
Bosworth ankle injuries are complex and inherently prone for irreducibility, where timely open reduction and stabilization restores joint function in acute and delayed presentations. In chronic neglected cases ankle arthrodesis could be considered as the salvage procedure to restore plantigrade foot.
Dr. Sitsabesan Chokkalingam, Department of Trauma and Orthopaedics, SRIHER, Pour, Chennai, Tamil Nadu, India. E-mail: sabesan101@gmail.com
Abstract
Introduction: Bosworth ankle injuries (BAIs) are rare talocrural dislocations with bi or trimalleolar fractures. Attempted closed reduction fails due to incarcerated fibular fracture behind the distal tibia. The diagnostic delay and failed attempts to restore anatomical reduction result in significant ankle swelling, compromised skin, and imminent compartment syndrome. In neglected cases with unreduced dislocation over months, capsular and tendo-Achilles contracture, additional disuse osteoporosis, adds to the complexity of surgical management. In chronic and neglected cases, literatures have no clear consensus of opinion on the type of surgical intervention and on the extent of optimization. In acute BAI, open reduction is recommended but the soft-tissue swelling may warrant staged internal fixation, after temporary external fixation.
Case study: In this retrospective study we present the clinico-radiological outcome of surgically treated delayed presentation of BAI. The primary fixation in delayed cases and the role of reverse talar dome osteotomy for fusion in the chronic neglected case will be discussed. Patients were aged between 25 and 62 years, presented with isolated closed ankle injuries. Initial X-rays were consistent with BAI. The delay in presentation ranges from 2 to 49 days. All had open reduction and stabilization of the ankle. Chronic neglected case with 7 months delay had “Reverse talar dome osteotomy” for reduction of the neglected dislocation and proceeded for the primary fusion. Patients gained back their full weight-bearing mobility at an average of 12 weeks following delayed fixation. Fused ankle gained full weight-bearing mobility at 5 months post-operative period.
Conclusion Bosworth type of ankle dislocations are difficult injuries for closed reduction. Early diagnosis and recognition of fibular impingement require open reduction of the joint. In cases of delayed presentation, it could be challenging. Even after open reduction, a staged procedure may be warranted based on the soft tissue status. Osteotomy for joint reduction and primary fusion remains a viable option in neglected cases with an ultimate aim to regain plantigrade foot for mobility.
Keywords: Bosworth ankle fracture, Irreducible ankle dislocation, Neglected ankle fracture, Primary ankle fusion, Reverse talar dome osteotomy.
Bosworth ankle injuries (BAIs) occur infrequently with a prevalence of 1.6% among all ankle fractures [1]. It was first described by Bosworth in 1947 [2] as an irreducible dislocation of the ankle with fractured fibula getting incarcerated behind the distal tibial metaphysis [4]. In this challenging injury, open reduction of the talocrural dislocation is inevitable to achieve reduction that prevents pressure necrosis of the anterior skin, vascular damage, neurologic impairment, and chondral damage. The supination external rotation injury [3,4] may often result in disrupted syndesmosis in addition to fibular fracture. Perry [4] showed a sequential tear of the tibiofibular ligament in addition to the capsule and interosseous membrane. Downey [7] described an irreducible posterior dislocation with an intact fibula an atypical variant of BAI. X-rays can be studied for the initial diagnosis. Khan and Borton described the Axilla sign [5] for these uncommon injures. BAI is one of the exceptional conditions, where the pre-reduction computed tomography (CT) scan can be an useful tool [8] . The orthopedic instinct of repeated closed reduction often worsens the swelling and compromises the situation. The better outcome of BAI with the early intervention (1) needs diagnostic suspicion in irreducible [6] ankle dislocations.
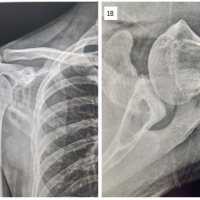
Retrospective study of five cases reported between 2016 and 2020 with delayed presentation of BAI. The age range was 25–62 years (Table 1-patient demographics) with a time delay (2–28 days, mean 11.2 days) for definitive treatment.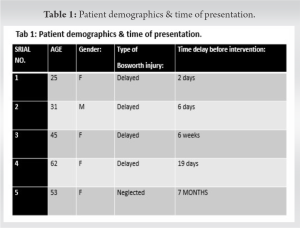 The chronic neglected case had 7 months delay. The mechanisms of injury were twist and fall, and RTA resulting in isolated closed fracture-dislocation in all these cases. Clinical symptoms were pain, swelling, and reduced mobility of their ankle for daily activities. On assessment, they had signs of ankle fracture dislocation with no signs of associated compartment syndrome. Chronic lipodermatosclerosis was encountered in the neglected case. The neurovascular status were intact. The X-ray on presentation (Fig. 1a, 2a, 3a) showed bi- or trimalleolar fracture with joint disruption and the proximal end of fracture fibula behind the posterior tibia. All these patients had a single attempt of closed reduction at their initial consultation.
The chronic neglected case had 7 months delay. The mechanisms of injury were twist and fall, and RTA resulting in isolated closed fracture-dislocation in all these cases. Clinical symptoms were pain, swelling, and reduced mobility of their ankle for daily activities. On assessment, they had signs of ankle fracture dislocation with no signs of associated compartment syndrome. Chronic lipodermatosclerosis was encountered in the neglected case. The neurovascular status were intact. The X-ray on presentation (Fig. 1a, 2a, 3a) showed bi- or trimalleolar fracture with joint disruption and the proximal end of fracture fibula behind the posterior tibia. All these patients had a single attempt of closed reduction at their initial consultation. In view of the delayed presentation, we avoided reattempts for closed reduction. After optimization, open reduction and operative stabilization was achieved in all the four cases except in the chronic neglected presentation. The posterolateral approach favored the reduction and a Hohmann retractor helped in the disimpaction of the incarcerated fibula. The Weber B, C fracture was stabilized with a lateral buttress plate and an additional tricortical syndesmotic screw through the plate to increase the screw pull-out strength, a modification (Figs. 1b and 2b), we consistently followed in this series of cases. The curvilinear medial incision exposed the medial fragment. Deltoid ligament interposition was found in two cases. Medial reducibility was checked even before fixing the lateral side in every single case. Lag screw principle was used on the medial side using 4 mm partially threaded compression screws where feasible and in one case due to the fragment size simply k-wires were used for fixation. The neglected case of BAI with 7 months delay was diagnosed in a 53-year-old non diabetic lady. She had an isolated closed injury to her left ankle following a road traffic accident.
In view of the delayed presentation, we avoided reattempts for closed reduction. After optimization, open reduction and operative stabilization was achieved in all the four cases except in the chronic neglected presentation. The posterolateral approach favored the reduction and a Hohmann retractor helped in the disimpaction of the incarcerated fibula. The Weber B, C fracture was stabilized with a lateral buttress plate and an additional tricortical syndesmotic screw through the plate to increase the screw pull-out strength, a modification (Figs. 1b and 2b), we consistently followed in this series of cases. The curvilinear medial incision exposed the medial fragment. Deltoid ligament interposition was found in two cases. Medial reducibility was checked even before fixing the lateral side in every single case. Lag screw principle was used on the medial side using 4 mm partially threaded compression screws where feasible and in one case due to the fragment size simply k-wires were used for fixation. The neglected case of BAI with 7 months delay was diagnosed in a 53-year-old non diabetic lady. She had an isolated closed injury to her left ankle following a road traffic accident. After native splinting for 12 weeks she developed superficial ulceration over the medial malleolus. She became wheelchair-bound for her activities of daily living. Except for a high BMI of 39, a local examination showed a healed ulcer over the medial malleolus. The surrounding skin had secondary lipodermo sclerosis with the ankle in equino-valgus deformity. ROM at her ankle was 20° with further plantar flexion of 20° in the non-anatomical plane. She had severe stiffness of subtalar movements, but no distal neurological or vascular deficit. X-rays of the left ankle AP and lateral view (Fig. 3a-c) confirmed the posterolateral unreduced talocrural dislocation with trimalleolar fracture.
After native splinting for 12 weeks she developed superficial ulceration over the medial malleolus. She became wheelchair-bound for her activities of daily living. Except for a high BMI of 39, a local examination showed a healed ulcer over the medial malleolus. The surrounding skin had secondary lipodermo sclerosis with the ankle in equino-valgus deformity. ROM at her ankle was 20° with further plantar flexion of 20° in the non-anatomical plane. She had severe stiffness of subtalar movements, but no distal neurological or vascular deficit. X-rays of the left ankle AP and lateral view (Fig. 3a-c) confirmed the posterolateral unreduced talocrural dislocation with trimalleolar fracture. The lateral side was a Weber C type with posteriorly incarcerated fibular fracture behind the tibia. Attempted callus response was noticed on the lateral side. The talus appeared to have normal radiological features with no signs of subtalar joint pathology. Charcot’s neuropathy was excluded using the nerve conduction studies. Her distal arterial flow studies were normal and a venous Doppler excluded deep vein thrombosis. Pre-operative calcaneal pin traction was a sham reduction procedure that helped to reduce the soft-tissue tension. Antero medial approach was used to address the dislocated ankle, as the distal part of tibia was entirely stuck in front of the talus. The non-anatomical plane of tibiotalar interface blunted the distal tibial plafond to become a convex surface. Additional posterior soft-tissue contracture plus the proximal migration of the talus posed a greater challenge for reduction. A reverse dome osteotomy of the talus allowed reduction of the convex distal tibial surface. With foot in plantigrade position, primary ankle arthrodesis was achieved with three partial threaded screws (Fig. 3d). The post-operative plaster cast was changed over to weight-bearing air cast boot at 6 weeks and extended for 6 months.
The lateral side was a Weber C type with posteriorly incarcerated fibular fracture behind the tibia. Attempted callus response was noticed on the lateral side. The talus appeared to have normal radiological features with no signs of subtalar joint pathology. Charcot’s neuropathy was excluded using the nerve conduction studies. Her distal arterial flow studies were normal and a venous Doppler excluded deep vein thrombosis. Pre-operative calcaneal pin traction was a sham reduction procedure that helped to reduce the soft-tissue tension. Antero medial approach was used to address the dislocated ankle, as the distal part of tibia was entirely stuck in front of the talus. The non-anatomical plane of tibiotalar interface blunted the distal tibial plafond to become a convex surface. Additional posterior soft-tissue contracture plus the proximal migration of the talus posed a greater challenge for reduction. A reverse dome osteotomy of the talus allowed reduction of the convex distal tibial surface. With foot in plantigrade position, primary ankle arthrodesis was achieved with three partial threaded screws (Fig. 3d). The post-operative plaster cast was changed over to weight-bearing air cast boot at 6 weeks and extended for 6 months.
Following open reduction and stabilization, patients gained back full eight-bearing mobility at an average of 12 weeks (range 8–16 weeks). Range of movement was average dorsiflexion of 20° (range 10–25), plantar flexion 20° (range 20–30°). Ankle fusion case with plantigrade foot gained back mobility at 6 months post-operative period. The VAS score for pain improved. Mobility and ankle stability were restored in all these cases.
BAI and its pathoanatomy were first described by D M Bosworth. A dislocation occurs in 21–36% of ankle injury cases but only the BAI are inherent for irreducibility [1]. Posterior displacement of fibula occurs after both osseous and ligamentous injury [4]. In the sequential damage [4], rotational forces continue, to cause weber B [2] or C type fracture. In addition to syndesmotic diastasis [1], the fractured fibula gets incarcerated behind the posterior tibia. About 70% of BAI have associated posterior malleolus fracture and an avulsion type of medial malleolus, rarely an adduction type of medial malleolar fracture [7] or a pilon fracture [11]. Atypical variant of BAI also includes intact fibular posterior displacement with ankle dislocation [12]. Patients with a displacement of the fibula behind the posterior tibial rim can have associated extra-incisural (Bartoníček/Rammelt) type 1 injury. The displacement between the posterior malleolar fragment and the tibia were associated with type 2 and 3 posterior malleolar fractures [11,20]. Other various soft-tissue causes for irreducibility includes interposition of the deltoid ligament on the medial side, tibialis posterior tendon on the fibular fracture site, in the syndesmotic joint or through the interosseous membrane [10,11].
Initial assessment and investigations in BAI
The orthopedic instinct of reduction and splinting before X-rays is challenging and doubtful in these cases. Acute swollen ankle poses a serious challenge in the assessment of bony landmarks. Pre-reduction ankle AP X-rays with excess tibiofibular overlap, lateral view with fibula behind the tibial flare, disrupted syndesmosis and a dislocated ankle are signs suggestive of BAI. “Axilla sign” as described [14] is unique for this injury in the mortise view, which is the cortical density in the axilla of the medial tibial plafond. A further CT evaluation in BAI shows the type of posterior malleolar fracture, the extent of incarceration [13] associated osteochondral lesion, and other bony causes of irreducibility. There is no clear consensus about pre-operative CT scans despite the proven benefits, but the surgical delay should be avoided [15]. Quigley’s method of closed reduction is meant for ankle fracture-dislocations, but with BAI a modified, lateral and anterior force over the proximal fibula with counterforce on the tibia [4] has been reported. Repeated attempts of closed reduction in BAI can compromise the blood supply and may cause post-operative compartment syndrome [13]. Compartment syndrome being rare after ankle fractures, the incidence with BF is 5.7% [02] Once diagnosed delay in operative reduction beyond 24 h [15] has poor prognosis. In BAI, open medial fracture is often due to its subcutaneous position. The skin and soft-tissue necrosis on the medial side can gets worsened when unreduced. BAI with vascular compromise needs urgent surgical intervention [17]. Transient vascular insult with pre-operative CT angiogram showing tapered flow with non-visualization of the dorsalis pedis or plantar arteries [17] got corrected just by open reduction. The literature on BAI suggests open surgery through a posterolateral approach, to lever the incarcerated fibula from the posterior tibial tubercle and for lateral side plate fixation [19]. Two-staged procedure [2] with a spanning external fixator could be used to hold the reduced ankle joint [7]. Definitive fixation of lateral malleolus could be using a locking or non-locking plate but often diastasis needs trans-syndesmotic fixation [7] with two quadricortical screws, as single or no screw shows poor prognosis and persistent ankle pain. Posterior malleolar fractures need either lag screw or plate fixation.
Neglected Bosworth fracture dislocation ankle
Misdiagnosis and late presentations delay the intervention and, hence, carry the risk of irreducibility and early onset arthritis [18] Literatures strongly highlight the need for open reduction but lacks consensus on the extended time frame [17,18] . Primary ankle fusion has been reported for a single case who refused initial surgery [18]. In the absence of clear consensus of opinion on neglected BAI with extensive chondral damage, primary ankle fusion surgery would be an option, to regain stable mobility.
BAI, when presented with delay, open reduction still remains feasible and stabilization restores ankle joint mobility. When salvage is near impossible, primary ankle fusion is a viable option. Reverse talar dome osteotomy achieves reduction in neglected posterolateral ankle dislocation with BAI scenario. It restores plantigrade foot, redesign the articular surface for fusion and regain stability for weight-bearing mobility.
BAI is inherently impossible for closed reduction. In delayed cases, even open reduction can be challenging but feasible. In neglected cases when reduction is impossible, primary ankle arthrodesis remains a viable option to restore weight-bearing stable mobility.
References
- 1.Won Y, Lee GS, Hwang JM, Park IY, Song JH, Kang C, et al. Improved functional outcome after early reduction in Bosworth fracture-dislocation. Foot Ankle Surg 2019;25:798-803. [Google Scholar | PubMed]
- 2.Bosworth DM. Fracture-dislocation of the ankle with fixed displacement of the fibula behind the tibia. J Bone Joint Surg Am 1947;29:130-5. [Google Scholar | PubMed]
- 3.Bartonícek J, Fric V, Svatos F, Lunácek L. Bosworth-type fibular entrapment injuries of the ankle: The Bosworth lesion. A report of 6 cases and literature review. J Orthop Trauma 2007;21:710-7. [Google Scholar | PubMed]
- 4.Perry CR, Rice S, Rao A, Burdge R. Posterior fracture-dislocation of the distal part of the fibula. Mechanism and staging of injury. J Bone Joint Surg Am 1983;65:1149-57. [Google Scholar | PubMed]
- 5.Khan F, Borton D. A constant radiological sign in Bosworth’s fractures: “The Axilla sign”. Foot Ankle Int 2008;29:55-7. [Google Scholar | PubMed]
- 6.Cappuccio M, Leonetti D, Di Matteo B, Tigani D. An uncommon case of irreducible ankle fracture-dislocation: The “Bosworth-like” tibio-fibular fracture. Foot Ankle Surg 2017;23:e1-4. [Google Scholar | PubMed]
- 7.Downey MW, Motley TA, Kosmopoulos V. The Bosworth ankle fracture: A retrospective case series and literature review. EC Orthopaedics 2016;3:243-53. [Google Scholar | PubMed]
- 8.Wright SE, Legg A, Davies MB. A contemporary approach to the management of a Bosworth injury. Injury 2012;43:252-3. [Google Scholar | PubMed]
- 9.Delasotta LA, Hansen RH 3rd, Sands AK. Surgical management of the posterior fibula fracture dislocation: Case report. Foot Ankle Int 2013;34:1443-6. [Google Scholar | PubMed]
- 10.Ashhurst AP, Bromer RS. Classification and mechanism of fractures of the leg bones involving the ankle. Based on a study of three hundred cases from the Episcopal hospital. Arch Surg 1922;4:51-129. [Google Scholar | PubMed]
- 11.Kostlivý K, Bartoníček J, Rammelt S. Posterior malleolus fractures in Bosworth fracture-dislocations. A combination not to be missed. Injury 2020;51:537-41. [Google Scholar | PubMed]
- 12.Williams AD, Blue M, Douthit C, Caroom C. Bosworth dislocation without associated fracture. Case Rep Orthop 2018;2018:7284643. [Google Scholar | PubMed]
- 13.Ren W, Hu YC, Lu JK. Rare variants of Bosworth fracture-dislocation: Bosworth fracture-dislocation with medial malleolus adduction type fracture. Chin J Traumatol 2019;22:120-4. [Google Scholar | PubMed]
- 14.Khan F, Borton D. A constant radiological sign in Bosworth’s fractures: “The Axilla sign”. Foot Ankle Int 2008;29:55-7. [Google Scholar | PubMed]
- 15.Won Y, Lee GS, Hwang JM, Park IY, Song JH, Kang C, et al. Improved functional outcome after early reduction in Bosworth fracture-dislocation. Foot Ankle Surg 2019;25:798-803. [Google Scholar | PubMed]
- 16.Ellanti P, Hammad Y, Grieve PP. Acutely irreducible ankle fracture dislocation: A report of a Bosworth fracture and its management. J Emerg Med 2013;44:e349-52. [Google Scholar | PubMed]
- 17.Yeoh CS, Tan GM. Bosworth fracture-dislocation of the ankle: A case report. J Orthop Surg (Hong Kong) 2013;21:249-52. [Google Scholar | PubMed]
- 18.Bartonícek J, Fric V, Svatos F, Lunácek L. Bosworth-type fibular entrapment injuries of the ankle: The Bosworth lesion. A report of 6 cases and literature review. J Orthop Trauma 2007;21:710-7. [Google Scholar | PubMed]
- 19.Foldager CB, Barckman J, Robertsen K, Borris LC. Bosworth fracture dislocation of the ankle: -Two case reports with perioperative illustration. Trauma Case Rep 2018;17:39-42. [Google Scholar | PubMed]
- 20.Bartoníček J, Rammelt S, Kostlivý K. Bosworth fracture complicated by unrecognized compartment syndrome: A case report and review of the literature. Arch Orthop Trauma Surg 2022;142:1435-41. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 August 10, 2022 A Rare Case Report of Primary Hydatid Disease of the Scapula – an Unforeseen Diagnosis!
August 10, 2022 A Rare Case Report of Primary Hydatid Disease of the Scapula – an Unforeseen Diagnosis! October 12, 2013 Tophus of the Pubis Bone: A Case Report
October 12, 2013 Tophus of the Pubis Bone: A Case Report December 10, 2023 Analogy of Lumbar Disc: Retained, Residual, or Recurrent Disc?
December 10, 2023 Analogy of Lumbar Disc: Retained, Residual, or Recurrent Disc? January 10, 2017 A Case of Chronic Inflammation of the Ankle Joint with Subtle Signs of Inflammation: A Rare Presentation of Tuberculosis Ankle
January 10, 2017 A Case of Chronic Inflammation of the Ankle Joint with Subtle Signs of Inflammation: A Rare Presentation of Tuberculosis Ankle