
Medial meniscus posterior root reconstruction and open wedge high tibial osteotomy may be a useful treatment for medial meniscus posterior root tear with varus knee.
Dr. Takuya Ohno, Department of Orthopedic Surgery, Nippon Koukan Hospital, 1-2-1 Koukandori, Kawasaki-Ku, Kawasaki City, Kanagawa Prefecture, 210-0852, Japan. E-mail: shinenow44@yahoo.co.jp
Abstract
Introduction: Pull-out suture, suture anchor, and open- wedge high tibial osteotomy have been widely used for surgical treatment of medial meniscus posterior root tear, and relatively good clinical results have been reported. However, radiologic and arthroscopic findings are not sufficient. This report describes the first case, to the best of our knowledge, of medial meniscus posterior root reconstruction and high tibial osteotomy for medial meniscus posterior root tear with varus knee.
Case Report: A 78-year-old Japanese man was referred to our hospital due to the right popliteal pain. Plain radiography showed the mechanical axis percentage of the right limb to be 17%, indicating a varus mechanical axis. magnetic Magnetic resonance imaging noted a medial meniscus posterior root tear. Medial meniscus posterior root reconstruction and high tibial osteotomy were performed. His knee injury and osteoarthritis score improved from 22 points preoperatively to 91 points 1 year postoperatively. The graft had a good live induction and the medial meniscus hoop was maintained.
Conclusion: This report is the first case, to the best of our knowledge, of medial meniscus posterior root reconstruction and high tibial osteotomy for medial meniscus posterior root tear with varus knee. This type surgical technique may be useful for a meniscus posterior root tear with varus knee.
Keywords: Arthroscopy, high tibial osteotomy, knee, medial meniscus posterior root tear, meniscus reconstruction.
Medial meniscus posterior root tear (MMPRT) is defined as a radial tear of <10 mm from the MMPR attachment and is reported to disrupt the MM hoop action thereby disrupting knee joint kinematics [1,2]. MMPRT is widely known to cause osteonecrosis (ON) and rapid progression of knee osteoarthritis [3,4]. Therefore, it is important to properly treat and restore the hoop action. Pull-out suture, suture anchor, and open-wedge high tibial osteotomy (OWHTO) have been widely used for surgical treatment of MMPRT, and relatively good clinical results have been reported [5,6,7]. However, radiologic and arthroscopic findings are not sufficient [5,6,7]. Recently, Ishikawa et al. reported that MMPR-reconstruction is useful for reconstructing the failed hoop function of MM [8]. However, the results of MMPR-reconstruction have not been reported, and its usefulness is not yet known. This report describes a case of MMPRT with varus knee treated with MMPR-reconstruction and OWHTO.
A 78-year-old Japanese man was referred to this hospital due to the right popliteal pain. His height was 159 cm, his weight was 59 kg, and his body mass index was 23.3. He had no history of trauma. Orthopedic physical examination of the right knee revealed tenderness from the posteromedial joint line to the popliteal fossa with a mild joint effusion. Ligament instability tests were all negative. The McMurray test was positive for pain but not click. His range of motion (ROM) was restricted to 0–145 degrees because deep flexion exacerbated the pain. The knee injury and osteoarthritis score (KOOS) was 22 points. Imaging studies were performed with plain radiography, including the entire length of the lower limbs with weight-bearing, frontal and lateral views of both knees, and magnetic resonance imaging (MRI). Plain radiography showed no obvious osteoarthritis of the knee, but the mechanical axis percentage was 17%, indicating a varus knee (Fig. 1). MRI showed a giraffe neck sign on T2-weighted coronal imaging and a white meniscus sign on T2-weighted sagittal imaging (Fig. 2).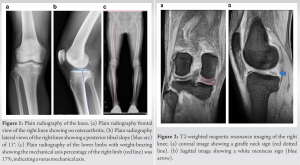 Arthroscopic MMPR-reconstruction using an autogracilis tendon and OWHTO was performed as follows: (1) The presence of MMPRT was confirmed using a probe (Fig. 3). (2) An autologous gracilis tendon was harvested using a diagonal skin incision on the medial side of the tibia. The harvested gracilis tendon was double folded and grafted with a baseball-groove suture at the end.
Arthroscopic MMPR-reconstruction using an autogracilis tendon and OWHTO was performed as follows: (1) The presence of MMPRT was confirmed using a probe (Fig. 3). (2) An autologous gracilis tendon was harvested using a diagonal skin incision on the medial side of the tibia. The harvested gracilis tendon was double folded and grafted with a baseball-groove suture at the end. (3) A soft-tissue tunnel was created from the femoral to the tibial side at the outer lesion of the MM, 5 mm from the MMPR edge, using a 3.5 mm 90° hook electrode (Mitek VAPR 3 system, DePuy Mitek), and a 60 °hooked rotary scissors (ACUFEX; Smith and Nephew) (Fig. 4). (4) A tibial tunnel was made from the lateral tibia to the anatomical MMPR attachment using an anterior cruciate reconstruction guide (3M) (Fig. 5).
(3) A soft-tissue tunnel was created from the femoral to the tibial side at the outer lesion of the MM, 5 mm from the MMPR edge, using a 3.5 mm 90° hook electrode (Mitek VAPR 3 system, DePuy Mitek), and a 60 °hooked rotary scissors (ACUFEX; Smith and Nephew) (Fig. 4). (4) A tibial tunnel was made from the lateral tibia to the anatomical MMPR attachment using an anterior cruciate reconstruction guide (3M) (Fig. 5). 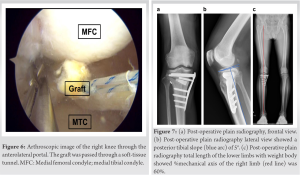 (5) The graft was inserted through a soft-tissue tunnel (Fig. 6). (6) OWHTO was performed using normal procedures to provide a mechanical axis percentage of 62.5% (Fig. 7). (7) The graft was pulled through the tibial tunnel and fixed with an artificial ligament fixture (pull-out button, AI-Medic) (Fig. 8a). The patient was started on partial weight-bearing 2 weeks postoperatively, and he was allowed full weight-bearing 6 weeks postoperatively. His ROM was limited to 90° for the first 4 weeks postoperatively and 130°for 6–12 weeks postoperatively. Full flexion and squatting were allowed beginning 3 months postoperatively. The patient underwent a second look operation and metal removal 1 year postoperatively. The reconstructed MMPR was well engrafted (Fig. 8b), and the area of necrosis showed good fibrocartilage augmentation (Fig. 9).
(5) The graft was inserted through a soft-tissue tunnel (Fig. 6). (6) OWHTO was performed using normal procedures to provide a mechanical axis percentage of 62.5% (Fig. 7). (7) The graft was pulled through the tibial tunnel and fixed with an artificial ligament fixture (pull-out button, AI-Medic) (Fig. 8a). The patient was started on partial weight-bearing 2 weeks postoperatively, and he was allowed full weight-bearing 6 weeks postoperatively. His ROM was limited to 90° for the first 4 weeks postoperatively and 130°for 6–12 weeks postoperatively. Full flexion and squatting were allowed beginning 3 months postoperatively. The patient underwent a second look operation and metal removal 1 year postoperatively. The reconstructed MMPR was well engrafted (Fig. 8b), and the area of necrosis showed good fibrocartilage augmentation (Fig. 9).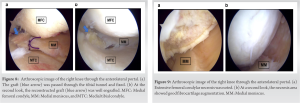 KOOS showed improvement with a score of 91 points, and the patient experienced no pain while performing normal activities.
KOOS showed improvement with a score of 91 points, and the patient experienced no pain while performing normal activities.
This report presents, to the best of our knowledge, the first case of MMPR-reconstruction and OWHTO for MMPRT with varus knee. A good clinical result was obtained. Furthermore, the MM hoop was successfully reconstructed and maintained 1 year later at a second look surgery. Pull-out suture, suture anchor, and OWHTO have been widely used for surgical treatment of MMPRT [5,6,7]. Moon et al. treated MMPRT with pull-out repair and reported that the Lysholm score improved from 48.3 points preoperatively to 83.2 points postoperatively, while MM extrusion increased from 3.6 mm preoperatively to 5.0 mm postoperatively [9]. Furthermore, Chung et al. reported worsening in Kellgren-Lawrence grade 5 years after pull-out repair [10]. Seo et al. reported 11 patients who had a second look surgery after pull-out repair and found none with complete healing. There were five cases of Lax healing, four cases of scar healing, and two cases of failed healing [11]. Jung et al. performed a follow-up MRI, on average 30 months after suture anchor repair, and reported that 50% had complete healing, 40% had partial healing, and 10% had no healing [7]. They also reported that MM extrusion ranged from 3.9 mm preoperatively to 3.5 mm postoperatively, with no significant improvement [7]. In this report, although there are only short-term results available, the patient achieved a good clinical outcome as well as good reconstruction of the hoop. Furthermore, despite extensive ON, good cartilage regeneration was observed. There have been reports of meniscus reconstruction using the peroneus longus tendon after lateral meniscectomy [12]. In addition, a study using rabbits reported that the semitendinosus and gracilis were suitable for meniscus reconstruction [13]. The outer region of the meniscus and the tendon are both rich in type I collagen [13,14], and it has been reported that the transplanted tendon can replace the meniscus [13]. As is well known in anterior cruciate ligament reconstruction, both the semitendinosus and gracilis show good bone tendon healing [15]. Furthermore, the varus knee mechanical axis and steep posterior tibial slope (PTS) increase mechanical stress on the MMPR and are reported to be risk factors. In the present case, OWHTO reduced the femorotibial angle and PTS, resulting in a reduced load on the graft. The use of OWHTO in conjunction with MMPR-reconstruction using the gracilis may have resulted in better engraftment.
This report is the first case, to the best of our knowledge, of MMPR-reconstruction and OWHTO for MMPRT with varus knee.
MMPR-reconstruction and OWHTO may be a useful treatment for MMPRT with varus knee.
References
- 1.Allaire R, Muriuki M, Gilbertson L, Harner CD. Biomechanical consequences of a tear of the posterior root of the medial meniscus. Similar to total meniscectomy. J Bone Joint Surg Am 2008;90:1922-31. [Google Scholar | PubMed]
- 2.LaPrade CM, James EW, Cram TR, Feagin JA, Engebretsen L, LaPrade RF. Meniscal root tears: A classification system based on tear morphology. Am J Sports Med 2015;43:363-9. [Google Scholar | PubMed]
- 3.Robertson DD, Armfield DR, Towers JD, Irrgang JJ, Maloney WJ, Harner CD. Meniscal root injury and spontaneous osteonecrosis of the knee: An observation. J Bone Joint Surg Br 2009;91:190-5. [Google Scholar | PubMed]
- 4.Guermazi A, Hayashi D, Jarraya M, Roemer FW, Zhang Y, Niu J, et al. Medial posterior meniscal root tears are associated with development or worsening of medial tibiofemoral cartilage damage: The multicenter osteoarthritis study. Radiology 2013;268:814-21. [Google Scholar | PubMed]
- 5.Kim CW, Lee CR, Gwak HC, Kim JH, Park DH, Kwon YU, et al. Clinical and radiologic outcomes of patients with lax healing after medial meniscal root repair: Comparison with subtotal meniscectomy. Arthroscopy 2019;35:3079-86. [Google Scholar | PubMed]
- 6.Nha KW, Lee YS, Hwang DH, Kwon JH, Chae DJ, Park YJ, et al. Second-look arthroscopic findings after open-wedge high tibia osteotomy focusing on the posterior root tears of the medial meniscus. Arthroscopy 2013;29:226-31. [Google Scholar | PubMed]
- 7.Jung YH, Choi NH, Oh JS, Victoroff BN. All-inside repair for a root tear of the medial meniscus using a suture anchor. Am J Sports Med 2012;40:1406-11. [Google Scholar | PubMed]
- 8.Ishikawa H, Okamura H, Ohno T, Fujita S, Akezuma H, Inagaki K. Arthroscopic medial meniscus posterior root reconstruction and pull-out repair combined technique for root tear of medial meniscus. Arthrosc Tech 2022;11:e109-14. [Google Scholar | PubMed]
- 9.Moon HK, Koh YG, Kim YC, Park YS, Jo SB, Kwon SK. Prognostic factors of arthroscopic pull-out repair for a posterior root tear of the medial meniscus. Am J Sports Med 2012;40:1138-43. [Google Scholar | PubMed]
- 10.Chung KS, Ha JK, Yeom CH, Ra HJ, Jang HS, Choi SH, et al. Comparison of clinical and radiologic results between partial meniscectomy and refixation of medial meniscus posterior root tears: A minimum 5-year follow-up. Arthroscopy 2015;31:1941-50. [Google Scholar | PubMed]
- 11.Seo HS, Lee SC, Jung KA. Second-look arthroscopic findings after repairs of posterior root tears of the medial meniscus. Am J Sports Med 2011;39:99-107. [Google Scholar | PubMed]
- 12.Milenin O, Strafun S, Sergienko R, Baranov K. Lateral meniscus replacement using peroneus longus tendon autograft. Arthrosc Tech 2020;9:e1163-9. [Google Scholar | PubMed]
- 13.Li C, Hu X, Meng Q, Zhang X, Zhu J, Dai L, et al. The potential of using semitendinosus tendon as autograft in rabbit meniscus reconstruction. Sci Rep 2017;7:7033. [Google Scholar | PubMed]
- 14.Kambic HE, McDevitt CA. Spatial organization of Types I and II collagen in the canine meniscus. J Orthop Res 2005;23:142-9. [Google Scholar | PubMed]
- 15.Lu H, Chen C, Xie S, Tang Y, Qu J. Tendon healing in bone tunnel after human anterior cruciate ligament reconstruction: A systematic review of histological results. J Knee Surg 2019;32:454-62. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain
August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain May 1, 2026 Simultaneous Anterior Cruciate Ligament Avulsion Fracture with Bilateral Posterior Meniscal Root Tears of the Knee: A Case Report
May 1, 2026 Simultaneous Anterior Cruciate Ligament Avulsion Fracture with Bilateral Posterior Meniscal Root Tears of the Knee: A Case Report April 1, 2026 Bucket Handle Tear of the Medial Meniscus with a New Magnetic Resonance Imaging Sign: The “Head in the Sand Sign” – A Case Report
April 1, 2026 Bucket Handle Tear of the Medial Meniscus with a New Magnetic Resonance Imaging Sign: The “Head in the Sand Sign” – A Case Report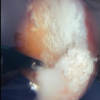 February 1, 2026 Gouty Arthritis Versus Chondrocalcinosis in a Stiff Knee, A Diagnostic Dilemma – A Case Report
February 1, 2026 Gouty Arthritis Versus Chondrocalcinosis in a Stiff Knee, A Diagnostic Dilemma – A Case Report