
On presentation of a patient with a thigh mass, medical practitioners must consider the possibility of a pseudoaneurysm with subsequent referral to the regional vascular surgical center.
Dr. Ibrahim Inzarul Haq, Department of Trauma and Orthopaedics, George Eliot Hospital, Nuneaton CV10 7DJ, United Kingdom. E-mail: Ibrahimhaq@hotmail.com
Abstract
Introduction: Non-traumatic pseudoaneurysms are very rare but should be considered as a differential diagnosis on patients presenting with a thigh mass.
Case Presentation: We present an extremely unusual case of a 70-year-old patient who presented with clinical features of a soft-tissue sarcoma of the thigh that instead was proven to be a non-traumatic pseudoaneurysm. There was also incidental finding of bilateral leg non-traumatic pseudoaneurysms.
Conclusion: Medical practitioners must consider the possibility of non-traumatic pseudoaneurysm in patients that present with a thigh mass.
Keywords: Pseudoaneurysm, non-traumatic, thigh, sarcoma.
Pseudoaneurysms are damaged blood vessels which lead to the collection of blood between the tunica media and tunica adventitia of the artery with a direct communication into the lumen [1]. It is commonly caused iatrogenically – for example, after cardiac catheterization or by traumatic injuries to the femoral artery by intravenous drug users. However, further causes such as neoplastic, infective, inflammatory, or rare connective tissue disorders such as Behcet’s disease [2] are also possible. The most common location for pseudoaneurysms is in the femoral arteries, but they are also frequently found in the carotid and radial arteries. The management of pseudoaneurysms can vary depending on size, site, and if there are clinical features of rupture. Small pseudoaneurysms are treated conservatively or with thrombin injection, but larger pseudoaneurysms are at risk of rupture and are usually managed surgically with stents or surgical repair/ligation. Non-traumatic pseudoaneurysms are exceptionally rare and this is the first case of concurrent non-traumatic bilateral leg pseudoaneurysms.
A 70-year-old man initially presented to the emergency department with a 10-month history of a large left thigh lesion. Due to the COVID-19 pandemic, this patient did not seek advice from his personal general practitioner. This lesion had started to rapidly increase in size and become painful in the past month with no previous history of trauma, fever, and weight loss. There was nothing to note in his medical history and his social history included chronic smoking only. The patient was referred to the orthopedic on-call team for review. He had a diffuse swelling measuring 40 × 40 cm over the medial aspect of the left thigh. The skin over the swelling was stretched and not discolored, there was no erythema, the swelling was tender, warm with ill-defined margins, not fluctuant, not pulsatile, and immobile. There was no palpable thrill and no bruit. There was no distal neurological deficit in his left leg. The dorsalis pedis and posterior tibial pulsations were palpable, and the left foot was well perfused and warm. An infective process such as an abscess was ruled out and a clinical diagnosis of a soft-tissue sarcoma was strongly considered as the underlying pathology. A plain radiograph showed a soft-tissue shadow in the medial aspect of the left thigh with no erosion or scalloping of the femur but some calcifications in the margins of the swelling (Fig. 1a and b). Then, an urgent magnetic resonance imaging (MRI) scan booked as an outpatient. While waiting for the MRI scan, he represented to the emergency department 2 weeks later with increased swelling size, bruising in the medial aspect of his left thigh, and overlying necrotic skin (Fig. 2). The dorsalis pedis and posterior tibial pulsations were now not palpable, but the left foot was well perfused and warm. His blood tests showed a red blood count of 106 g/L. His urea and electrolytes showed a mild acute kidney injury that was treated with intravenous fluids. He, then, had an urgent same-day MRI scan (Fig. 3a and b) for a presumed expanding highly vascular soft-tissue sarcoma but was reported to be a pseudoaneurysm of both left superficial femoral (SFA) (size 19.6 cm × 16.1 cm) and popliteal artery (size 9.4 cm × 4.9 cm), as well as an incidental right popliteal pseudoaneurysm (size 7.4 cm × 5.3 cm). He was urgently for surgery to the nearest vascular center as the left SFA artery was shown to be ruptured. This patient underwent an emergency left femoral-popliteal artery aneurysm exclusion bypass surgery, debridement, and drainage of the hematoma. He, then, had another operation for further wound debridement and a vacuum assisted dressing applied. He continues to have follow-up to monitor the vascular graft and up to his follow-up (15 months post-surgery); the vascular graft is patent and working well. The rehabilitation postoperatively for this patient included a multi-disciplinary team approach. Tissue viability nurses specializing in the treatment and management of wounds worked to monitor and care for the wound preventing further deterioration and to promote adequate healing. Physiotherapists also played an important role in helping him to regain strength and mobility in the affected leg through exercises that improve range of motion, muscle strength, and cardiovascular fitness. Follow-up with the plastics and vascular surgeons was also done to monitor the graft, ensuring proper healing, and to prevent complications. This patient is well, walking independently, and the thigh wound is healed. For the right popliteal pseudoaneurysm, he is currently on the waiting list for popliteal artery aneurysm repair.
The dorsalis pedis and posterior tibial pulsations were now not palpable, but the left foot was well perfused and warm. His blood tests showed a red blood count of 106 g/L. His urea and electrolytes showed a mild acute kidney injury that was treated with intravenous fluids. He, then, had an urgent same-day MRI scan (Fig. 3a and b) for a presumed expanding highly vascular soft-tissue sarcoma but was reported to be a pseudoaneurysm of both left superficial femoral (SFA) (size 19.6 cm × 16.1 cm) and popliteal artery (size 9.4 cm × 4.9 cm), as well as an incidental right popliteal pseudoaneurysm (size 7.4 cm × 5.3 cm). He was urgently for surgery to the nearest vascular center as the left SFA artery was shown to be ruptured. This patient underwent an emergency left femoral-popliteal artery aneurysm exclusion bypass surgery, debridement, and drainage of the hematoma. He, then, had another operation for further wound debridement and a vacuum assisted dressing applied. He continues to have follow-up to monitor the vascular graft and up to his follow-up (15 months post-surgery); the vascular graft is patent and working well. The rehabilitation postoperatively for this patient included a multi-disciplinary team approach. Tissue viability nurses specializing in the treatment and management of wounds worked to monitor and care for the wound preventing further deterioration and to promote adequate healing. Physiotherapists also played an important role in helping him to regain strength and mobility in the affected leg through exercises that improve range of motion, muscle strength, and cardiovascular fitness. Follow-up with the plastics and vascular surgeons was also done to monitor the graft, ensuring proper healing, and to prevent complications. This patient is well, walking independently, and the thigh wound is healed. For the right popliteal pseudoaneurysm, he is currently on the waiting list for popliteal artery aneurysm repair.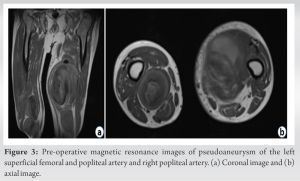
Pseudoaneurysms are rare and are difficult to diagnose on clinical examination. There have been some case reports regarding the clinical uncertainty or misdiagnosis of pseudoaneurysms mimicking soft-tissue sarcomas [3,4,5]. At the initial presentation, this patient presented with features of a soft-tissue sarcoma which included a large slowly growing mass deep to the superficial fascia. An infective process – such as abscess – was ruled out due to the chronicity of the thigh mass and the absence of local clinical features of infection (erythema) and normal body temperature. An MRI scan is a good imaging modality to differentiate between these two differentials – sarcoma and pseudoaneurysm – with a dynamic enhanced MR angiography being the most useful. However, MRI scans are expensive and can be difficult to arrange in an outpatient setting – like in this case – and another alternative can be an ultrasound Doppler that is cheaper and can be done at the bedside. There are only a very limited number of cases published in the literature with spontaneous SFA artery pseudoaneurysms and rupture is yet more rare [6]. There are case reports though of femoral artery pseudoaneurysm – but with the exception of the limited cases mentioned above – they clearly document a traumatic blunt trauma [7,8,9,10,11,12,13,14]. This case is unique not only due to the diagnostic uncertainty but also due to the concurrent bilateral non-traumatic pseudoaneurysms that have not been documented in the literature before. Bilateral pseudoaneurysms have also been documented, but in the neck and only following maxillofacial surgery [15].
Non-traumatic spontaneous pseudoaneurysm is a very rare cause of a thigh mass. This should be considered as a part of a differential diagnosis as it can mimic a soft-tissue sarcoma and be investigated promptly with an MRI scan or an ultrasound Doppler. On diagnosis of a pseudoaneurysm, the medical professional should be alerted of the possibility of bilateral and other anatomical sites of pseudoaneurysms.
Patients can present to a medical practitioner with a large thigh mass having the clinical features of a soft-tissue sarcoma. We advise that medical practitioners must consider the possibility of a non-traumatic pseudoaneurysm and conduct prompt further radiological investigations with subsequent referral to the regional vascular surgical center.
References
- 1.Rivera PA, Dattilo JB. Pseudoaneurysm. In: StatPearls; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/nbk542244 [Last accessed on 2022 Jul 31]. [Google Scholar | PubMed]
- 2.Ugurlucan M, Sendil S, Sayin OA, Barburoglu M, Gok E, Turkyilmaz G, et al. Spontaneous superficial femoral artery pseudoaneurysm in Behcet’s disease. Case Rep Med 2014;2014:860243. [Google Scholar | PubMed]
- 3.Albert S, Daniel S, Gouse M, Cherian VM. Case of pseudoaneurysm mimicking a soft tissue sarcoma: A diagnostic pitfall. Malays J Med Sci 2015;22:61-4. [Google Scholar | PubMed]
- 4.Byregowda S, Puri A, Gulia A, Prabhu A, Janu A. Pseudoaneurysms masquerading as malignant bone tumours. J Clin Diagn Res 2016;10:XD03-5. [Google Scholar | PubMed]
- 5.Keller PM, Simon MS. Post-traumatic false aneurysm simulating a soft tissue tumor. Orthopedics 1988;11:641-3. [Google Scholar | PubMed]
- 6.Darigny S, Astarci P, Elens M. A rare case of spontaneous superficial femoral artery pseudoaneurysm in a young patient: Case report and review of literature. J Surg Case Rep 2021;2021:rjab327. [Google Scholar | PubMed]
- 7.Lee SY, Lee SJ, Lee CS. Bilateral pseudoaneurysms of femoral artery caused by blunt trauma. J Trauma 2011;71:782. [Google Scholar | PubMed]
- 8.Naouli H, Jiber H, Bouarhroum A. False aneurysm of perforating branch of the deep femoral artery-report of two cases. Int J Surg Case Rep 2015;14:36-9. [Google Scholar | PubMed]
- 9.Currie P, Turnbull CM, Shaw TR. Pseudoaneurysm of the femoral artery after catheterization: Diagnosis and treatment by manual compression guided by Doppler color flow imaging. Br Heart J 1994;72:80-4. [Google Scholar | PubMed]
- 10.Chong KC, Yap EC, Lam KS, Low BY. Profunda femoris artery pseudoaneurysm presenting with triad of thigh swelling, bleeding and anaemia. Ann Acad Med Singap 2004;33:267-9. [Google Scholar | PubMed]
- 11.Hanna GB, Holdsworth RJ, McCollum PT. Profunda femoris artery pseudoaneurysm following orthopaedic procedures. Injury 1994;25:477-9. [Google Scholar | PubMed]
- 12.Khoshnevis J, Sobhiyeh MR, Zavareh MF. Deep femoral artery branch pseudoaneurysm after orthopedic procedure requiring surgical treatment: A case report. Trauma Mon 2012;17:305-8. [Google Scholar | PubMed]
- 13.Valli F, Teli MG, Innocenti M, Vercelli R, Prestamburgo D. Profunda femoris artery pseudoaneurysm following revision for femoral shaft fracture nonunion. World J. Orthop 2013;4:154-6. [Google Scholar | PubMed]
- 14.Ritchie ED, Haverkamp D, Schiphorst TJ, Bosscha K. False aneurysm of the profunda femoris artery, a rare complication of a proximal femoral fracture. Acta Orthop Belg 2007;73:530-2. [Google Scholar | PubMed]
- 15.Słotwińska A, Orzechowska-Wylęgała B, Latusek K, Katra M. Bilateral maxillary pseudoaneurysms as a complication of craniofacial fracture: A case report. Am J Case Rep 2021;22:e932443. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report
June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report June 1, 2026 Delayed Pseudoaneurysm of the Subclavian Artery Following Clavicle Fracture Fixation: A Case Report
June 1, 2026 Delayed Pseudoaneurysm of the Subclavian Artery Following Clavicle Fracture Fixation: A Case Report April 1, 2026 Pseudoaneurysm of the Medial Genicular Artery as a Rare Cause of Recurrent Knee Swelling – A Case Report
April 1, 2026 Pseudoaneurysm of the Medial Genicular Artery as a Rare Cause of Recurrent Knee Swelling – A Case Report November 1, 2025 Anterior Tibial Artery Pseudoaneurysm Following Arthroscopic Ankle Arthrodesis: A Case Report
November 1, 2025 Anterior Tibial Artery Pseudoaneurysm Following Arthroscopic Ankle Arthrodesis: A Case Report