
Stress fractures of the medial femoral condyle are an infrequent phenomenon. An early and correct diagnosis is imperative for the management of such fractures and to prevent complications.
Dr. Vijay Kumar, Department of Orthopaedics, AIIMS, New Delhi, India. E-mail: vijayaiims@yahoo.co
Abstract
Introduction: Stress fractures are common in athletics and military recruits exposed to repetitive mechanical stresses. They are usually located in the weight-bearing lower limb and foot bone, usually in the metatarsals and tibial shaft. The medial femoral condyle is an unusual site for a stress fracture so reporting such a case is imperative.
Case Report: We report a case of a medial femoral condyle stress fracture in a young adult without any athletic or military background, which was managed conservatively by cast application.
Conclusion: Stress fractures of the medial femoral condyle are an infrequent phenomenon in individuals without any military or athletic background. Surgeons should have to be very vigilant when dealing with cases of indistinct knee pain.
Keywords: Stress fracture, medial femoral condyle, insufficiency fracture, sports injury
Stress fractures are overuse injuries usually occurring in military personnel and athletes [1,2,3]. Among the various theories known for the mechanism of stress fractures, the most accepted is the repetitive stress after microtrauma to the bone with insufficient rest for the healing process [4]. The incidence of a stress fracture in the medial femoral condyle is unknown due to its rarity. Diagnosis of stress fracture at such a site is difficult for clinicians due to similar presentation of other intra-articular pathologies and negative radiographs at the inception of the disease [5]. It is essential to diagnose such cases early to prevent the progression of stress fracture into a complete full-blown fracture. We are reporting a case of a medial femoral condyle stress fracture in a young adult.
An 18-year-old male presented to us with pain and instability around the right knee for one month. He did not recall any episode of a significant traumatic event. On examination, tenderness was present around the medial epicondyle and tests for knee ligaments were normal. Initial radiographs were within normal limits (Fig. 1). Blood parameters such as calcium, vitamin D3, and alkaline phosphatase level were within normal range. The patient was advised to rest and prescribed NSAIDs to relieve the symptoms. A week later, the patient revisited with similar complaints. This time he was advised to take an magnetic resonance imaging (MRI) of the knee, which revealed signal changes in T1 and T2 images in the medial femoral condyle with an incomplete oblique fracture line starting from the medial epicondyle and progressing toward the intercondylar area (Fig. 2). 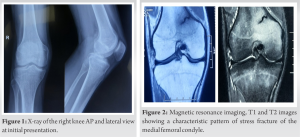 The patient was diagnosed with a stress fracture of the medial femoral condyle. The patient was managed with a long cylindrical plaster of paris cast for 4 weeks and advised for non-weight-bearing axillary crutches assisted walking. Oral calcium, vitamin C, and vitamin D supplements were prescribed for rapid recovery. The cast was removed after 4 weeks and radiographs at 4 weeks follow-up visit were normal (Fig. 3). The patient was symptomatically relieved from his initial symptoms with only slight post-cast knee stiffness. The patient was advised physical therapy in form of quadriceps, hamstring, and knee ROM exercises and non-weight-bearing for 2 more weeks. At 6 weeks follow-up, patients attained full knee range of movement without any pain. MRI was done which revealed complete healing of the stress fracture with no signal changes and fracture line (Fig. 4). The patient was advised to do partial weight-bearing and continue the physical therapy. At 3 months follow-up, the patient was allowed full weight-bearing without any support.
The patient was diagnosed with a stress fracture of the medial femoral condyle. The patient was managed with a long cylindrical plaster of paris cast for 4 weeks and advised for non-weight-bearing axillary crutches assisted walking. Oral calcium, vitamin C, and vitamin D supplements were prescribed for rapid recovery. The cast was removed after 4 weeks and radiographs at 4 weeks follow-up visit were normal (Fig. 3). The patient was symptomatically relieved from his initial symptoms with only slight post-cast knee stiffness. The patient was advised physical therapy in form of quadriceps, hamstring, and knee ROM exercises and non-weight-bearing for 2 more weeks. At 6 weeks follow-up, patients attained full knee range of movement without any pain. MRI was done which revealed complete healing of the stress fracture with no signal changes and fracture line (Fig. 4). The patient was advised to do partial weight-bearing and continue the physical therapy. At 3 months follow-up, the patient was allowed full weight-bearing without any support.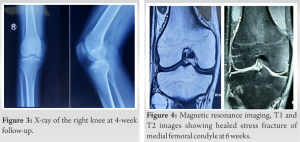
Stress fracture accounts for 20% of cases in a sports medicine clinic [6]. They are commonly encountered when a normal bone is undergoing repetitive stress or when a weakened bone undergoing physiological loading. The earlier scenario is commonin sports persons and military recruits, and the latter one in tumours, osteoporosis and osteomalacia [7]. The usual site for such fractures is the weight-bearing bones of the lower limbs and foot. Metatarsal, tarsal bones, and tibial shaft account for most of the cases. The femur accounts for 6-7% of cases of stress fracture usually occurring in the neck region. The incidence of a stress fracture in the distal femur region is unknown due to the unusual site of presentation [6]. Our case had no military and athletic background, and either had any abnormal bone metabolic studies which make our case a rare of rare entity, so reporting such an interesting case becomes an essentiality. Patients with stress fractures present with pain during the activity which gets relieved by taking rest. Diagnosis of stress fracture of the medial femoral condyle is difficult for surgeons due to its anatomic location near the knee joint, so confusing them with other intra-articular ligament-related pathologies. In our case, along with pain, instability was also a presenting complaint which too, which made us, think of other intra-articular pathologies first. In a study by Drabicki et al., distal femur stress fractures are rare and diagnosing them is an even more challenging task for surgeons due to their proximity to the knee joint [5]. Early diagnosis and management of such fractures are very essential to prevent the progression of fractures. Misdiagnosis can lead to catastrophic complications. In a study by Huber et al., a patient with a stress fracture of the distal femur, which was wrongly diagnosed as meniscus pathology, underwent an iatrogenic fracture of the distal femur during arthroscopy [8]. The initial imaging modality to start with for a suspected stress fracture is a plain radiograph, which has a sensitivity of only 10% in the first 3 weeks after the symptoms [6]. In our case too, the plain radiographs were normal and showed no signs of a stress fracture of the medial condyle of the femur. MRI is the diagnostic imaging of choice for stress fractures accounting for 100% sensitivity and high specificity. A stress fracture in MRI depicts a low signal intensity in the T1 image (dark line) with surrounding fewer dark areas, and in the T2 images line remains dark with increased signal surrounding the line showing bone marrow edema [9]. Our case also depicted a similar pattern in the MRI study, which confirmed our diagnosis. The treatment of stress fracture is usually conservative, which includes rest, cast immobilization, protected activity, and nutritional supplementation [10]. Full recovery is normally accomplished in 6 weeks with the resumption of full weight-bearing. In our case also, we obtained a full radiological recovery in 6 weeks (MRI after 6 weeks showed normal study) and started partial weight-bearing at a 6-week follow-up and total weight-bearing at 3 months.
Stress fractures of the medial femoral condyle are an infrequent phenomenon in individuals without any military or athletic background. Delayed and missed diagnoses are typical for such fracture patterns. Surgeons should have to be very vigilant when dealing with cases of indistinct knee pain and should include the possibility of such fractures at this rare site in their differential diagnosis.
Surgeons should have to be very vigilant when dealing with cases of indistinct knee pain and should include the possibility of stress fracture of the medial femoral condyle at this rare site in their differential diagnosis.
References
- 1.Finestone A, Milgrom C, Wolf O, Petrov K, Evans R, Moran D. Epidemiology of metatarsal stress fractures versus tibial and femoral stress fractures during elite training. Foot Ankle Int 2011;32:16-20. [Google Scholar | PubMed]
- 2.Fredericson M, Jennings F, Beaulieu C, Matheson GO. Stress fractures in athletes. Top Magn Reson Imaging 2006;17:309-25. [Google Scholar | PubMed]
- 3.Takkar P, Prabhakar R. Stress fractures in military recruits: A prospective study for evaluation of incidence, patterns of injury and invalidments out of service. Med J Armed Forces India 2019;75:330-4. [Google Scholar | PubMed]
- 4.Yasuda T, Miyazaki K, Tada K, Matsuda Y, Murakami H. Stress fracture of the right distal femur following bilateral fractures of the proximal fibulas. A case report. Am J Sports Med 1992;20:771-4. [Google Scholar | PubMed]
- 5.Drabicki RR, Greer WJ, DeMeo PJ. Stress fractures around the knee. Clin Sports Med 2006;25:105-15. [Google Scholar | PubMed]
- 6.Kavin M, Chrusch A. Grade 4 distal femur stress fracture in a long-distance hiker on the Appalachian trail. Wilderness Environ Med 2021;32:59-62. [Google Scholar | PubMed]
- 7.Vij N, Ranade AS, Gupte S, Oka GA, Belthur MV. Tension-sided femoral neck stress fracture in an adolescent with Vitamin D deficiency and osteomalacia: A case report. JBJS Case Connect 2021;11. [Google Scholar | PubMed]
- 8.Huber W, Trieb K. Serious consequences of the wrong diagnosis of meniscal lesion in a case of stress fracture of the distal femur. Arthroscopy 2002;18:935-8. [Google Scholar | PubMed]
- 9.Pistolesi GF, Caudana R, D’Attoma N, Residori E, Pregarz M. Case report 686. Stress fracture at distal end of femur simulating “periosteal desmoid”. Skeletal Radiol 1991;20:454-7. [Google Scholar | PubMed]
- 10.Matcuk GR Jr., Mahanty SR, Skalski MR, Patel DB, White EA, Gottsegen CJ. Stress fractures: Pathophysiology, clinical presentation, imaging features, and treatment options. Emerg Radiol 2016;23:365-75. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Profile of Sports Injuries: Retrospective Analysis from a Single Centre
July 1, 2026 Profile of Sports Injuries: Retrospective Analysis from a Single Centre June 1, 2026 Malleolar Stress Fracture as the First Manifestation of Undiagnosed Crohn’s Disease: A Case Report
June 1, 2026 Malleolar Stress Fracture as the First Manifestation of Undiagnosed Crohn’s Disease: A Case Report February 1, 2026 Atraumatic Subtrochanteric Stress Fracture in a 45-Year-Old Housewife: Diagnostic Challenge and Management Strategy
February 1, 2026 Atraumatic Subtrochanteric Stress Fracture in a 45-Year-Old Housewife: Diagnostic Challenge and Management Strategy December 1, 2025 Adult-Onset Fanconi Syndrome Presenting as Stress Fractures: A Case Report
December 1, 2025 Adult-Onset Fanconi Syndrome Presenting as Stress Fractures: A Case Report