
To demonstrate that, external fixators, often familiar to use for infection or reconstruction of large long bones, can also be used as a treatment for small long bones such as metacarpals.
Dr. Oguzhan Korkmaz, Department of Orthopedics and Traumatology, Istanbul Medipol University, Istanbul, Turkey. E-mail: droguzhankorkmaz@gmail.co
Abstract
Introduction: Metacarpal bone fractures often lead to significant shortening in the phalanges; it can be caused by variable conditions, ranging from idiopathic, and infective to traumatic causes. There are very rare reports of metacarpals shortening in idiopathic primary hypoparathyroidism cases in the literature. Traumatic metacarpal shortening differs from congenital agenesis [2]. This condition leads to both functional and cosmetic limitations which affect the patient’s quality of life.
Case Report: A 22-year-old male patient was admitted to our outpatient clinic with a traumatic left-hand fracture that caused a bone defect in the second metacarpal shaft leading to bone loss, shortening and flexion limitation in the second finger of the left hand, and a flexion contracture in the first metacarpophalangeal joint. For the treatment plan, an external fixator was set on the second metacarpal of the left hand for a 23 mm elongation over a period of 58 days, elongation rate was organized as 1 mm/day. After achieving the planned elongation, another operation was planned for the reconstruction of the bone defect that has occurred due to trauma in the second metacarpal bone. An osteotomy was performed for extracting an iliac crest graft and inserting it into the bone defect after debridement of scar tissue. For the first metacarpophalangeal joint, an arthrodesis was performed through the use of plate and screws. Multiple studies have showed a common complication of pin tract infections, which were controlled with oral antibiotics and local wound care [10,11]. Proper alignment and union were achieved with early, stable fracture fixation of low-velocity gunshot wounds of the metacarpal. With early rehabilitation, treatment was provided without an increase in morbidity. [11].
Conclusion: It is possible to obtain acceptable surgical results when the method of fixation of the defect with autograft is used after lengthening with external fixator in pseudoarthrosis with metacarpal defect.
Keywords: Metacarpal fracture, metacarpal defect, metacarpal shortening, metacarpal lengthening/elongation.
Metacarpal fractures are common. It can be caused by variable conditions, ranging from idiopathic and infective to traumatic causes. There are very rare reports of metacarpals shortening in idiopathic primary hypoparathyroidism cases in the literature [1]. Traumatic metacarpal shortening differs from congenital agenesis [2]. Metacarpal bone fractures account for up to 50% of all hand fractures, and the fractures of metacarpal shaft are usually the result of direct or indirect trauma [3,4]. Metacarpal fractures with segmental bone loss occur with open injuries and are usually associated with significant soft-tissue injuries or defects [5]. Different methods and approaches have been used to fix the metacarpal bone defect and lengthening of the remaining bone segment. In a prospective cohort study that evaluated eight patients after delayed treatment of metacarpal bone defects, two different approaches were used for treating these fractures [5]. In classical approach, the length of the metacarpal is preserved with intermetacarpal Kirschner wires or with external fixator, and either a primary or delayed primary soft-tissue closure is performed [6]. Bone grafting of the metacarpal defect is then done at a later stage, preferably after the soft tissues have healed and hand joint mobility has been regained. However, it is different for others, since some consider that the first 10 days after injury is the golden period of wound healing which is the preferable time for bone grafting of a segmental bone defect [7]. The first step is to immediately debride the wound and stabilize the fracture. Then, any appropriate bone grafting or distraction can be performed with wound care. In our case, we have found the judicial use of both of these approaches, but the treatment modality was quite distinguishable compared to other cases of metacarpal bone defects, since bone loss had occurred and caused significant metacarpal shortening, which added a more challenging approach to properly preserve suitable bone length and stabilization. In this case report, we will be presenting our treatment approach and the functional findings after the treatment.
A 22-year-old male patient was admitted to our clinic with a main complaint of the left-hand fracture due to a war injury, the injury had resulted in metacarpal bone fracture in the left hand, which was operated for debridement 1.5 year ago back in his country (Fig. 1 and 2).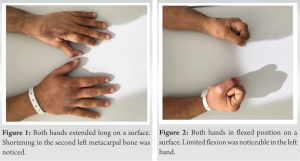 On physical examination, approximately 4 cm shortening was detected in the left second metacarpal bone, the range of motion was normal in the third, fourth, and fifth digits, and the flexion in the second metacarpophalangeal, proximal, and distal interphalangeal joints was in normal range, but the extension was found weak. There was also a 50° flexion contracture in the interphalangeal joint of the first finger, and the flexion in the metacarpophalangeal joint was restricted to 30–40°. The capillary filling time was appropriate and no loss of sensation has been observed. The patient had no known allergies, bad habits, or medications. The following tests were required for further evaluation of the patient: A left hand X-rays, infection parameters were examined as well. 2.13 cm bone defect and 2.2 cm shortening were detected in the left second metacarpal bone compared to the right hand on the X-rays (Fig. 3).
On physical examination, approximately 4 cm shortening was detected in the left second metacarpal bone, the range of motion was normal in the third, fourth, and fifth digits, and the flexion in the second metacarpophalangeal, proximal, and distal interphalangeal joints was in normal range, but the extension was found weak. There was also a 50° flexion contracture in the interphalangeal joint of the first finger, and the flexion in the metacarpophalangeal joint was restricted to 30–40°. The capillary filling time was appropriate and no loss of sensation has been observed. The patient had no known allergies, bad habits, or medications. The following tests were required for further evaluation of the patient: A left hand X-rays, infection parameters were examined as well. 2.13 cm bone defect and 2.2 cm shortening were detected in the left second metacarpal bone compared to the right hand on the X-rays (Fig. 3). 
For the treatment plan, lengthening was planned through the use of an external fixator to elongate the shortening in the second digit of the left hand (Fig. 4 and 5) for a planned 23 mm elongation that began over a period of 23 days (1 mm/day). The patient was followed up with the required imaging methods. Twenty-six days after the application of the external fixator, during a control visit, the operation’s details were discussed as follows: Perform an arthrodesis on the first metacarpophalangeal joint; iliac crest bone graft will be inserted into the bone defect fill in the empty gap in the second metacarpal bone. Lengthening was being controlled every week, the external fixator was adjusted to a 1 mm/day rate. The main aim was to reach an appropriate length of the second metacarpal. After reach the appropriate length, defect size was 4 cm. Metacarpophalangeal and proximal and distal interphalangeal joint mobilization was performed during the distraction to prevent any contracture. After the lengthening was done, second and the last surgery was performed. The patient was put under general anesthesia in a supine position, and essential sterilized covering and stain were applied. The osteotomy site was exposed through a 3 cm longitudinal incision on the anterior side of the left iliac crest bone, connective tissues were separated to reach the iliac crest and a 4 cm long tricortical bone autograft was resected, after that spongious autograft bone was collected from the iliac crest, the osteotomy site was then washed thoroughly with lots of saline fluid. An upper extremity tourniquet was applied on the left arm with a pressure of 220 mmhg. The fracture was exposed dorsally by first using Schanz screws to remove the external fixator device which was located on the second metacarpal bone of the left hand, then a longitudinal incision of 7 cm was made (the incision was conducted on top of an old incision in the same site) the extensor tendon was retracted laterally, connective tissues and neurovascular structures were cautiously explored. The defected bone was reached and the proximal and distal segments of the second metacarpal bone were visualized, and we have managed detecting a pseudoarthrosis tissue. Following this, the segments of the second metacarpal bone were cleaned through the help of rongeur. The taken iliac crest autograft was inserted into the bone defect which was between proximal and distal second metacarpal segments. An eight holes metacarpal plate was inserted for fixation, and once the iliac graft was supported and fixed with the spongious graft taken from the same site, we used seven screws to fixate the entire graft in the correct location. Intraoperative fluoroscopy imaging method was used to check the proper fixation of the screws and if they were aligned in place. For the first metacarpophalangeal joint that was contracted after trauma, arthrodesis was performed with a plate and screw in the appropriate position. Then, we closed the incision’s layers in a correct anatomic manner, after doing a sterile-dry wound dressing, a short arm cast was properly fitted into the patient’s arm. No perioperative complications were observed. Control X-rays were taken for the first 2 weeks after the surgery, weekly, and then once every 2 weeks. Complete union was observed at approximately 6 weeks (Fig. 6 and 7).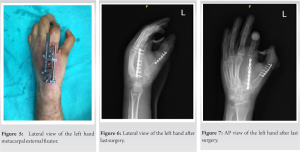
Metacarpal bone fractures account for up to 50% of all hand fractures [8] and variable causes may lead to bone defects and shortening in the metacarpal, while some causes such as trauma may lead to limitations in function in a shortened metacarpal. Metacarpal fractures with segmental bone defect can be successfully treated by iliac crest bone grafting like we do in our case [5]. The principle of treating a metacarpal fracture with a bone defect is to restore normal bone length, function, and total hand’s range of motion [1]. In another study that has evaluated eight patients with nine metacarpal bone defects due to high-velocity gunshot injuries, after a long time these patients were admitted to the hospital for appropriate intervention, but by then the metacarpals were severely affected by shortening with non-union fracture. The technique of choice was to first the application of an external fixator to the shortened and non-union metacarpal that was distracted at a rate of 1 mm/day until the original length of the metacarpal was restored [5]. The distraction osteogenesis method is successful and reliable for the lengthening of short metacarpals [6]. However, to avoid certain complications related to distraction method, some author’s suggest protection of the periosteum, by refraining from distraction rates of more than 2 × 0.25 mm/day and, if possible, avoid lengthening a bone by more than 40% [6]. To preserve the joint’s mobility, physical therapy was performed to maintain and/or regain the proximal interphalangeal and distal interphalangeal joint mobility. Metacarpophalangeal and proximal and distal interphalangeal joint mobilization was performed during the distraction, to preserve the joint’s mobility, and prevent contracture [5]. The technique that was used in this study was quite similar to our technique, which was taking a tri-cortical bone graft from the iliac crest and inserting it into the bone defect after debridement of scar tissue, but graft fixation was done using Kirschner wires in two cases, with screws in one case and by compressing graft between two ends of the defect with the external fixator in five [5]. Our graft fixation was mainly done using screws and plates, and the mean time to bone graft union was 6–8 weeks. However, there are also plenty of cases of congenital metacarpal or/and metatarsal shortening, patients with congenital short metacarpals and metatarsals underwent a lengthening procedure using the callus distraction method [6]. In a retrospective study [9] that analyzed metacarpal fractures due to gunshot wounds in 49 patients, the reconstructive procedures were carried out between 1 and 7 days after injury. Stable internal fixation was used to provide sufficient fracture stability to allow immediate phalangeal motion was obtained in all cases. Fixation was achieved with some form of intramedullary implant in 47 metacarpals. Moreover, the metacarpals that had no significant bone comminution were treated with solid metallic intramedullary spacers, multiple flexible intramedullary nails, or plates and screws. Metallic intramedullary spacers which were about 2–3 mm diameter rods were placed in the medullary canal of the metacarpal. After comminution, these implants were augmented with supplemental fixation that consisted of plates with intramedullary fixation, Kirschner wires, or cerclage wires to enhance control of rotation and length of the metacarpals. Autogenous iliac bone graft was used in 40 cases. With moderate comminution, only cancellous bone was added (28 cases), while fractures with circumferential bone loss received blocks of cortical-cancellous bone [9]. Whereas in our case, an autogenous iliac tri-cortical bone graft, 4 cm in length was excised through osteotomy with an approximately 5 cm incision. In another study [10], retrospectively evaluated the clinical outcome of distraction lengthening of the thumb metacarpal without bone grafting in seven patients with traumatic thumb loss which required amputation in all case. The surgical technique that was used for reconstruction was a paired threaded external fixation pins (2.5 mm) that were drilled perpendicular to the longitudinal axis in a dorsal to palmar direction through both cortices of the proximal and distal ends, then an osteotomy was performed using an oscillating saw, and a unilateral distractor which was mounted on the pins. The osteotomy is immediately distracted by 0.5 cm to ensure proper movement of the bone fragments and then closed again to bring the bone ends back into contact. Seven days post-operative as pain and edema have subsided, gradual lengthening has begun, and the patient was instructed to distract the device by 3–4 turns (1 mm) per day. After adequate lengthening, the patient remained in the external fixator until radiographs showed consolidation of thumb metacarpal. The distractor was left in place for a median of 155 days after the osteotomy while new bone formed and consolidated. In all seven patients, a stable pinch grip was obtained [10]. In our approach, we use external fixator for just achieve an appropriate length of the metacarpal bone. When it reached the appropriate length, the external fixator was removed and second stage surgery was performed. Lam et al. [11] retrospectively assessed the outcomes of distraction osteogenesis in skeletally mature adults with brachymetacarpia (which is a rare congenital hand deformity resulting in abnormal shortening of the metacarpal) also assessed the patients’ perspectives on their satisfaction through outcome measure scores. Seven metacarpal lengthening’s were performed in four adult females, the average amount engthened was 1.5 cm, the mean distraction rate was 0.432 mm/day, and the mean distraction time was 38 days. As a result, no functional loss was observed and has concluded that progressive distraction osteogenesis can obtain functionally successful results and improvement in esthetics and body image without severe complications in skeletally mature adults with brachymetacarpia [11]. We also did not see any significant functional loss in the patient in our surgical approach. In another study [12], multiple case studies have presented four cases of metacarpal bone reconstruction after gunshot wounds in a limited-resource setting. Reconstruction was performed using Masquelet’s technique without polymethylmethacrylate (PMMA) cement in a limited-resources setting in two patients. PMMA cement was usually required for the first stage of the surgery of gunshot reconstruction of bone defects, but since it was unavailable in that situation, the induced membrane technique was applied as it is a simple and effective procedure for reconstruction of segmental bone defects. The technique that was used Peimer et al. [1], was different in every case, for example, if the second or third metacarpal shaft was lost, wires were drilled transversely through the head of the injured metacarpal into the adjacent intact metacarpal. Moreover, distraction-fixation after partial loss of one metacarpal was achieved by transfixing the third metacarpal to the second, or the fourth to the fifth. With loss of portions of several finger metacarpals or of the first metacarpal, when intermetacarpal wires alone were insufficient to maintain length, the transverse wires were held by external fixation devices which were adjusted to achieve proper bone length. With loss of all four metacarpals, two sets of external fixation devices were required to prevent flattening of the transverse palmar arch. Whereas for patients who lost the metacarpal shaft and head, the distal transverse wires were placed in the proximal phalanges. If the patient was seen late, when bone and soft-tissue shortening had already occurred, the external fixation device was adjusted to gradually increase distraction and restore metacarpal length before bone grafting [1]. The late interpretation of that study shown was found quite similar to our approach, since our patient was admitted to our hospital 1.5 years after the injury which was caused by an explosion back in his country. The bone destruction caused by a direct hit of the bullet onto the diaphyseal region of the bone can cause severe comminution and bone loss. Bone grafting as part of the definitive fixation may be required. Depending on the degree of bone loss cancellous or en bloc corticocancellous bone may be used [13]. A study has reported good results with immediate corticocancellous autografting of bone in open hand fractures with bone loss [14]. However, trying to eliminate the total shortness in our patient in a single session was not appropriate due to possible soft-tissue problems and possible damage to neurovascular structures. Another retrospective study reviewed ten low-velocity gunshot fractures to the metacarpal which marked diaphyseal comminution. The fractured metacarpal was in the index finger in two patients, the middle finger in three patients, the ring finger in one patient, and the small finger in four patients. Three of the patients had an additional metacarpal fracture without bone loss at the time of presentation that was treated with a non-locking intramedullary rod in two patients (small finger) and a plate in one patient (thumb) [13]. The gunshot wound was debrided initially and dressed under sterile conditions. If there was no sign of infection within 7 days of the injury, the reconstruction was performed. If the wound appeared infected or the viability of the soft-tissue envelope was in question, then an external fixator or K-wires were used temporarily to maintain metacarpal length until the wound could be stabilized. After that the definitive procedure of locked intramedullary metacarpal rodding was performed within 7 days in all ten patients. With the help of the drill bits were available in the same diameter sizes as the intramedullary rods which are going to be used, beginning at 2.8 mm and ranged up to 4.8 mm, increased by every 0.4 mm. Metacarpal length was restored by longitudinal traction and a measurement was made of the proper nail length from the metaphyseal – diaphyseal area near the metacarpal head to the metaphyseal – diaphyseal area near the metacarpal base. The rod was introduced into the distal fragment and advanced distally. The fracture was then distracted and the rod was introduced into the proximal medullary canal. Each bone defect was grafted with bone harvested from the iliac crest. In eight of ten patients, corticocancellous bone was used, in one patient cancellous bone was used, and in one patient no graft was used. Active motion exercises were begun within 1 week of surgery with supervised occupational therapy [13]. We also applied physical therapy to our patient during his external fixation period and continued physical therapy after fixation. Intramedullary implants may always be an option in metacarpal fractures, but the surgeon’s experience is also important here. In our case, we preferred the osteosynthesis method with plate screw. In all cases that we have explored throughout the literature, the principal goals of primary treatment were to 1-prevent infection, 2-restore bone stability, length, and alignment, 3-prevent joint contractures, and 4-provide proper skin coverage. Regardless of the different techniques that were used in the literature on metacarpal fractures due to variable causes, the joint’s range of motion, neurovascular exploration, and post-operative rehabilitation were given crucial importance in the treatment process. However, distinguishable complications were noticed; three patients had pintract infections, which were controlled with oral antibiotics and local wound care [9]. In Murison et al., the patient had suffered an infection and the injured fingers were found shortened with rotational deformities. Repeat debridement resulted in an extensive diaphyseal bone defect on the 4th and 5th metacarpal bones [12]. In Peimer et al., series case study, there were two infections. One patient referred with a metacarpal osteomyelitis and the other patient who had primary closure with a distant flap developed a deep proteus infection 8 weeks after the bone graft [1]. Complications included one case each of pin infection, pin loosening and migration, and fracture of the lengthened bone. The pin infection was treated conservatively and the pin loosening/migration was treated by re-application of the distractor [10]. We did not encounter any pre-operative or post-operative complications.
The external fixator was applied for approximately 1 month (28 days). Postoperatively, the average follow-up of the patient was 6 months and the mean time to bone graft union (clinical and radiological) was 6–8 week. The mean grip strength of the injured hand was 80% compared to the intact side. A stable pinch grip was obtained. Normal metacarpal length was successfully achieved with a mean percentage of 30% increase in metacarpophalangeal joint motion after the operation. The proximal and distal interphalangeal joints had normal flexion motion postoperatively but limited extension. Grip strength and metacarpophalangeal joint movements were within acceptable ranges.
It is possible to obtain acceptable surgical results when the method of fixation of the defect with autograft is used after lengthening with external fixator in pseudoarthrosis with metacarpal defect.
It should be kept in mind that external fixators may be a treatment option for incomplete pseudoarthrosis of small long bones such as metacarpals.
References
- 1.Peimer CA, Smith RJ, Leffert RD. Distraction-fixation in the primary treatment of metacarpal bone loss. J Hand Surg 1981;6:111-24. [Google Scholar | PubMed]
- 2.Eisenschenk A, Spitzmüller R, Güthoff C, Obladen A, Kim S, Henning E, et al. Single versus dual Kirschner wires for closed reduction and intramedullary nailing of displaced fractures of the fifth metacarpal neck (1-2 KiWi): A randomized controlled trial. Bone Joint J 2019;101:1263- 71. [Google Scholar | PubMed]
- 3.Ashkenaze DM, Ruby LK. Metacarpal fractures and dislocations. Orthop Clin North Am 1992;23:19-33. [Google Scholar | PubMed]
- 4.Chung KC, Spilson SV. The frequency and epidemiology of hand and forearm fractures in the United States. J Hand Surg 2001;26:908-15. [Google Scholar | PubMed]
- 5.Akmaz I, Kiral A, Pehlivan O, Mahirogullari M, Solakoglu C, Rodop O, et al. Late reconstruction of neglected metacarpal shaft defects due to gunshot wound. J Hand Surg 2004;29:585-9. [Google Scholar | PubMed]
- 6.Erdem M, Sen C, Eralp L, Kocaoğlu M, Ozden V. Lengthening of short bones by distraction osteogenesis-results and complications. Int Orthop 2009;33:807-13. [Google Scholar | PubMed]
- 7.Freeland AE. External fixation for skeletal stabilization of severe open fractures of the hand. Clin Orthop 1987;214:93-100. [Google Scholar | PubMed]
- 8.Valizadeh N, Mehdizadeh A, Nazarbaghi S. Short fourth and fifth metacarpals in a case of idiopathic primary hypoparathyroidism. Indian J Endocrinol Metab 2013;17:924. [Google Scholar | PubMed]
- 9.Gonzalez MH, McKay W, Hall RF. Low-velocity gunshot wounds of the metacarpal: Treatment by early stable fixation and bone grafting. J Hand Surg 1993;18:267-70. [Google Scholar | PubMed]
- 10.Heitmann C, Levin LS. Distraction lengthening of thumb metacarpal. J Hand Surg 2004;29:71-5. [Google Scholar | PubMed]
- 11.Lam A, Fragomen AT, Rozbruch SR. Metacarpal lengthening in adults with brachymetacarpia. Hand (N Y) 2019;14:339-45. [Google Scholar | PubMed]
- 12.Murison JC, Pfister G, Amar S, Rigal S, Mathieu L. Metacarpal bone reconstruction by a cementless induced membrane technique. Hand Surg Rehabil 2019;38:83-6. [Google Scholar | PubMed]
- 13.Bach HG, Gonzalez MH, Hall RF. Locked intramedullary nailing of metacarpal fractures secondary to gunshot wounds. J Hand Surg 2006;31:1083-7. [Google Scholar | PubMed]
- 14.Stahl S, Lerner A, Kaufman T. Immediate autografting of bone in open fractures with bone loss of the hand: A preliminary report. Scand J Plast Reconstr Surg Hand Surg 1999;33:117-22. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Clinical outcome of Intramedullary Screw Fixation in Metacarpal and Phalangeal Fractures
March 1, 2026 Clinical outcome of Intramedullary Screw Fixation in Metacarpal and Phalangeal Fractures November 1, 2025 Outcome of Non-thumb Metacarpal Shaft Fractures Treated by Two Different Techniques – K Wire and Herbert Screw Fixation: A Comparative Single Centre Study
November 1, 2025 Outcome of Non-thumb Metacarpal Shaft Fractures Treated by Two Different Techniques – K Wire and Herbert Screw Fixation: A Comparative Single Centre Study April 1, 2025 Clinical Outcomes of Retrograde Percutaneous Pinning for Shaft Fracture of Metacarpal Bone: A Case Series
April 1, 2025 Clinical Outcomes of Retrograde Percutaneous Pinning for Shaft Fracture of Metacarpal Bone: A Case Series January 10, 2024 Unusual Mechanism of Injury during a Wedding Tradition Leading to a Metacarpal Shaft Fracture – A Case Report
January 10, 2024 Unusual Mechanism of Injury during a Wedding Tradition Leading to a Metacarpal Shaft Fracture – A Case Report