
The importance of clinical examination in identification of a rare disease and proper pre-operative planning to avoid intraoperative complications and to achieve excellent post-operative outcome.
Dr. A Arul Prasanna, Department of Orthopaedics, JJ Arul Hospital, Dindigul - 624 002, Tamil Nadu, India. E-mail: arulprasanna2018@gmail.com
Abstract
Introduction: Ochronosis is a rare metabolic disorder, characterized by accumulation of homogentisic acid in the connective tissues due to the lack of the enzyme homogentisic acid oxidase. The musculoskeletal manifestation of alkaptonuria is black pigmentation of cartilage of the knee and the hip leading to arthropathy.
Case Report: In this article, we report three patients with involvement of hip, knee, and spine, but with more severe involvement of the hips. Bilateral hip arthroplasty was done in one out of the three patients.
Conclusion: Being a rare disorder and often missed, the functional outcome of hip arthroplasty in these patients is similar to primary osteoarthritis. The importance lies in correct diagnosis and anticipation of intraoperative difficulties.
Keywords: Ochronosis, arthroplasty, arthropathy, metabolic arthropathy, alkaptonuria.
Alkaptonuria is a rare metabolic disorder, with an autosomal recessive inheritance. It is due to the deficiency of the enzyme homogentisate oxidase. Males and females are equally affected. This disorder results in the accumulation of homogentisic acid in the connective tissues, hence the term Ochronosis [1,2]. Homogentisic acid gets deposited in all the cartilages such as sclera, menisci, intervertebral discs, pinnae, articular surfaces, and tendons which results in progressive degeneration and arthropathy. Hip, knee, and spine are the usually involved joints, there may be involvement of cardiovascular, respiratory, genitourinary, and ocular systems [2]. Herniation of disc in the thoracolumbar levels with osteophyte formation is common [3]. The urine darkens when exposed to air or reducing agents [4]. The treatment is mainly symptomatic and supportive. Surgical treatment in the form of arthroscopic debridement, synovectomy, and total joint replacement can achieve alleviation of pain and painless range of motion (ROM). Being a rare entity, the diagnosis may be missed during initial examination or the surgeon may be surprised to find black pigmentation while proceeding for arthroplasty, during which some surgeons may take a biopsy and postpone the arthroplasty after a histological diagnosis, while some may proceed with the planned procedure, but without recognizing the anesthetic and orthopedic complications, leading to devastating complications. Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Case 1
A 68-year-old female came with the complaints of pain in her left hip for the past 7 years, associated with limping and could walk only with a support for the past 2 years. On clinical examination, there was black discoloration of sclera, nails, and palm (Fig. 1). Urine showed black discoloration on leaving it in the sun. Patient had restriction of abduction, adduction, and internal rotation movements in the left hip with flexion being limited terminally (0–80° possible). The ipsilateral knee joint had restriction of flexion (0–90° possible). Radiographs showed sclerosis of femoral head, erosion of acetabulum, and complete loss of joint space of the left hip. The right hip showed only partial loss of joint space with no other significant arthritis changes. There was fusion of lower thoracic and upper lumbar vertebra with formation of osteophytes (Fig. 2). The patient could not bend forwards or backwards, implying a fused spine. Under spinal anesthesia, which was achieved with difficulty due to the fused spine, we performed a posterior approach to the left hip with patient in lateral decubitus. The trochanteric bursa was pigmented, as well as the joint capsule and the femoral head (Fig. 3). The head was delivered with difficulty after releasing the capsule. The femoral head was deformed and had bluish black pigmentation. The head was sent for histopathological examination along with the other tissue samples which were taken earlier in the procedure. The acetabulum was reamed carefully along with the curettage of the cysts. Uncemented total hip arthroplasty was performed, the movements were adequate and the joint was stable. Post-operative radiograph showed prosthesis in satisfactory position (Fig. 4). Active ROM was started on post-operative day 1. The technical difficulties in this case include spinal anesthesia, acceptable anteversion of the acetabular cup, curettage of the cysts in the floor, release of the capsule to regain motion, and prevention of intraoperative periprosthetic fractures. Patient was followed up to 1 year and had no complications.
Urine showed black discoloration on leaving it in the sun. Patient had restriction of abduction, adduction, and internal rotation movements in the left hip with flexion being limited terminally (0–80° possible). The ipsilateral knee joint had restriction of flexion (0–90° possible). Radiographs showed sclerosis of femoral head, erosion of acetabulum, and complete loss of joint space of the left hip. The right hip showed only partial loss of joint space with no other significant arthritis changes. There was fusion of lower thoracic and upper lumbar vertebra with formation of osteophytes (Fig. 2). The patient could not bend forwards or backwards, implying a fused spine. Under spinal anesthesia, which was achieved with difficulty due to the fused spine, we performed a posterior approach to the left hip with patient in lateral decubitus. The trochanteric bursa was pigmented, as well as the joint capsule and the femoral head (Fig. 3). The head was delivered with difficulty after releasing the capsule. The femoral head was deformed and had bluish black pigmentation. The head was sent for histopathological examination along with the other tissue samples which were taken earlier in the procedure. The acetabulum was reamed carefully along with the curettage of the cysts. Uncemented total hip arthroplasty was performed, the movements were adequate and the joint was stable. Post-operative radiograph showed prosthesis in satisfactory position (Fig. 4). Active ROM was started on post-operative day 1. The technical difficulties in this case include spinal anesthesia, acceptable anteversion of the acetabular cup, curettage of the cysts in the floor, release of the capsule to regain motion, and prevention of intraoperative periprosthetic fractures. Patient was followed up to 1 year and had no complications.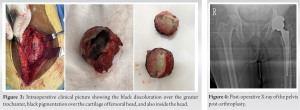
Case 2
A 36-year-old male presented to our outpatient department with the complaints of pain in both hips for the past 3 years, associated with limping. On clinical examination, patient had restriction of extension and internal rotation in both the hips. Radiographs showed sclerosis of femoral head, complete loss of joint space of both the hips. Under spinal anesthesia, we performed a posterior approach to the left hip with patient in lateral decubitus. There was pigmentation of joint capsule and the femoral head. The head was delivered with difficulty after releasing the capsule. The femoral head had bluish black pigmentation (Fig. 5).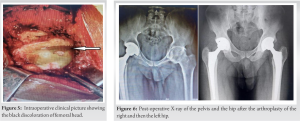 The head was sent for histopathological examination along with the other tissue samples which were taken earlier in the procedure. The diagnosis was established with the HPE reports. Uncemented total hip arthroplasty was performed for the right hip and then for the left hip after an interval of 60 days. Post-operative radiograph showed prosthesis in satisfactory position (Fig. 6). Active ROM was started on post-operative day 1 for both the procedures. Post-operative period was uneventful. Patient was followed up for 5 years and had no complications.
The head was sent for histopathological examination along with the other tissue samples which were taken earlier in the procedure. The diagnosis was established with the HPE reports. Uncemented total hip arthroplasty was performed for the right hip and then for the left hip after an interval of 60 days. Post-operative radiograph showed prosthesis in satisfactory position (Fig. 6). Active ROM was started on post-operative day 1 for both the procedures. Post-operative period was uneventful. Patient was followed up for 5 years and had no complications.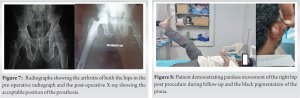
Case 3
A 56-year-old male came with the complaints of pain in both the hips, and with restriction of movements in the right hip more than the left hip (Fig. 7). Clinical examination revealed black pigmentation of the pinna, which made us suspect ochronosis (Fig. 8). Radiographs showed arthritis of both the hips with sclerosis and reduction of joint space bilaterally (Fig. 7). Uncemented total hip arthroplasty was performed on the right hip. Post-operative period was uneventful and an active range of movements was started on post-operative day 2. Patient was followed up for 2 years and showed no complications, but had restriction of movements on the left hip and has been planned for arthroplasty for the left hip.
Most of the patients with alkaptonuria are asymptomatic. Symptoms arise around 3rd–5th decade of life. The musculoskeletal manifestations encountered commonly are arthritis of large joints, rupture of tendons, spondylolisthesis, angular deformities of spine, and pathological fractures. Radiographs show calcification of pubic symphysis, intervertebral discs, cardiac valves, and cartilage. The damage of cartilage leads to destruction of joint leading to pain and limping. Almost half of these patients undergo replacement surgery [5]. Intraoperative diagnosis of ochronosis is not uncommon, due to the presence of dark bursa, cartilages, and synovium. The literature regarding joint arthroplasty especially the hip for Ochronotic arthritis is limited [5,6]. If the operating surgeon was familiar to intraoperative management of ochronosis arthropathy, the outcome of joint replacement was good [7]. There are some reports of the surgeons having deferred the planned procedure and postponing the definitive procedure until making a histopathological diagnosis; however, their results were satisfactory as well [7,8,9]. Pandey et al. assessed the anesthetic concerns in ochronosis. They emphasized that these patients need a pre-operative diagnosis and a thorough pre-operative systemic evaluation. Although, spinal anesthesia is a good option, ochronotic changes in the lumbar spine might challenge the regional anesthesia. They concluded that general anesthesia is a safe alternative with proper pre-operative preparation [10,11]. Spencer et al. concluded from a follow-up for 12 years that the survival rate of the prosthesis is same as that of primary arthroplasty [5]. Harun et al. had demonstrated excellent result after arthroplasty [7]. Makela and Korkala had shown good results after performing bilateral hip arthroplasty [10]. Some surgeons recommended removal of anterior capsule to prevent recurrence of disease [12,13]. Pachore et al. advocated preservation og capsule from their study in 12 patients with a follow-up of 3–24 years [14]. We performed release of capsule depending upon the pathology and restriction of movements. Various studies recommend uncemented arthroplasty if the bone stock is adequate and to proceed with cemented components if the bone stock is inadequate radiologically or macroscopically. Good functional outcome was obtained with uncemented arthroplasty.
The importance of thorough clinical evaluation will help in preoperative diagnosis of this inflammatory arthropathy and will help the surgeon and anesthetist plan accordingly to prevent intraoperative and post-operative complications [14]. The intraoperative diagnosis of ochronosis will not alter the type of prothesis being used. Excellent outcomes have been obtained with cementless hip arthroplasty systems.
Being a rare disorder, thorough clinical evaluation will help in proper planning of the surgery in these patients by anticipating difficulties in anesthesia, recognizing associated spine involvement and achieving better post-operative outcomes in these patients. The above cited clinical and intra operative images can be used for correlation in day to day clinical practice.
References
- 1.Dom K, Pittevils T. Ochronotic arthropathy: The black hip. Case report and review of the literature. Acta Orthop Belg 1997;63:122-5 [Google Scholar | PubMed]
- 2.Acar MA, Erkocak OF, Aydin BK, Altan E, Senaran H, Elmadağ NM. Patients with black hip and black knee due to ochronotic arthropathy: Case report and review of literature. Oman Med J 2013;28:448-9. [Google Scholar | PubMed]
- 3.Farzannia A, Shokouhi G, Hadidchi S. Alkaptonuria and lumbar disc herniation. Report of three cases. J Neurosurg 2003;98(1 Suppl):87-9. [Google Scholar | PubMed]
- 4.Collins EJ, Hand R. Alkaptonuric ochronosis: A case report. AANA J 2005;73:41-6. [Google Scholar | PubMed]
- 5.Spencer JM, Gibbons CL, Sharp RJ, Carr AJ, Athanasou NA. Arthroplasty for ochronotic arthritis: No failure of 11 replacements in 3 patients followed 6-12 years. Acta Orthop Scand 2004;75:355-8. [Google Scholar | PubMed]
- 6.Mazoochy H, Razi M. Knee and hip joint replacement surgery in a patient with ochronotic arthropathy: Surgical tips. Arch Bone Jt Surg 2018;6:577-81. [Google Scholar | PubMed]
- 7.Harun M, Hayrettin Y, Serhat M, Cuneyt M, Fırat F, Ufuk O. A rare cause of arthropathy: An ochronotic patient with black joints. Int J Surg Case Rep 2014;5:554-7. [Google Scholar | PubMed]
- 8.Siavashi B, Zehtab MJ, Pendar E. Ochronosis of hip joint; A case report. Cases J 2009;16:9337. [Google Scholar | PubMed]
- 9.Mohapatra S, Biswas T, Das S, Saxena A. Ochronosis of the hip joint: Differential diagnosis of inflammatory arthropathy with lytic lesion. Indian J Clin Biochem 2014;29:112-3. [Google Scholar | PubMed]
- 10.Makela A, Korkala O. Hip arthroplasty for alkaptonuric ochronosis: A case report. Acta Orthop Scand 1986;57:171-2. [Google Scholar | PubMed]
- 11.Pandey R, Kumar A, Garg R, Khanna P, Darlong V. Perioperative management of patient with alkaptonuria and associated multiple comorbidities. J Anaesthesiol Clin Pharmacol 2011;27:259-61. [Google Scholar | PubMed]
- 12.Cebesoy O, Isik M, Subasi M, Kaya A, Bilgin F, Kaya O. Total hip replacement for an ochronotic patient: A technical trick. Am J Case Rep 2014;15:27-30. [Google Scholar | PubMed]
- 13.Fernando OS, Supreeth N, David GD, Borja L, Ricardo L. An unusual case of bilateral ochronotic arthropathy of the hip successfully managed by a staged bilateral total hip replacement-an insight with a surgical note. J Orthop Case Rep 2018;8:11-4. [Google Scholar | PubMed]
- 14.Pachore JA, Shah VI, Upadhyay S, Shah K, Sheth A, Kshatriya A. Primary hip arthroplasty for the treatment of alkaptonuric hip arthritis: 3-to 24-year follow-ups. Arthroplasty 2019;1:8. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2025 Ochronotic Arthropathy of the Shoulder – A Rare Case Report
January 1, 2025 Ochronotic Arthropathy of the Shoulder – A Rare Case Report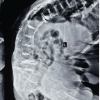 November 1, 2025 A Dark Turn in the OR: Incidental Discovery of Ochronosis during Trauma Surgery: A Case Report
November 1, 2025 A Dark Turn in the OR: Incidental Discovery of Ochronosis during Trauma Surgery: A Case Report December 1, 2024 Blackish Discoloration of Articular Cartilage during Total Knee Replacement; a Case Report
December 1, 2024 Blackish Discoloration of Articular Cartilage during Total Knee Replacement; a Case Report February 10, 2024 Arthroplasty in Ochronotic Arthropathy: 3 Replacements in a Single Patient with a Long-term Follow-up of 11 Years
February 10, 2024 Arthroplasty in Ochronotic Arthropathy: 3 Replacements in a Single Patient with a Long-term Follow-up of 11 Years