
Successful regeneration of the distal thumb tissues can be performed with a judicious combination of platelet-rich fibrin and dermal regeneration template. It achieves a near-normal appearance, sensation, and function of the thumb.
Dr. Srinjoy Saha, Department of Aesthetic and Plastic Surgery, Apollo Multispecialty Hospital, Kolkata, West Bengal, India. E-mail: ss@medi.ac
Abstract
Introduction: The human thumb is critical for performing complex movements with the hand. Injuries to the thumb can significantly impact an individual’s livelihood, and those with exposed bones or tendons have traditionally been treated with terminalization or reconstructive flap surgeries. However, many patients feel that their results could be better.
Case Report: We attempted a novel approach stacking multiple layers of a dermal regeneration template in a quest for better results. A young male teacher presented to our clinic with a 2-day-old severely injured thumb tip. Attempting to regenerate the lost fingertip, we first stacked the inner absorbable layers of the template layer-by-layer over the exposed bone and raw areas. Then, we injected platelet-rich fibrin (PRF) around the wound intraoperatively and at weekly intervals for a month to encourage soft-tissue development. After 6 months, we observed near-total soft-tissue development and good anatomical restoration of the lost thumb tip. Sensation returned to near-normal levels, with full functional recovery of the thumb and hand.
Conclusion: Our minimally invasive approach to reconstructing the distal thumb after an Allen Type 3 traumatic injury, utilizing PRF and a regenerative template, is a safe and effective alternative to traditional treatments. This innovative method has improved upon previously described results and may offer hope to many patients with severe thumb injuries.
Keywords: Thumb, dermal regeneration template, platelet-rich plasma, PRF. trauma, soft-tissue defect, hand, tissue reconstruction, tissue scaffold, biodegradable matrix, acellular.
The thumb is a unique organ in the human body that allows humans to perform superior tasks and more complex hand functions than other animals. Severe posttraumatic crush injuries of the thumb may be disastrous, compromising hand function for the rest of one’s life. To reconstruct distal thumb injuries with exposed bones and tendons, a viable soft-tissue cover is required [1]. Various flap surgeries have been described for reconstructing the thumb using tissues from the proximal areas of the thumb, adjacent fingers, palm, or abdomen/groin areas [2]. These procedures require well-equipped operating rooms, plastic surgery skills, anesthesia, and meticulous techniques. Still, in some patients, flaps may not produce satisfactory results [3]. A large portion of the world’s population lacks access to the sophisticated operating facilities required to perform complex reconstructive surgeries. As an alternative, healing by secondary intention through daily wash, ointment, and artificial semiocclusive barrier application has proven effective [4]. The use of dermal substitutes is another option, though the previous research has revealed some shortcomings with this approach [5]. We present a case in which we had to reconstruct an Allen Type 3 traumatic thumb injury using a minimally invasive procedure performed under local anesthesia, by stacking several layers of an acellular dermal regeneration template (ADRT) and injecting platelet-rich fibrin (PRF).
A 33-year-old male patient from a rural area arrived at our plastic surgery clinic with a 2-day-old thumb injury sustained in a motorcycle accident. He had recovered the soiled amputated distal part, but doctors at the local hospital refused to attach it for fear of infection. He had seen several doctors since the injury and had been advised about partial amputation and closure, as well as various flap surgeries. He insisted, however, on restoring the thumb’s appearance and function while avoiding any flap surgeries. On examination, he had complete loss of his right thumb’s distal soft tissues, with an exposed and injured distal phalanx, as well as loss of the entire tip and the nail plate (Fig. 1a and b).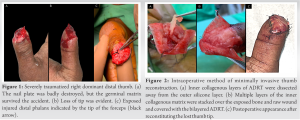 The distal phalanx was structurally intact despite being injured and exposed on the tip and palmar aspect (black arrow, Fig. 1c). With avulsed soft tissues, traumatized nail bed, and partial loss of the distal phalanx, the thumb injury was classified as Allen Type 3. The patient was advised on various treatment options, including terminalization, various types of flap cover, such as microvascular toe pulp and cross finger kite flaps, secondary intention healing with semiocclusive dressings, and the use of biomaterials. After much deliberation with his family, he decided on minimally invasive reconstruction with biomaterials. He believed it would provide him with an improved and safer version of healing through secondary intention. He was not confident in his ability to perform daily dressings and wound care while working alone in a remote area. As a result, a minimally invasive reconstruction was carried out using a wrist and digital block. Following wound debridement, PRF was prepared and injected according to the protocols described [6]. The inner porous collagenous layers of the bi-layered ADRT were dissected from the overlying silicone layer and stacked layer-by-layer over the exposed distal phalanx. The stacked collagenous layers mimicked the lost soft tissues of the distal thumb while covering the 2.5 × 1.5 cm raw wound (Fig. 2a). Finally, two artificial flaps were made from the remaining bi-layered ADRT and sutured over the stacked-up inner collagenous layers that covered the volar pulp and the injured nail bed (Fig. 2b). After laying down several layers of the inner collagenous matrix, the shape of the destroyed distal thumb was recreated (Fig. 2c). For the next 1 month, the patient was followed up at weekly intervals, during which time liquid PRF was injected into and around the progressing wound margins. Within 6 weeks, the outer silicone membrane covering the wound separated from the deeper layers on its own, revealing significant growth of soft tissues. The nail and volar tissues developed normally, but a 1 × 0.5 cm raw area remained over the tip (Fig. 3a-c).
The distal phalanx was structurally intact despite being injured and exposed on the tip and palmar aspect (black arrow, Fig. 1c). With avulsed soft tissues, traumatized nail bed, and partial loss of the distal phalanx, the thumb injury was classified as Allen Type 3. The patient was advised on various treatment options, including terminalization, various types of flap cover, such as microvascular toe pulp and cross finger kite flaps, secondary intention healing with semiocclusive dressings, and the use of biomaterials. After much deliberation with his family, he decided on minimally invasive reconstruction with biomaterials. He believed it would provide him with an improved and safer version of healing through secondary intention. He was not confident in his ability to perform daily dressings and wound care while working alone in a remote area. As a result, a minimally invasive reconstruction was carried out using a wrist and digital block. Following wound debridement, PRF was prepared and injected according to the protocols described [6]. The inner porous collagenous layers of the bi-layered ADRT were dissected from the overlying silicone layer and stacked layer-by-layer over the exposed distal phalanx. The stacked collagenous layers mimicked the lost soft tissues of the distal thumb while covering the 2.5 × 1.5 cm raw wound (Fig. 2a). Finally, two artificial flaps were made from the remaining bi-layered ADRT and sutured over the stacked-up inner collagenous layers that covered the volar pulp and the injured nail bed (Fig. 2b). After laying down several layers of the inner collagenous matrix, the shape of the destroyed distal thumb was recreated (Fig. 2c). For the next 1 month, the patient was followed up at weekly intervals, during which time liquid PRF was injected into and around the progressing wound margins. Within 6 weeks, the outer silicone membrane covering the wound separated from the deeper layers on its own, revealing significant growth of soft tissues. The nail and volar tissues developed normally, but a 1 × 0.5 cm raw area remained over the tip (Fig. 3a-c).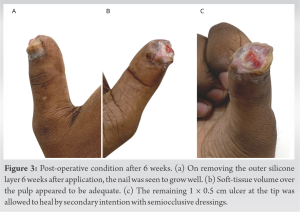 The patient was now advised to use semiocclusive dressings at weekly intervals by applying semi-permeable transparent polyurethane adhesive film to the wound. The remaining raw area was re-epithelialized within 2 weeks, though it healed with some scarring after healing by secondary intention (Fig. 4c). A follow-up examination after 6 months revealed a nearly complete development of the soft tissues. As the nail plate developed normally, the reconstructed thumb felt and appeared nearly similar to the opposite side (Fig. 4a and b). On the thumb tip and near the nail, a 1 × 0.3 cm strip of flat scar with mixed pigmentation was found at the area that healed by secondary intention (Fig. 4c). The 2-point discrimination over the reconstructed tip was 4 mm, which was slightly higher than the opposite normal side (3 mm). On the scarred strip, 2-point discrimination remained at 8 mm. The patient could feel adequate sensation along the progressively epithelializing wound edges throughout the follow-up period. He did not encounter numbness or hot/cold intolerance anytime. After healing completely, he was able to effortlessly perform all normal activities, including strenuous ones, with his newly reconstructed thumb. Patient-reported satisfaction was excellent, scoring a perfect 10/10 on a 1–10 visual analog scale, according to an outcomes questionnaire.
The patient was now advised to use semiocclusive dressings at weekly intervals by applying semi-permeable transparent polyurethane adhesive film to the wound. The remaining raw area was re-epithelialized within 2 weeks, though it healed with some scarring after healing by secondary intention (Fig. 4c). A follow-up examination after 6 months revealed a nearly complete development of the soft tissues. As the nail plate developed normally, the reconstructed thumb felt and appeared nearly similar to the opposite side (Fig. 4a and b). On the thumb tip and near the nail, a 1 × 0.3 cm strip of flat scar with mixed pigmentation was found at the area that healed by secondary intention (Fig. 4c). The 2-point discrimination over the reconstructed tip was 4 mm, which was slightly higher than the opposite normal side (3 mm). On the scarred strip, 2-point discrimination remained at 8 mm. The patient could feel adequate sensation along the progressively epithelializing wound edges throughout the follow-up period. He did not encounter numbness or hot/cold intolerance anytime. After healing completely, he was able to effortlessly perform all normal activities, including strenuous ones, with his newly reconstructed thumb. Patient-reported satisfaction was excellent, scoring a perfect 10/10 on a 1–10 visual analog scale, according to an outcomes questionnaire.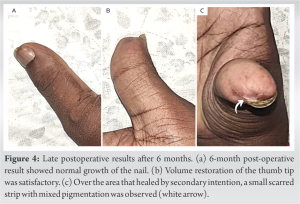
Several treatments are currently available for reconstructing distal finger injuries, which Allen classified from types 1 to 4 based on the severity of the injury. Fingertip injuries resulting in only soft-tissue loss without bone/tendon exposure (Allen types 1 and 2) can be successfully treated by secondary intention healing with or without the use of semiocclusive dressings. They are most effective when the wound is <1.5 cm long that is associated with a good recovery of sensation [4]. Split-thickness skin grafts may appear appealing for use on fingertip wounds where bone and tendon are not exposed, but they are not recommended. The skin grafts are not durable, cause numerous skin problems including fissures and ulcers, are prone to tenderness, cold sensitivity, and decreased protective and touch sensation. As a result of their dysfunctional outcomes, they are not considered appropriate for the fingertips, and certainly not over the thumb [4]. Terminalization (amputation) of the distal thumb with skeletal shortening provides a simpler solution for patients with bone/tendon exposure (typically Allen types 3 and 4). They result in permanent disability and loss of function, however, and is better avoided [2]. Replantation of the distal segment may be attempted first, if possible, especially in a sharp-cut injury. Alternatively, plastic surgeons may preserve the entire available skeletal length of the thumb and cover it with various types of flaps [1,2,3,4]. Local finger flaps and regional flaps from adjacent fingers/palm and distal flaps from the abdomen/groin are all options for flap coverage. Common options for thumb reconstruction include the palmar advancement flap, innervated cross-finger flap, first dorsal metacarpal artery island flap, and neurovascular island flap [1]. While flaps are an excellent treatment option for fingertip defects, they do have some drawbacks, such as the risk of flap loss, insufficient sensation, donor site morbidity, and excessive flap bulkiness that necessitates debulking procedures later [3]. Plastic surgeons used ADRT with and without skin grafts as an alternative to flaps for reconstructing fingertip defects. They were also used successfully to reconstruct soft-tissue deformities of the hand after severe posttraumatic hand wounds [7]. While a satisfactory range of motion and esthetically pleasing results was reported, complete restoration of form and function of the injured fingertips were not achieved, and volume loss over the finger pulp was observed [8]. Overall, secondary intention healing with ointment and semiocclusive dressings was found to be less expensive and likely to produce the same results. However, in this case, we imagined a regeneration matrix to be a more advanced form of secondary intention healing. Injecting PRF around the stacked inner layers of ADRT was expected to increase final tissue bulk and produce better results than those seen earlier with secondary intention healing or the standard application of a bi-layered ADRT [4,8]. Moiemen et al. observed four distinct histological stages of tissue development following the application of ADRT: (1) Imbibition, (2) fibroblast migration, (3) neovascularization, and (4) remodelling with maturation. Imbibition began within minutes of ADRT application on the wound bed. By day 7, fibroblast migration began at the base of the inner collagenous layers and gradually progressed upwards [9]. By the 3rd week, myofibroblasts settled into the inner porous layers and produced collagen. By the 2nd week, neovascularization began, and vascular lumen formed by the end of the 3rd week, becoming well established by the end of the 4th week. After the 4th week, the collagenous layers of ADRT were replaced with newly formed human collagen, and the regenerated dermis appeared histologically similar to a normal dermis [9]. Recent research found that injecting platelet-rich plasma (PRP) along the wound margins after applying a synthetic biodegradable temporizing matrix (BTM) over significant areas of exposed bones and tendons resulted in appreciable soft-tissue growth within BTM [10,11]. This game-changing concept was absorbed and applied in this case using PRF, a modified form of PRP. We anticipated that PRF would promote sufficient cell growth within all stacked inner layers of ADRT. PRP is defined by the American Red Cross as an autologous human plasma preparation with a high platelet concentration greater than or equal to 5.5 × 1010/50 mL, corresponding to a 2-7-fold increase in platelet concentration when compared to whole blood [12]. PRP contains a high concentration of various growth factors (TGF-1, PDGF, bFGF, VEGF, EGF, and IGF-1) and cytokine mediators [13]. This diverse set of growth factors and cytokines is essential for various stages of new tissue development such as cell proliferation, differentiation, chemotaxis, and angiogenesis. All of these processes were likely to have played a role in cell migration within the inner layers of ADRT in this case [13,14]. PRP was also shown to significantly improve skin wound healing by reducing local inflammation, increasing angiogenesis, and enhancing re-epithelialization [14]. PRF is the second generation of PRP, in which activated platelets are obtained from venous blood without the addition of anticoagulants. It is prepared using a different protocol and centrifugation technique [6,14]. Early clinical results showed that wound healing and dermatological interventions were effective [6]. In a regenerative study, PRF produced significantly higher fibroblast migration and collagen1 expression at least 7 days after injections [14,15]. Thus, weekly injection intervals appeared to be optimal for stimulating fibroblast migration and vascularization within the stacked collagenous layers of the ADRT used in this case study. Sufficient volume of newly developed tissues combined with wound contraction and re-epithelization to restore the shape and function of the distal thumb. However, it took several weeks to achieve satisfactory final results. Further research into shortening the treatment duration would broaden the benefits of this procedure.
An innovative method of stacking inner absorbable layers of a regenerative matrix and injecting PRF resulted in the safe and effective reconstruction of a severely injured thumb. While restoring the reconstructed thumb’s appearance and function, this minimally invasive procedure reduced the extent and pain of flap surgeries, anesthetic complications, donor site morbidity, and the need for any further procedures.
It can be difficult to restore a destroyed thumb after a major injury. Stacking several layers of a regenerative matrix simulates lost soft-tissue volume, and injecting PRF promotes cell growth and vascularization within them. Combining these two methods with a minimally invasive procedure yields excellent results.
References
- 1.Azari K. Thumb reconstruction. In: Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH, Cohen MS, editors. Green’s Operative Hand Surgery. 7th ed. Philadelphia: Elsevier; 2017. p. 1674-707. [Google Scholar | PubMed]
- 2.Pet MA, Ko JH, Vedder NB. Reconstruction of the traumatized thumb. Plast Reconstr Surg 2014;134:1235-45. [Google Scholar | PubMed]
- 3.Karjalainen T, Sebastin SJ, Chee KG, Peng YP, Chong AK. Flap related complications requiring secondary surgery in a series of 851 local flaps used for fingertip reconstruction. J Hand Surg Asian Pac Vol 2019;24:24-9. [Google Scholar | PubMed]
- 4.Kakar S. Digital amputations. In: Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH, Cohen MS, editors. Green’s Operative Hand Surgery. 7th ed. Philadelphia: Elsevier; 2017. p. 1708-52. [Google Scholar | PubMed]
- 5.Lorio MP, Ziakas G, Masker K, Howell S, Lewis BM. Use of artificial dermal substitute as a bridge in complex finger reconstruction. Wounds 2012;24:120-3. [Google Scholar | PubMed]
- 6.Shashank B, Bhushan M. Injectable platelet-rich fibrin (PRF): The newest biomaterial and its use in various dermatological conditions in our practice: A case series. J Cosmet Dermatol 2021;20:1421-6. [Google Scholar | PubMed]
- 7.Weigert R, Choughri H, Casoli V. Management of severe hand wounds with Integra® dermal regeneration template. J Hand Surg Eur Vol 2011;36:185-93. [Google Scholar | PubMed]
- 8.Elliot D, Adani R, Woo SH, Tang JB. Repair of soft tissue defects in finger, thumb and forearm: Less invasive methods with similar outcomes. J Hand Surg Eur Vol 2018;43:1019-29. [Google Scholar | PubMed]
- 9.Moiemen NS, Vlachou E, Staiano JJ, Thawy Y, Frame JD. Reconstructive surgery with Integra dermal regeneration template: Histologic study, clinical evaluation, and current practice. Plast Reconstr Surg 2006;117(7 Suppl):160S-74S. [Google Scholar | PubMed]
- 10.Saha S. Minimalistic reconstruction of exposed skull in a complex craniovertebral polytrauma. Surg Neurol Int 2021;12:248. [Google Scholar | PubMed]
- 11.Saha S. Tissue engineered successful reconstruction of a complex traumatized lower extremity. J Orthop Case Rep 2021;11:1-6. [Google Scholar | PubMed]
- 12.Ehrenfest DM, Rasmusson L, Albrektsson T. Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte-and platelet-rich fibrin (L-PRF). Trends Biotechnol 2009;27:158-67. [Google Scholar | PubMed]
- 13.Werner S, Grose R. Regulation of wound healing by growth factors and cytokines. Physiol Rev 2003;83:835-70. [Google Scholar | PubMed]
- 14.Xu P, Wu Y, Zhou L, Yang Z, Zhang X, Hu X, et al. Platelet-rich plasma accelerates skin wound healing by promoting re-epithelialization. Burns Trauma 2020;8:tkaa028. [Google Scholar | PubMed]
- 15.Fujioka-Kobayashi M, Miron RJ, Hernandez M, Kandalam U, Zhang Y, Choukroun J. Optimized platelet-rich fibrin with the low-speed concept: Growth factor release, biocompatibility, and cellular response. J Periodontol 2017;88:112-21. [Google Scholar | PubMed]

Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Thumb Distal Phalanx Enchondroma: Expanding the Surgical Corridor Through a Modified Volar Lateral Technique – A Case Report
August 1, 2026 Thumb Distal Phalanx Enchondroma: Expanding the Surgical Corridor Through a Modified Volar Lateral Technique – A Case Report August 1, 2026 Platelet-Rich Plasma Augmentation of Osteosynthesis in Femoral Neck Fractures: A Prospective Comparative Study Demonstrating Accelerated Union and Improved Function
August 1, 2026 Platelet-Rich Plasma Augmentation of Osteosynthesis in Femoral Neck Fractures: A Prospective Comparative Study Demonstrating Accelerated Union and Improved Function August 1, 2026 The Effect of Intraarticular Platelet-Rich Plasma Injection in Knee Osteoarthritis
August 1, 2026 The Effect of Intraarticular Platelet-Rich Plasma Injection in Knee Osteoarthritis August 1, 2026 Comparative Outcome Analysis of Leukocyte-Rich Platelet-rich Plasma, Leukocyte-Poor Platelet-rich Plasma, Injectable Platelet-rich Fibrin and Corticosteroid Injections in Periarthritis of the Shoulder: A Double-Blinded, Four-Arm Randomized Controlled Trial
August 1, 2026 Comparative Outcome Analysis of Leukocyte-Rich Platelet-rich Plasma, Leukocyte-Poor Platelet-rich Plasma, Injectable Platelet-rich Fibrin and Corticosteroid Injections in Periarthritis of the Shoulder: A Double-Blinded, Four-Arm Randomized Controlled Trial