
The Masquelet technique could be a novel treatment approach to manage septic arthritis of the pubic symphysis.
Dr. Takahiro Niikura, Department of Orthopaedic Surgery, Kobe University Graduate School of Medicine, 7-5-1 Kusunoki-Cho, Chuo-Ku, Kobe 650-0017, Japan. Email: tniikura@med.kobe-u.ac.jp
Abstract
Introduction: Osteomyelitis pubis is a rare disease that presents with fever, pubic or hip pain, pain during hip movement, and claudication to avoid pain. It most frequently affects young athletes involved in sports that require twisting and cutting, but its exact cause is unknown and no definite treatment has been established. We report a case of pubic osteomyelitis in a young football player who was treated using the Masquelet technique and antibiotics with a good clinical course.
Case Reports: A 22-year-old male football player in a national-level university club team visited a nearby clinic complaining of high fever and mild pain in his bilateral hip joints. As a result of examination, we diagnosed osteomyelitis pubis and reconstructed the pubic symphysis by the Masquelet technique. In this case, the joint-like structure of the pubic symphysis was successfully reconstructed, and the patient was able to continue playing the sport. Three years and 3 months after surgery, he had no limitation of bilateral hip joint range of motion and did not display any symptoms while playing football.
Conclusion: Masquelet technique could be a novel surgical method for managing osteomyelitis pubis, even in athletes.
Keywords: Pubic symphysis, infection, athlete, football.
Osteomyelitis pubis is a rare disease. It is controversial whether surgical or conservative treatment is the best management option for patients [1,2]. The most frequently employed surgical procedures are curettage of the affected lesion and drainage, and, to our knowledge, no report of bone reconstruction following curettage for pubic osteomyelitis exists [1,3,4]. The Masquelet technique is a two-stage surgery for critical bone defects, first reported by a French orthopedic surgeon [5]. It involves placing a cement spacer into the bone defect during the first surgery and its replacement with autologous bone in a second surgery. Reports indicate that it is being performed worldwide [6,7]. We report a case of a highly-skilled college-level soccer player from a university club team who returned to his pre-injury sports performance after treatment for pubic osteomyelitis using the Masquelet technique.
A 22-year-old male football player in a national-level university club team visited a nearby clinic complaining of high fever and mild pain in his bilateral hip joints. His body temperature was 38–40°C, his serum white blood cell count was 6700 cells/mm3 (3300–8500 cells/mm3), and his C-reactive protein level was 17.7 mg/dL (<0.3 mg/dL). He was treated with non-steroidal anti-inflammatory drugs (NSAIDs) to relieve his initial complaints. However, his symptoms persisted for 3 months, prompting X-ray, and computed tomography (CT) studies. Osteolytic changes in the bilateral pubis were noted (Fig. 1a and c). Therefore, osteomyelitis of the pubis was suspected, and he was referred to our institution for further treatment. He had a medical history of Ramsay Hunt syndrome and underwent steroid pulse therapy 3 months before the onset of fever and bilateral hip pain. On physical examination, we found no limitation in the range of motion or tenderness of both hip joints. However, radiating pain to the pubic symphysis was induced by hip adduction. Radiography of the pelvis performed at the previous hospital and at our hospital showed osteolytic changes chronologically progressing outward from the pubic symphysis (Fig. 1a and b). Magnetic resonance imaging (MRI) of the pelvis showed bone edema and fluid collection in the pubic symphysis (Fig. 1d). The culture of samples taken through CT-guided biopsy detected Staphylococcus epidermidis and Staphylococcus hominis. He was diagnosed with osteomyelitis pubis and septic arthritis of the pubic symphysis. Although clindamycin was administered for 6 weeks, it was not effective. In addition, he strongly hoped to return to playing soccer as soon as possible. Thus, the patient opted for surgical intervention and treatment using the Masquelet technique.
Magnetic resonance imaging (MRI) of the pelvis showed bone edema and fluid collection in the pubic symphysis (Fig. 1d). The culture of samples taken through CT-guided biopsy detected Staphylococcus epidermidis and Staphylococcus hominis. He was diagnosed with osteomyelitis pubis and septic arthritis of the pubic symphysis. Although clindamycin was administered for 6 weeks, it was not effective. In addition, he strongly hoped to return to playing soccer as soon as possible. Thus, the patient opted for surgical intervention and treatment using the Masquelet technique.
In the first surgery, debridement of infectious granulation tissue around the pubic symphysis was performed using the Pfannenstiel approach. The proximal, distal, and posterior cortices were preserved, and the cement spacer, including 10% vancomycin, was placed in the bone defect after debridement (Fig. 2). Clindamycin was orally administered for 6 weeks after surgery.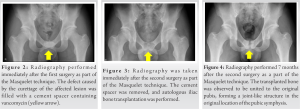
Two months after the first surgery, we confirmed no relapse of infection, removed the cement spacer, and transplanted an autologous iliac bone in a second surgery (Fig. 3). Union of the transplanted bone with original pubis was confirmed 7 months after the surgery. A joint-like structure was formed in the original location of the pubic symphysis (Fig. 4). Activities of daily living were not restricted immediately after the operation, and jogging was permitted 3 months postoperatively. Six months after the second operation, the patient returned to playing soccer. At the latest follow-up at 3 years and 3 months after the surgeries, remodeling in the bone transplantation area has proceeded, and a joint-like structure in the pubic symphysis appears closer to the original form (Fig. 5). There was no limitation of bilateral hip joint range of motion, and no symptoms were experienced while playing soccer.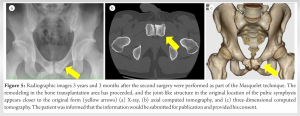
The patient was informed that the information would be submitted for publication and provided his consent.
Osteomyelitis pubis is rare, accounting for <1%–2 % of all hematogenous osteomyelitis cases [8]. It affects women with a medical history of gynecologic or urologic surgery, young athletes requiring forceful hip adduction, and patients with intravenous drug use [8]. Common symptoms include fever, pubic tenderness, pain with a hip motion, and claudication to avoid pain [8,9]. It has been reported that osteomyelitis pubis may occur due to the concurrence of hematogenous infection and osteitis pubis [3]. Osteitis pubis is correlated with sports, especially in activities that require movements such as kicking, pulling away, and running with abrupt changes in direction. This occurs most frequently in sports such as soccer, hockey, and rugby [10]. One of the factors involved in the manifestation of the symptoms is the biomechanical component in repeated kicking movements, which overloads the abdominal musculature, hip flexors, and hip adductors [11]. A similar tendency is observed in osteomyelitis pubis. In a systematic review on osteomyelitis pubis in athletes, Choi et al. reported its occurrence in ten male athletes, with a mean age of 28.1 years, consisting of five soccer players (which is a typical sport that requires kicking motion), two runners, one weight lifter, and one soldier [4].
The primary treatment of osteomyelitis pubis is initiated by rest and administration of antibiotics and NSAIDs. The duration of antibiotic therapy is 6 weeks on average [4]. However, it has been reported that more than 50% of the cases did not show clinical improvement after antibiotic treatment and required surgical debridement [8]. Whether surgical or conservative treatment should be selected for osteomyelitis pubis resistant to initial conservative treatment is controversial.
There have been reports of various surgical interventions, such as curettage, arthrodesis, wedge resection, and wide resection, for athletes with osteitis pubis. In all those reports, patients returned to competitive sports soon after treatment. This may support the use of surgical treatment among elite athletes [1,12,13]. However, to the best of our knowledge, there are no reports on the treatment of critical bone defects following surgery for osteomyelitis pubis.
French orthopedic surgeons first reported the Masquelet technique as a novel strategy for managing critical bone defects [5]. It is a two-stage surgery consisting of the temporary placement of a cement spacer into the bone defect, followed by autologous bone grafting into the defect. The induced membrane formed around the cement spacer between the two surgeries is vital, because it acts as a biological chamber protecting the autograft, providing blood supply, and inducing new bone formation from the bone graft [6].
Our patient was a male football player who underwent high-dose steroid therapy. We believe that frequent kicking movements and steroid-induced infection may have triggered the onset of osteomyelitis pubis.
Conservative treatment was ineffective in alleviating his symptoms, and the patient hoped to return to playing football as soon as possible. Based on the MRI findings, we deduced that the size of the bone defect after resection of the infected area would be large, and bone reconstruction would be needed to facilitate early return to competitive sports. Therefore, we decided to use the Masquelet technique. The transplanted bone graft was united to the original pubis, creating a joint-like structure. Bone union was confirmed 6 months after the final surgery. The patient could return to his sport soon after, and no recurrence was observed 3 years after the surgery.
Our findings support the hypothesis that severe spontaneous bacterial arthritis of the pubic symphysis in athletes requires surgical treatment. This is the first report describing the effectiveness of the Masquelet technique in such cases. This surgical method could be a novel method for managing septic arthritis of the pubic symphysis, even in athletes.
We encountered the case of a football player with septic arthritis of the pubic symphysis, who successfully returned to the pre-injury sports activity level after treatment using the Masquelet technique. The Masquelet technique could effectively treat osteomyelitis pubis, even in highly-skilled college-level athletes.
It is necessary to consider osteomyelitis pubis when athletes complain their hip pain, pubic pain, and fever. Surgical intervention could be required when osteomyelitis pubis is resistant to conservative treatment, and it is supposed that the Masquelet technique can be one of the surgical treatment options.
References
- 1.Mehin R, Meek R, Obrien P, Blachut P. Surgery for osteitis pubis. Can J Surg 2006;49:170-6. [Google Scholar | PubMed]
- 2.Smits FJ, Frima H, Schaeffeler C, Sommer C. Spontaneous septic arthritis of pubic symphysis in an elite athlete. Case Rep Surg 2016;2016:6384707. [Google Scholar | PubMed]
- 3.Pauli S, Willemsen P, Declerck K, Chappel R, Vanderveken M. Osteomyelitis pubis versus osteitis pubis: A case presentation and review of the literature. Br J Sports Med 2002;36:71-3. [Google Scholar | PubMed]
- 4.Choi H, Mccartney M, Best TM. Treatment of osteitis pubis and osteomyelitis of the pubic symphysis in athletes: A systematic review. Br J Sports Med 2011;45:57-64. [Google Scholar | PubMed]
- 5.Masquelet AC, Fitoussi F, Begue T, Muller GP. Reconstruction of the long bones by the induced membrane and spongy autograft. Ann Chir Plast Esthet 2000;45:346-53. [Google Scholar | PubMed]
- 6.Careri S, Vitiello R, Oliva MS, Ziranu A, Maccauro G, Perisano C. Masquelet technique and osteomyelitis: Innovations and literature review. Eur Rev Med Pharmacol Sci 2019;23:210-6. [Google Scholar | PubMed]
- 7.Kasha S, Rathore SS, Kumar H. Antibiotic cement spacer and induced membrane bone grafting in open fractures with bone loss: A case series. Indian J Orthop 2019;53:237-45. [Google Scholar | PubMed]
- 8.Ross JJ, Hu LT. Septic arthritis of the pubic symphysis: Review of 100 cases. Medicine (Baltimore) 2003;82:340-5. [Google Scholar | PubMed]
- 9.El Mezouar I, Abourazzak FZ, Mansouri S, Harzy T. Septic arthritis of the pubic symphysis: A case report. Pan Afr Med J 2014;18:149. [Google Scholar | PubMed]
- 10.Batt ME, Mcshanej M, Dillingham MF. Osteitis pubis in collegiate football players. Med Sci Sports Exerc 1995;27:629-33. [Google Scholar | PubMed]
- 11.De Queiroz RD, De Carvalho RT, De Queiroz Szeles PR, Janovsky C, Cohen M. Return to sport after surgical treatment for pubalgia among professional soccer players. Rev Bras Ortop 2014;49:233-9. [Google Scholar | PubMed]
- 12.Mulhall KJ, Mckenna J, Walsh A, Mccormack D. Osteitis pubis in professional soccer players: A report of outcome with symphyseal curettage in cases refractory to conservative management. Clin J Sport Med 2002;12:179-81. [Google Scholar | PubMed]
- 13.Williams PR, Thomas DP, Downes EM. Osteitis pubis and instability of the pubic symphysis. When nonoperative measures fail. Am J Sports Med 2000;28:350-5. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Profile of Sports Injuries: Retrospective Analysis from a Single Centre
July 1, 2026 Profile of Sports Injuries: Retrospective Analysis from a Single Centre May 1, 2026 Salvage of Infected Dynamic Hip Screw and Distal Femur Nail Fixation for Ipsilateral Femoral Neck and Femoral Shaft Fracture Using Antibiotic-Coated Custom Long-Stem Austin Moore Prosthesis – A Rare Case Report
May 1, 2026 Salvage of Infected Dynamic Hip Screw and Distal Femur Nail Fixation for Ipsilateral Femoral Neck and Femoral Shaft Fracture Using Antibiotic-Coated Custom Long-Stem Austin Moore Prosthesis – A Rare Case Report March 1, 2026 Case Report: Chronic Olecranon Bursitis as a Risk Factor for Squamous Cell Carcinoma
March 1, 2026 Case Report: Chronic Olecranon Bursitis as a Risk Factor for Squamous Cell Carcinoma March 1, 2026 Proximal Rectus Femoris Avulsion Repair in a Collegiate Football Player: A Case Report
March 1, 2026 Proximal Rectus Femoris Avulsion Repair in a Collegiate Football Player: A Case Report