
Early reduction, decompression and stabilization of Cervical Spine Injuries can help in neural recoveries.
Dr. Nitish Kumar, Department of Orthopedics, All India Institute of Medical Sciences, Gorakhpur, Uttar Pradesh, India. E-mail: nitishaiims@gmail.com
Abstract
Introduction: Subaxial cervical spine (C3-7) injuries are among the most common and potentially most devastating injuries involving the axial skeleton. The treatment of fracture dislocations of the cervical spine still varies. Early operative treatment has gained increasing acceptance. This case report will discuss a case of subaxial cervical spine fracture dislocation and spondyloptosis with minimal neurological compromise and after reduction and stabilization, complete recovery of neurological functional was achieved.
Case Report: A 26-year-old male patient presented to emergency department with history of road traffic accident with injury to his neck having complain of severe neck and shoulder pain and weakness in the right upper limb. On clinical and radiological evaluation, it was diagnosed a case of high-grade anterolisthesis C5 over C6 (spondyloptosis) with neurological compromise. Surgical intervention was done within 48 h with complete neurological recovery.
Conclusion: Satisfactory clinical and good long-term outcome can be obtained in fracture dislocation of subaxial cervical spine by anterior approach, discectomy, and anterior cervical plating.
Keywords: Subaxial spine, spondyloptosis, discectomy, cervical plating.
Injuries of the subaxial cervical spine (C3-7) are among the most common and potentially most devastating injuries involving the axial skeleton. The cervical spine often is injured in motor vehicle accidents and falls, resulting in bony or soft-tissue injury; however, the presence of multiple traumatic injuries may distract the examiner from the cervical spine. In the evaluation of the polytrauma patient, examination of the cervical spine is of utmost priority and must take precedence, along with maintenance of airway. The treatment of fracture dislocations of the cervical spine still varies. Several reports on various treatment protocols have been published, but surprisingly few [1,2] have compared their benefits and drawbacks. The treatment protocol for acute cord injury has no clear consensus regarding timing of decompression, but few studies including animal studies do support early decompression for better outcome in patients with bifacetal dislocation and incomplete cord injury with detoriating nural function [2,3,4]. I do not agree with the statement that there is controversy in management of acute traumatic fracture dislocation of spine in terms of operative management. The references quoted are for unilateral facetal dislocation and not for fracture dislocation. In recent years, the early operative treatment has gained increasing acceptance [5]. We report a case of subaxial cervical spine fracture dislocation and spondyloptosis with minimal neurological compromise and after reduction and stabilization, complete recovery of neurological function (please correct the spellings).
A 26-year-old ambulatory male patient presented to the emergency department with alleged history of road traffic accident with injury to his neck. He complained of severe neck and right shoulder pain along with weakness in the right upper limb. He had two episodes of vomiting after injury. The patient had a history of difficulty in micturition and had to put pressure for voiding; however, complete urinary retention was not there. The patient was catheterized with 14 Fr Foley’s Catheter to relieve of his symptoms. In addition, the patient did not pass stool since the injury (what do you mean by altered Bowel bladder habit). On primary survey, he was conscious and oriented to place, time, and persons. His vital parameters such as respiratory rate, pulse rate, blood pressure, and oxygen saturation were within normal limits. There was no tenderness over chest, abdomen, pelvis, and long bones on complete systemic examination of the patient done with adequate exposure. On local examination of the neck (with head stabilized as per standard ATLS protocol), there was a midline bony tenderness with painful and restricted neck motion. As cervical (write full forms) spine injury was suspected, a Philadelphia collar was applied around the neck. He had weak hand grip in the right side with motor weakness in the shoulder abduction and forward flexion (Power as per Medical Research Council (write full forms) grading-2/5), with ipsilateral triceps (C7) and biceps (C5) weakness (each 3/5) (it would be better if you mention the power examination based on myotomes). The skin sensation was decreased in C5 to T1 dermatomes in the same side. On neurological examination in the lower limb, the power in hip flexor, knee extensor, ankle dorsi-flexor, and plantar-flexor was 5/5 on both side with intact sensation in each dermatome below T2 including perianal sensation. Planter response was equivocal. The other deep tendon reflexes and superficial reflexes of both lower limbs were normal. The patient was able to feel the sensation of catheter on gentle pull on indwelling Foley’s catheter (Catheter Tug Test) (Please write complete neurological exam with reflexes and if there were any other injuries seen on examination).
Investigations
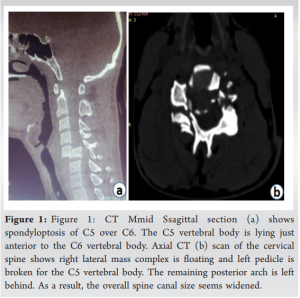
Non-contrast CT cervical spine was done (Fig. 1a and b). There were multiple comminuted fractures of anterior and posterior elements of C5 vertebra causing Grade V anterolisthesis of C5 over C6 (Spondyloptosis). The spinal canal at the injury level seemed to be widened due to injured and posteriorly displaced posterior elements.
A fracture of the left lamina of the C4 and right lamina of the C6 extending into foramen transversarium was also seen.
CT chest: B/L ribs fracture with minimal pneumothorax, minimal left-sided hemothorax, and B/L lung contusions.
CT brain: There was no evidence of any intracranial bleeding in the CT scan.
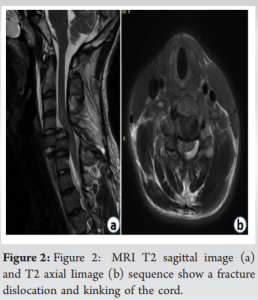
MRI spine: Post-traumatic spondyloptosis of C5 over C6 with kinking of the cervical spine cord was seen (Fig. 2a and b).
Procedure
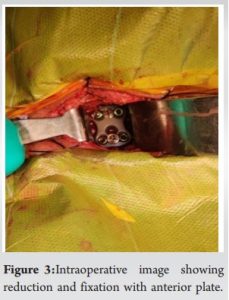
Preoperatively, traction of 6.5 kg was applied using a Gardner-Wells tongs and slight reduction of the listhesis was noted. Complete reduction was not achieved even under general anesthesia (no abbreviations please at least in first when you introduce the terms). Transverse incision from medial border of the right sternocleidomastoid to midline was given. After reaching to the injured area, the traumatized and ruptured disc at C5-C6 was removed using Kerrison rongeur. The injured PLL was also removed and complete decompression of the cord was achieved. Dislocation was reduced using caspar pins in each body with some manipulation. During manipulation and reduction, iatrogenic dural injury occurred which was sutured by 5–0 Prolene (what suture size and make??) under microscope and fibrin glue applied. Interbody fusion was done using a PEEK cage with autologous cancellous bone graft and single level anterior cervical plate (Medtronic). Name of implant company??
Post-operative course
No new neurological deficit was noted after surgery. The case was followed up on regular interval and the final follow-up was until 13 months after the surgery.

Neurological assessment at the final follow-up
His right-hand grip improved and became comparable to his normal side. The weakness around his right shoulder and elbow improved and there was no apparent deficit. Deep tendon reflexes were normal in both upper and lower limbs with improvement in his sensory functions. His bowel and bladder functions became regular with time. At the operated area, an intervertebral fusion was noted at the final follow-up with intact implant assembly.
Almost two-thirds of cervical spine injuries occur within the subaxial cervical spine, with dislocations occurring most commonly at C5–C6 and C6–C7 levels. Cervical facet dislocation usually occurs as a result of combined flexion and distraction forces [6]. Injury in this zone ranges from ligamentous insufficiency to unstable fracture, involving both posterior and anterior structures in the spinal column. This segment of the spine is highly vulnerable to injury as it is greatly mobile and at the proximal end it carries the weight of the head (12–15 pounds). Moreover, it has to bear great amount of force in acceleration and deceleration injuries [7]. Fracture dislocation of the cervical spine is a devastating injury and there is high probability of neurological deficit. The patient might have simple root injuries, as was in our case (C5, C6, and C7 root injuries), to a devastating complete neurological dysfunction (quadriplegia) [8]. In upper cervical spine, vertebral canal size is greater and hence neurological deficit less commonly happens. Whenever there is neural injury at that level, the patient is usually not compatible with independent life as there would be paralysis of phrenic nerves and subsequent respiratory apnea ensues [9]. In contrast, in subaxial cervical spine, the size of the canal decreases and any dislocation has a great potential to cause severe cord injury with quadriplegia. In our case, despite being spondyloptotic displacement at the C5 and C6 level, there were only root injuries in the right side. The spinal cord injury was not there, and hence, rest of the limbs were unaffected with preservation of patient’s ambulatory status. It was theorized that on account of the floating lateral mass in the one side and pedicle fracture in the other side, the posterior elements were separated from the vertebral body in anterior side and hence even after great displacement of the proximal vertebral body, the size of vertebral canal was paradoxically increased. The increased canal saved the patient from a major spinal cord injury. Like any other dislocation, this injury also has to be treated with reduction (closed or open) and stabilization. There is no consensus as to conservatively manage or one should do operative stabilization of the injury. However, scientific community is favoring operative early stabilization and rehabilitation of the patients as there are complications of chronic bed recumbencies. In our case, we could do the surgery within 48 h of the injury and reduction was easy. Complete reduction, cord decompression, and rigid stabilization with the early start of the rehabilitation greatly helped the patient to achieve full neurological recovery without complications. This type of injury demands diligent patient management with focus on preservation of neurological function as reduction and operative process itself is fraught with complications.
Subaxial cervical spine (C3-7) injuries are among the most common and devastating axial skeleton injuries associated with polytrauma patients. These patients presents to the emergency department with varying degree of neurological compromise. Management varies from conservative to surgical intervention in the form of reduction and stabilization. Early surgical intervention results in near complete neurological recovery.
Early surgical intervention and stabilization is the key for neurological recovery in patients of traumatic spondyloptosis of cervical spine with neurological compromise.
References
- 1.Beyer CA, Cabanela ME, Berquist TH. Unilateral facet dislocations and fracture-dislocations of the cervical spine. J Bone Joint Surg Br 1991;73B:977-81. [Google Scholar | PubMed]
- 2.Lee AS, MacLean JC, Newton DA. Rapid traction for reduction of cervical spine dislocations. J Bone Joint Surg Br 1994;76B:352-6. [Google Scholar | PubMed]
- 3.Beyer CA, Cabanela ME. Unilateral facet dislocations and fracture-dislocations of the cervical spine: A review. Orthopedics 1992;15:311-5. [Google Scholar | PubMed]
- 4.Fehlings MG, Sekhon LH, Tator C. The role and timing of decompression in acute spinal cord injury: What do we know? What should we do? Spine (Phila Pa 1976) 2001;26 24 Suppl:S101-10. [Google Scholar | PubMed]
- 5.Allred CD, Sledge JB. Irreducible dislocations of the cervical spine with a prolapsed disc: Preliminary results from a treatment technique. Spine (Phila Pa 1976) 2001;26:1927-30; discussion 1931. [Google Scholar | PubMed]
- 6.Zaveri G, Das G. Management of sub-axial cervical spine injuries. Indian J Orthop 2017;51:633-52. [Google Scholar | PubMed]
- 7.Shafafy R, Valsamis EM, Luck J, Dimock R, Rampersad S, Kieffer W, et al. Predictors of mortality in the elderly patient with a fracture of the odontoid process. Bone Joint J 2019;101-B:253-9. [Google Scholar | PubMed]
- 8.Rief M, Zoidl P, Zajic P, Heschl S, Orlob S, Silbernagel G, et al. Atlanto-occipital dislocation in a patient presenting with out-of-hospital cardiac arrest: A case report and literature review. J Med Case Rep 2019;13:44. [Google Scholar | PubMed]
- 9.Clark CR, White AA 3rd. Fractures of the dens. A multicenter study. J Bone Joint Surg Am 1985;67:1340-8. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Adolescent Cauda Equina Secondary to Traumatic Lumbar Disc Herniation: A Rare Case Report with Review of Literature
August 1, 2026 Adolescent Cauda Equina Secondary to Traumatic Lumbar Disc Herniation: A Rare Case Report with Review of Literature April 1, 2025 Acute Traumatic Lumbar Spondyloptosis with Complete Neurological Deficit: A Case Report and Literature Review
April 1, 2025 Acute Traumatic Lumbar Spondyloptosis with Complete Neurological Deficit: A Case Report and Literature Review January 1, 2025 Transformative Spinal Surgery: Lateral Position Unilateral Biportal Endoscopic Discectomy
January 1, 2025 Transformative Spinal Surgery: Lateral Position Unilateral Biportal Endoscopic Discectomy May 1, 2026 Tubercular Compound Palmar Ganglion Presenting with Chronic Wrist Swelling and Flexor Dysfunction: A Case Report
May 1, 2026 Tubercular Compound Palmar Ganglion Presenting with Chronic Wrist Swelling and Flexor Dysfunction: A Case Report