
Proper evaluation for prosthesis failure is necessary in patients with new onset instability, recurrent effusions, and early signs of aseptic loosening on radiographs after revision TKA, with surgeons advised to ensure proper prosthesis assembly intra-operatively and follow the zonal fixation concept to optimize construct stability.
Dr. Tarun Jayakumar, Department of Orthopeadic, Sunshine Bone and Joint Institute, Sunshine Hospitals, Hyderabad, Telangana, India. E-mail: tarunjaykumar@gmail.com
Abstract
Introduction: The use of modular implants for revision TKA are ever increasing in number due to their definitive advantage over their monoblock counterparts by providing the surgeon with the versatility needed to achieve equal gaps and manage bone defects. This superiority comes at the cost of certain unique complications attributable to its modular design such as loosening and fractures at the areas of component coupling that are prone to fatigue failure with suboptimal fixation.
Case Report: We present a case of modular femoral component failure in a 59-year man of Asian decent after revision TKA secondary to disengagement and migration of the extension stem locking bolt of a Total Condylar-III prosthesis. Patient presented with pain, effusion, and instability 2.5 years after stage-2 revision TKA. Radiographs revealed migration of the femur-stem locking bolt into the joint cavity. The femoral component and stem were loose. The locking bolt was extracted, and he underwent re-revision surgery with revised femoral components.
Conclusion: Stem-condylar junction of modern modular TKA implants are prone to early loosening and failure. This diagnosis should be anticipated on serial follow-up radiographs and in patients who complain of sudden onset of instability following revision surgery.
Keywords: revision arthroplasty, disengagement, modular total knee arthroplasty, Locking bolt, migration
Revision total knee arthroplasty is often associated with bone loss after removal of the primary prosthesis. Bone defect management and optimization of fixation of revision implants is vital for immediate weight-bearing and longevity of the revision prosthesis. To achieve optimal prosthesis fixation, the zonal concept of fixation was proposed by MorganJones[1,2] which requires the use of modular components to achieve metaphyseal and diaphyseal fixation. Diaphyseal fixation is achieved with the use of femoral or tibial extension stems, which prevent subsidence of the revision components and transfer stress to the diaphysis. However, modular implants can be affected by specific complications of loosening, fractures at modular junctions since the areas of component coupling are prone to fatigue failure with sub-optimal fixation [3-5]. We report a case of modular component failure in a Total Condylar-III (TC-3) prosthesis at the junction of the femoral component and extension stem, with complete disengagement and migration of the femoral locking bolt in the knee joint.
A 59-year-old man with no comorbidities was referred to our centre with a peri-prosthetic joint infection of the knee. Patient initially underwent index TKA for uncomplicated varus deformity of the knee at an outside hospital. Patient had a sinus tract and persistent wound discharge for 30 days post-surgery, when he presented to our institute for which he was confirmed to have periprosthetic joint infection as per MSIS criteria (Fig 1a). Patient was planned for 2-stage revision TKA, and Stage-1 revision was performed with implant removal and placement of an antibiotic cement spacer (Fig 1b). The second stage surgery was performed after eradication of infection 8-weeks later, with the implantation of a Total Condylar III prosthesis (DePuy Johnson and Johnson, Warsaw, Ind) with femoral and tibial extension stems (Fig 2a). The patient had a painless, stable and well-functioning joint for two-and-a-half years after revision surgery. Two-and-a-half years post-revision, patient presented to us with pain, knee effusions and complaints of instability. The pain was insidious in onset and gradually progressive in severity, and classically presented as start-up pain. On examination, he had a varus thrust gait, joint effusion with medial joint line tenderness, along with a palpable “clicking” sensation during passive range of motion of the knee. Radiographs during intermediate (1 year) follow-up appeared normal except for a slightly undersized femoral stem, without evidence of component loosening (Fig. 2b). 
Plain radiographs of the knee at 2.5 years follow-up showed complete disengagement and migration of the modular femoral locking bolt into the knee joint cavity, along with osteolysis around the femoral component and extension stem (Fig. 3). Prosthetic joint infection was ruled out with normal C-reactive protein (CRP), Erythrocyte Sedimentation Rate (ESR) as per MSIS criteria. Re-revision TKA surgery was planned with a diagnosis of a septic loosening secondary to modular femoral implant failure. The knee joint was exposed through medial para-patellar approach. The distal femur screw was found lying freely in the joint cavity (Fig.4a), disengaged from the femoral component (Fig. 4b).

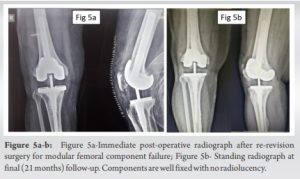
The polyethylene insert showed some delamination No metallosis or synovitis was noted. The femoral component was grossly loose and the extension stem could be easily extracted without any instrumentation. The tibial component was well fixed and did not necessitate revision. The cement mantle of the femoral component and in the medullary canal was removed and the femur prepared for re-implantation with new prosthesis and new wider diameter femur stem (Size 3 TC-3 Modular femur with cemented extension stem). The bone loss did not necessitate the use of femoral sleeves. The immediate post-operative X-ray is shown in Fig. 5a. Patient was mobilized immediately post-surgery and was allowed to bear full weight on the first post-operative day. The immediate post-operative period and early follow-up was uneventful without wound healing complications. At final follow-up of 21 months (1 year, 9 months) patient is walking without pain or instability, with 0-100 degrees active knee ROM.
With the increasing number of primary knee arthroplasty procedures, the revision burden in arthroplasty is also set to increase in the future [6]. Revision knee arthroplasty cases are often associated with bone loss. Studies have shown that optimal management of bone loss to achieve stable implant fixation is essential for longevity of the revision prosthesis [7,8]. Morgan-Jones et al[1]described the zonal concept of implant fixation, to improve construct stability. In most cases, modular components and implants have now become the standard of care in management of revision arthroplasty cases. Modular implants allow surgeons to optimize construct stability and achieve fixation with the use of extension stems, metaphyseal sleeves and cones and augments. However, the modularity of such components may deam it to be a weak link in the prosthesis construct. Although rare, modular implants been associated with unique complication of modular-interface failure including fractures and loosening. These complications are usually the result of high mechanical stress and fatigue failure at the component stem interface [9-11]. Failure at the component-stem interface occurs mainly by two mechanisms. Firstly, there may fatigue failure at the junction secondary to corrosion and mechanical stress. Secondly, the locking bolt may fail or disengage due to improper tightening of the assembly before implantation. The Total Condylar-III revision prosthesis (DePuy, Warsaw, IN) is one of the most commonly used revision implant worldwide. The femoral component is connected to the distal femoral extension stem through a femoral adapter and corresponding femoral adapter bolt or a locking bolt. Due to the high concentration of forces at the stem-condyle junction, complications such as corrosion, fretting, metallic wear, locking bolt loosening and breakage have come to light. There are few articles which have reported bolt loosening and fracture at the stem- condyle junction, with the use of other implant systems. In a study by Westrich et al[12], loosening and migration of the locking screw were reported in 3 cases from the Insall-Burstein II Constrained Condylar Knee (Zimmer, Warsaw, Ind) with press-fit femoral stems. They concluded that faulty component assembly was the main reason for the failure. However, none of the cases in this series had loosening of the femoral component and only one case developed femoral component loosening after isolated locking bolt removal from the joint, which went on to be revised. Nadkarni et al[13] also reported locking bolt disengagement in the Insall-Burstein II (IB-II) prosthesis, with the bolt causing acute locking episode of the knee, requiring revision surgery to remove the offending locking bolt. In 2007, Issack et al[11] reported 2 cases of failure at the taper lock of modular stemmed femoral implant. However, these failures were both secondary to fatigue failure and fracture at the taper junction secondary to aseptic loosening. Both fractures were reported with the Optetrak (Exactech, Gainesville, Florida) system. In these reports, even the tibial component was loose, and the failure occurred secondary to loosening of the entire prosthesis. Lim et al[14] reported 5 cases of locking bolt disengagement from stem-condyle junction of the femur component from the Total Condylar III implant (DePuy Johnson and Johnson, Warsaw, Ind). All of the 5 cases, similarly had dissociation of the locking screw stem-condyle junction but most cases had well-fixed cemented femur stems. All 5 knees underwent re-revision TKR and they concluded by recommending the use of components with morse- taper junctions and preferably nonmodular implants for better outcomes. In our case, the entire femoral component and extension stem showed “debonding” with no cement mantle around the retrieved extension stem which might have been the result of the initial under sizing of the stem contributing to the secondary locking bolt loosening or vice-versa. Ahn et al[15] reported a case with loosening of the locking bolt from a Total Condylar III implant. This case was not associated with complete disengagement and the authors recommend the use of CT scan with metal artifact reduction and adjusted window level-width on the DICOM viewer for better implant visualization. Despite changes to instrumentation and component design over the past decade, there is still a possibility of locking bolt disengagement and modular failure with the TC-III prosthesis. To combat this complication, we recommend taking a few precautions. Firstly, intra-operatively, the surgeon should ensure that the component handed over by the assisting staff is fully tightened and stems should be fitting the diaphysis of the long bones adequately in order to provide long-term stability. Lim et al(14) described the 2- wrench technique, to tighten the femur component with the stem, which was found to increase static retention strength by 150%. Secondly, patients presenting with new onset instability with varus/valgus thrust gait, recurrent effusions, early signs of aseptic loosening on radiographs should be properly evaluated for prosthesis failure. Modular implant failure after TKA remains a rare but challenging complication. Surgeons should ensure proper assembly of the prosthesis prior to implantation and follow the zonal fixation concept during revision surgery, to optimize construct stability.
Stem-condylar junction of modern modular TKA implants are prone to early loosening and failure. This diagnosis of aseptic loosening should be anticipated on serial follow-up radiographs and in patients who complain of instability following revision surgery.
Modular component implant failure after TKA remains a rare but challenging complication. Patients presenting with new-onset instability with varus/valgus thrust gait, recurrent effusions, and early signs of aseptic loosening on radiographs should be properly evaluated for prosthesis failure. Surgeons should ensure proper assembly of the prosthesis before implantation intraoperatively and follow the zonal fixation concept during revision surgery, to optimize construct stability.
References
- 1.Morgan-Jones R, Oussedik SIS, Graichen H, Haddad FS. Zonal fixation in revision total knee arthroplasty. Bone Joint J. 2015 Feb;97-B(2):147–9. [Google Scholar | PubMed]
- 2.Oh JH, Scuderi GR. Zonal Fixation in Revision TKA: The Key Is Metaphyseal Fixation. J Knee Surg. 2021 Nov;34(13):1402-1407. [Google Scholar | PubMed]
- 3.Windsor RE, Scuderi GR, Moran MC, Insall JN. Mechanisms of failure of the femoral and tibial components in total knee arthroplasty. Clin Orthop Relat Res. 1989 Nov;(248):15–20. [Google Scholar | PubMed]
- 4.Whiteside LA. Cementless fixation in revision total knee arthroplasty. Clin Orthop Relat Res. 2006 May;446:140–8. [Google Scholar | PubMed]
- 5.Lee, SH., Shih, HN., Chang, CH. et al. Influence of extension stem length and diameter on clinical and radiographic outcomes of revision total knee arthroplasty. BMC Musculoskelet Disord 21, 15 (2020). [Google Scholar | PubMed]
- 6.Leitner L, Türk S, Heidinger M, et al. Trends and Economic Impact of Hip and Knee Arthroplasty in Central Europe: Findings from the Austrian National Database. Sci Rep. 2018 Mar 16;8(1):4707. [Google Scholar | PubMed]
- 7.Vince KG, Long W. Revision knee arthroplasty. The limits of press fit medullary fixation. Clin Orthop Relat Res. 1995 Aug;(317):172–7. [Google Scholar | PubMed]
- 8.Dalury DF, Pomeroy DL, Gorab RS, Adams MJ. Why are total knee arthroplasties being revised? J Arthroplasty. 2013 Sep;28(8 Suppl):120–1. [Google Scholar | PubMed]
- 9.Conlisk N, Howie CR, Pankaj P. The role of complex clinical scenarios in the failure of modular components following revision total knee arthroplasty: A finite element study. J Orthop Res [Internet]. 2015;33(8):1134–41. [Google Scholar | PubMed]
- 10.Jindal S, Bansal V, Ahmed M. Disengagement of tibial insert locking pin in total knee arthroplasty - A rare failure case report. J Clin Orthop Trauma. 2022 Aug 21;33:101996. [Google Scholar | PubMed]
- 11.Issack PS, Cottrell JM, Delgado S, Wright TM, Sculco TP, Su EP. Failure at the taper lock of a modular stemmed femoral implant in revision knee arthroplasty. A report of two cases and a retrieval analysis. J Bone Joint Surg Am. 2007 Oct;89(10):2271–4. [Google Scholar | PubMed]
- 12.Westrich GH, Hidaka C, Windsor RE. Disengagement of a locking screw from a modular stem in revision total knee arthroplasty. A report of three cases. J Bone Joint Surg Am. 1997 Feb;79(2):254–8. [Google Scholar | PubMed]
- 13.Nadkarni JB, Carden DG. Acute locking in revision total knee arthroplasty due to disengagement of the locking screw. Knee Surg Sports Traumatol Arthrosc. 2005 Apr;13(3):190–2. [Google Scholar | PubMed]
- 14.Lim LA, Trousdale RT, Berry DJ, Hanssen AD. Failure of the stem-condyle junction of a modular femoral stem in revision total knee arthroplasty: a report of five cases. J Arthroplasty. 2001 Jan;16(1):128–32. [Google Scholar | PubMed]
- 15.Ahn JM, Suh JT. Detection of locking bolt loosening in the stem-condyle junction of a modular femoral stem in revision total knee arthroplasty. J Arthroplasty. 2010 Jun;25(4):660.e11-3. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Diagnostic Accuracy of Synovial Alpha-Defensin and Histopathology for Periprosthetic Joint Infection: A Validation Study
May 1, 2026 Diagnostic Accuracy of Synovial Alpha-Defensin and Histopathology for Periprosthetic Joint Infection: A Validation Study April 1, 2026 Migration of Two Broken K-wires into the Cervical Region following Lateral End Clavicle Fixation: A Rare Case Report and Literature Review
April 1, 2026 Migration of Two Broken K-wires into the Cervical Region following Lateral End Clavicle Fixation: A Rare Case Report and Literature Review January 1, 2026 Severe Metallosis-Induced Osteolysis and Polyethylene Liner Dissociation as a Cause of Total Knee Replacement Failure
January 1, 2026 Severe Metallosis-Induced Osteolysis and Polyethylene Liner Dissociation as a Cause of Total Knee Replacement Failure August 1, 2025 Polyethylene Insert Wear Leading to Early Aseptic Bilateral Total Knee Arthroplasty Failure: Case Report
August 1, 2025 Polyethylene Insert Wear Leading to Early Aseptic Bilateral Total Knee Arthroplasty Failure: Case Report