pain could be a long process and patients who do not get instant relief, prefer taking alternate types of treatment like manipulation. Close clinical and radiological examination should be done and possible risk factors of such treatments should be explained to the patients.
References
- 1.Thiel HW, Bolton JE, Docherty S, Portlock JC. Safety of chiropractic manipulation of the cervical spine: A prospective national survey. Spine (Phila Pa 1976) 2007;32:2375-8; discussion 2379. [Google Scholar | PubMed]
- 2.Gibbons P, Tehan P. HVLA thrust techniques-what are the risks? Int J Osteopath Med 2006;9:4-12. [Google Scholar | PubMed]
- 3.Stevinson C, Ernst E. Risks associated with spinal manipulation. Am J Med 2002;112:566-71. [Google Scholar | PubMed]
- 4.Ernst E, Canter PH. A systematic review of systematic reviews on spinal manipulation. J R Soc Med 2006;99:192-6. [Google Scholar | PubMed]
- 5.Gouveia LO, Castanho P, Ferriera JJ. Safety of chiropractic intervention: A systematic review. Spine 2009;34:E405-13. [Google Scholar | PubMed]
- 6.Paciaroni M, Bogousslavsky J. Cerebrovasular complications of neck manipulation. Eur Neurol 2009;61:112-8. [Google Scholar | PubMed]
- 7.Torg JS, Naranja RJ Jr., Pavlov H, Galinat BJ, Warren R, Stine RA. The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-14. [Google Scholar | PubMed]
- 8.Sasaki T, Kadoya S, Iizuka H. Roentgenological study of the sagittal diameter of the cervical spinal canal in normal adult Japanese. Neurol Med Chir (Tokyo) 1998;38:83-8; discussion 88-9. [Google Scholar | PubMed]
- 9.Sani S, Boco T, Deutsch H. Cervical stenosis presenting with acute Brown-Sequard syndrome: Case report. Spine (Phila Pa 1976) 2005;30:E481-3. [Google Scholar | PubMed]
- 10.Ueyama T, Tamaki N, Kondoh T, Miyamoto H, Akiyama H, Nagashima T. Non-traumatic acute paraplegia associated with cervical disk herniation: A case report. Surg Neurol 1999;52:204-6; discussion 206-7. [Google Scholar | PubMed]
- 11.Tator CH, Duncan EG, Edmonds VE, Lapczak LI, Andrews DF. Changes in epidemiology of acute spinal cord injury from 1947 to 1981. Surg Neurol 1993;40:207-15. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Delayed Esophageal Perforation 14 Years after Cervical Anterior Decompression and Fusion: A Case Report
April 1, 2026 Delayed Esophageal Perforation 14 Years after Cervical Anterior Decompression and Fusion: A Case Report March 1, 2026 Acute Cauda Equina Syndrome Due to Primary Lumbar Spinal Hydatid Cyst: A Rare Case
March 1, 2026 Acute Cauda Equina Syndrome Due to Primary Lumbar Spinal Hydatid Cyst: A Rare Case March 1, 2026 Silently Gradually Progressing Paraparesis Pott’s Spine Lumbar Vertebra with Bilateral Psoas Abscess
March 1, 2026 Silently Gradually Progressing Paraparesis Pott’s Spine Lumbar Vertebra with Bilateral Psoas Abscess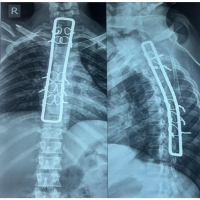 August 6, 2024 Use of Hartshill Rectangle with Sublaminar Wiring in Spinal Stabilization of D4-D5 Fracture Dislocation with Acute Spinal Cord Injury – A Cost-Effective Treatment
August 6, 2024 Use of Hartshill Rectangle with Sublaminar Wiring in Spinal Stabilization of D4-D5 Fracture Dislocation with Acute Spinal Cord Injury – A Cost-Effective Treatment