
The inverted boot technique for intertrochanteric fracture is safe and easy way to maintain reduction and rotation in below-knee amputation. Fracture fixation by proximal femoral nail is better way for rehabilitation and early mobilization.
Dr. Sanket Tanpure, Department of Orthopaedics, Dr Vithalrao Vikhe Patil Medical College, Ahmednagar, Maharashtra, India. E-mail: sankettanpure55@gmail.com
Abstract
Introduction: An intertrochanteric fracture (IT) with below-knee (BK) amputation is challenging to manage since it is impossible to provide the ideal amount of traction to reduce the fracture due to the lack of a foot. We emphasize this complex problem and offer solutions to overcome it.
Case Presentation: A 55-year-old man with a previous ipsilateral BK amputation presented to us after an episode of fall. The patient had been using a BK prosthesis for mobilization before the fall. Radiographs revealed a femoral IT fracture. A proximal femoral nail (PFN) fixation was intended for the fracture, but positioning the patient on the fracture table for surgery proved challenging. The patient had to be carefully positioned on the fracture table during surgery.
Conclusion: The reverse boot technique is an effective method for treating an IT fracture in a patient with ipsilateral BK amputation. It involves the usual technique of applying traction, achieving reduction, and fixing the fracture with a PFN of the appropriate size. The patient was able to walk with support the next day after surgery and pre-injury mobility was regained within 3 days. We here emphasize a method of applying traction with this simple modification of the fracture table to apply an adequate amount of traction safely.
Keywords: Fracture table, intertrochanteric fracture, below-knee amputation.
Hip fracture incidence rises as the age of general population increases [1]. By achieving early union with rehabilitation and an acceptable reduction in fracture, the primary objectives of hip fracture therapy are to re-establish pre-operative gait and activity status and to reduce fracture-related complications [2,3]. Intertrochanteric fracture (IT) fractures are commonly treated with the help of a fracture table [3,4]. To maintain reduction in a stable fracture, axial traction, internal rotation, and adduction of the limb are done. Percutaneous pinning sometimes helps to maintain the anatomical reduction in an unstable fracture. When treating an IT femur fracture, the patient is positioned on a fracture table with their feet fastened to the boots. After that, necessary traction and rotation are applied for reduction purposes. It has always been a challenge for orthopedic surgeons all over the world to manage an IT fracture in a patient with a below-knee (BK) amputation as it requires the presence of a foot to strap the patient’s limb to the fracture table. Careful attention to patient positioning is of paramount importance in such cases. Positioning on the fracture table is challenging for these patients since they are missing their feet and part of their leg. We bring emphasis on the difficulties encountered when treating an IT fracture in a patient who had BK amputations.
The 55-year-old male patient experienced right hip-joint pain after an episode of a fall while walking on the road 5 days prior. There was no history of chronic illness. Despite having a history of BK amputation in the same leg following a right foot crush injury a few years ago, the patient walked independently and carried out activities of daily life with the use of a prosthetic limb.
Clinical findings
In the AO classification, the fracture type was A1.2 (Fig. 1). The patient was classed as stage I by anesthetic profile according to the American Society of Anesthesiology.
Therapeutic intervention
On the fracture table, surgery was intended to fix the fracture using a proximal femoral nail (PFN). To facilitate access to C-arm imaging fluoroscopy while under spinal anesthesia, the contralateral limb was fastened to the leg support device and placed in a 90° hip flexion and abduction posture. After flipping the boot piece upside-down, the wounded leg’s stump was fastened with elastic bandages and Velcro straps, and the knee was flexed (Fig. 2). In other words, by inverting the boot piece, the flexed knee was anchored at the boot piece, permitting traction, and manipulation like in a typical femoral IT fracture. Following adequate traction and internal rotation, fracture reduction was confirmed in anteroposterior (AP) and cross-table lateral imaging. The leg was addicted 10–15° to get better access for insertion of PFN. A 3 mm K-wire was used to transfix the fracture. A lateral X-ray confirmed K-wire position (Fig. 3). After taking an incision of 4 cm from the tip of greater trochanter, entry was taken under C-arm guidance by the awl. A bent tip guide wire was passed through the entry awl. Following the proximal reaming, a 135 PFN with a size of 12 × 180 mm was inserted. A femoral bolt guide pin and a de-rotation screw guide pin were inserted through the proximal hole within 5 mm in subchondral bone of the femoral head. The 8 mm cannulated femoral bolt coupled with a 6.4 mm cannulated de-rotation bolt was positioned in the usual manner in femoral neck and head and confirmed on the AP and cross-table lateral views under C-arm guide. Traction was gradually released while tightening the screw to achieve appropriate compression at the fracture site. The apposition of anterior cortex was confirmed in lateral view after final fixation of nail.
Follow-up and outcome
Postoperatively, plain radiographs showed well-reduced fracture with appropriate internal fixation (Fig. 4). During the 12-month post-operative follow-up period, there were no orthopedic complications, such as infection, implant blackout, or progression of the underlying diseases. The fracture was observed to be united at 6 months after surgery. The patient regained his pre-operative gait function and was able to walk with complete weight-bearing on the prosthetic leg.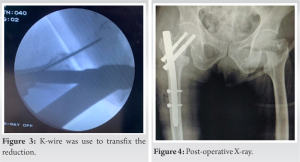
IT fractures are quite prevalent in the elderly population and can be managed with a variety of surgical techniques such as dynamic hip screw, IM nailing, and dynamic condylar screw. Patients with ipsilateral BK amputations and IT fractures face unique challenges in positioning and fracture reduction due to the lack of the foot and a portion of the leg. The literature is lacking in details on methods for solving this issue. A few techniques for reducing femoral IT fractures in individuals with limb amputations have been described in earlier research. Anjum and McNicholas [5] described a fractured neck of the femur in a BK amputated leg in 22-year-old patient. Skin traction is administered to the stump with an elastic bandage while the patient was lying on the fracture table. The traction cord was fastened to the traction assembly to maintain adequate traction and reduce the fracture. In the distal femur or proximal tibia, a Steinmann pin was placed, and later, the rope was tied to the pin and the boot piece was tractioned [7]. Although the Steinmann pin along with the rope technique can maintain appropriate traction and the adduction posture, achieving rotational stability with these was difficult. The fourth option was the placement of the distal femur external fixation which was secured to the fracture table [8]. Although it offers adequate traction along with stability, it is very cumbersome to adjustments during surgery, which leads to additional medical expenses. External fixators increase soft-tissue injury risk to stump, pin-track infection [9], and pullout fracture by applying traction to an osteoporotic bone. Freitas et al. [10] described a neck of the femur fracture in 28-year-old patient with above-knee (AK) leg amputation. The fracture was secured with three cancellous cannulated (CC) screws and reduced with a 4.5 mm Schantz pin. Ochi et al. [11] used Al-Harthy et al. method [4] of boot inversion for supporting the stump of the amputated limb in a flexed knee manner in a 97 years old BK amputee and fixed with intramedullary Gamma nail. Boussakri et al. [12] described an 81-year-old patient with a fractured neck of femur in an AK amputated leg and treated with bipolar hemiarthroplasty by Harding approach. Kandel et al. [13] described a 68-year-old patient with a femoral neck fracture with an AK amputation treated with bipolar hemiarthroplasty using the posterior approach. Our study preferred PFN over hemiarthroplasty or CC screw to fix the femoral IT fracture. Considering the patient’s age, infection following hemiarthroplasty is always a high-risk event after amputation. For a better outcome following surgery, post-operative rehabilitation is essential. Strengthening exercises for the hip and knee, early mobilization, respiratory exercises, and mental rehabilitation play a major role in recovery. He walked with full weight-bearing with a BK prosthesis at a 12-month follow-up without any support. This study had some drawbacks. First, there was the possibility of selection bias. Second, it is necessary to consider the small number of cases. Due to the enormous influence of hip fractures on a patient’s quality of life, adequate fracture reduction and surgical fixation procedure selection are critical. The fracture table used extensively to treat hip fractures has its limitations when applied to patients with lower limb amputation.
For orthopedic surgeons, fracture fixation in BK amputation is a complex and technically challenging issue. The conundrum is to reduce the fracture by providing traction and rotation. The technique mentioned here provides several options for handling this circumstance while resolving this issue.
IT fracture of the femur rarely happens in a BK amputation. Proper reduction and definitive fixation are the keys to get better outcomes after surgery. The inverted boot technique is a simple and safe method to provide adequate traction for proper reduction along with slight modifications with the fracture table.
References
- 1.Kim DS, Shon HC, Kim YM, Choi ES, Park KJ, Im SH. Postoperative mortality and the associated factors for senile hip fracture patients. J Korean Orthop Assoc 2008;43:488-94. [Google Scholar | PubMed]
- 2.Kaufer H, Matthews LS, Sonstegard D. Stable fixation of intertrochanteric fractures. J Bone Joint Surg Am 1974;56:899-907. [Google Scholar | PubMed]
- 3.Chun YS, Oh H, Cho YJ, Rhyu KH. Technique and early results of percutaneous reduction of sagittally unstable intertrochateric fractures. Clin Orthop Surg 2011;3:217-24. [Google Scholar | PubMed]
- 4.Al-Harthy A, Abed R, Campbell AC. Manipulation of hip fracture in the below-knee amputee. Injury 1997;28:570. [Google Scholar | PubMed]
- 5.Anjum SN, McNicholas MJ. Innovative method of traction on fracture table in femoral neck fracture fixation in a below knee amputee. INJ Extra 2006;37:277e-8. [Google Scholar | PubMed]
- 6.Davarinos N, Ellanti P, McCoy G. A simple technique for the positioning of a patient with an above knee amputation for an ipsilateral extracapsular hip fracture fixation. Case Rep Orthop 2013;2013:875656. [Google Scholar | PubMed]
- 7.Ramseier LE, Werner CM, Hug T, Preiss S. Supracondylar traction of a pertrochanteric femur fracture in a patient amputated below the knee. Unfallchirurg 2005;108:239-40. [Google Scholar | PubMed]
- 8.Gamulin A, Farshad M. Amputated lower limb fixation to the fracture table. Orthopedics 2015;38:679-82. [Google Scholar | PubMed]
- 9.Parameswaran AD, Roberts CS, Seligson D, Voor M. Pin tract infection with contemporary external fixation: How much of a problem? J Orthop Trauma 2003;17:503-7. [Google Scholar | PubMed]
- 10.Freitas A, Souto DR, da Silva JF, Dantas BR, de Paula AP. Treatment of an acute fracture of the femoral neck in a young female adult with a transfemoral amputation: A case report. JBJS Case Connect 2015;5:e58. [Google Scholar | PubMed]
- 11.Ochi H, Baba T, Hamanaka T, Ozaki Y, Watari T, Homma Y, et al. Safe and effective reduction technique for intertrochanteric fracture with ipsilateral below-knee amputated limb. Case Rep Orthop 2017;2017:2672905. [Google Scholar | PubMed]
- 12.Boussakri H, Alassaf I, Hamoudi S, Elibrahimi A, Ntarataz P, ELMrini A, et al. Hip arthroplasty in a patient with transfemoral amputation: A new tip. Case Rep Orthop 2015;2015:593747. [Google Scholar | PubMed]
- 13.Kandel L, Hernandez M, Safran O, Schwartz I, Liebergall M, Mattan Y. Bipolar hip hemiarthroplasty in a patientwith an above knee amputation: A case report. J Orthop Surg Res 2009;4:30. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Radiological Outcomes of Reamed Short Proximal Femoral Nailing in Intertrochanteric Fractures in Patients Aged 50 Years and Above
August 1, 2026 Radiological Outcomes of Reamed Short Proximal Femoral Nailing in Intertrochanteric Fractures in Patients Aged 50 Years and Above August 1, 2026 Evaluation of Orthopedic Outcomes of Proximal Femoral Nailing for Intertrochanteric Fractures and Predictive Value of Pre-operative Glycemic Status, Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio: A Prospective Study
August 1, 2026 Evaluation of Orthopedic Outcomes of Proximal Femoral Nailing for Intertrochanteric Fractures and Predictive Value of Pre-operative Glycemic Status, Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio: A Prospective Study July 1, 2026 Intertrochanteric Fracture Secondary to Solitary Osteochondroma: A Case Report and Literature Review
July 1, 2026 Intertrochanteric Fracture Secondary to Solitary Osteochondroma: A Case Report and Literature Review July 1, 2026 Association of Different Levels of Vitamin D Deficiency and Hip Fracture in Indian Population: A Cross-sectional Study
July 1, 2026 Association of Different Levels of Vitamin D Deficiency and Hip Fracture in Indian Population: A Cross-sectional Study