
Consider further investigations and revision of the diagnosis if empirical therapy is not effective in cases of paraplegia.
Dr. Lokesh Raghav, Department of Orthopaedics, Lady Hardinge Medical College, New Delhi, India. E-mail: lokeshraghav10@gmail.com
Introduction: Chondrosarcoma of rib encroaching spine and subsequently leading to paraplegia has never been reported in the literature. Association of paraplegia can often lead to misdiagnosis with a common disease like breast cancer or Potts spine causing a significant delay in treatment.
Case Report: We describe a case of a 45-year-old male with chondrosarcoma of rib with paraplegia who was misdiagnosed initially as Pott’s spine and was started empirically on anti-tubercular treatment for paraplegia and chest wall mass. Further work up at tertiary care center including detailed imaging and biopsy revealed features of chondrosarcoma. However, before any definitive treatment could be done; the patient passed away.
Conclusion: Empirical treatment of paraplegia with chest wall mass for more common diseases like tuberculosis are often initiated without obtaining appropriate radiological and tissue diagnosis. This can lead to a delay in diagnosis and initiation of treatment.
Keywords: Chondrosarcoma, thoracic neoplasm, tuberculosis spinal, paraplegia.
Chondrosarcoma is the most common primary malignancy of the chest wall but in routine clinical practices, it is encountered relatively rarely [1]. The diagnosis and management of chest wall tumors are resource intensive. Very high quality of care and a multidisciplinary approach is often required as they have a tendency to involve surrounding vital structures such as the great vessels, lung, colon, and spine. There are often instances where the tumor may mimic another disease such as breast cancer, metastasis, and tuberculosis, often delaying the diagnosis and appropriate management [2, 3, 4]. Moreover, paraplegia as a complication of encroachment chest wall chondrosarcoma has not been reported in the literature which further increases the chance of misdiagnosis. We present a case of a 45-year-old male with chondrosarcoma of the chest wall who presented with gradual onset paraplegia in our casualty. The consent for publication was taken from the patient at the time of admission.
A 45-year-old male manual laborer presented to the casualty with complete paraplegia of 1 month duration and loss of bowel and bladder control for the past 7 days. The patient was apparently well 4 months ago when he developed weakness in both the lower limbs. The weakness was progressive in nature and over the past 2 months, it had limited the patient’s activities of daily living making him dependent on family members. He noticed a swelling in the right chest wall which was also progressively increasing for the past 4 months. He also had constitutional symptoms. The patient had been started empirically on antitubercular therapy (ATT) 1 month before presentation by a local practitioner based on X-ray and clinical impressions. Despite 1 month of ATT, the condition of the patient worsened and before higher radiological investigation including magnetic resonance imaging (MRI) could have been done by primary treating doctor, the patient presented to our casualty with complete loss of movement of bilateral lower limb with loss of bowel and bladder control. On examination, the patient was severely dehydrated and cachectic. His weight and weight were 173 cm and 45 kg, respectively. There was a 3 × 3 cm mass over the right chest wall which was, variegated, immobile, and not adherent to the overlying skin. The local temperature around the swelling was also increased. Neurological examination revealed spastic tone in both lower limbs; muscle power was 0/5 as per Medical Research Council grading in all muscle groups of both the lower limb. The patient had altered sensations below D5 dermatome and complete loss of sensations below L1 dermatome. Knee and ankle jerks were exaggerated and ankle clonus was present. There was loss of bowel and bladder control. On hematological examination, the patient had anemia (Hemoglobin 7.9) with increased Erythrocyte Sedimentation rate (70/h) and C-reactive protein (80 mg/L). He also had hyponatremia (128 mEq/L) and hyperkalemia (6 mEq/L) with some Electrocardiography changes. Serum urea and creatinine levels were also increased (75 mg/dL and 1.3 mg/dL respectively). He was admitted to ward and intravenous fluids started and medical management was initiated to correct the dyselectrolytemia. Plain radiograph of the dorsolumbar spine revealed a heterogeneous opacity in the right lung field extending from D7 to D9 (Fig. 1). 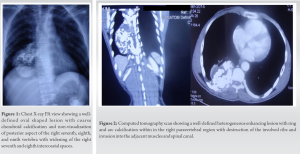 Computed tomography (CT) and MRI scans were done to characterize the mass which showed destruction of the rib and vertebra with internal calcifications suggestive of chondrosarcoma (Figs. 2, 3, 4). Mass arising from the rib appeared to encroach the spinal canal damaging the pedicle and lamina of vertebra leading to extradural compression of cord. CT-guided tissue biopsy was done and histopathological examination confirmed the diagnosis of chondrosarcoma which was of moderate grade. The patient was planned for surgical excision and canal decompression after optimization of parameters. However, on the 16th day of admission, he suffered a sudden cardiorespiratory arrest and he could not be revived. The relatives refused for an autopsy limiting the further investigation of mass lesion.
Computed tomography (CT) and MRI scans were done to characterize the mass which showed destruction of the rib and vertebra with internal calcifications suggestive of chondrosarcoma (Figs. 2, 3, 4). Mass arising from the rib appeared to encroach the spinal canal damaging the pedicle and lamina of vertebra leading to extradural compression of cord. CT-guided tissue biopsy was done and histopathological examination confirmed the diagnosis of chondrosarcoma which was of moderate grade. The patient was planned for surgical excision and canal decompression after optimization of parameters. However, on the 16th day of admission, he suffered a sudden cardiorespiratory arrest and he could not be revived. The relatives refused for an autopsy limiting the further investigation of mass lesion.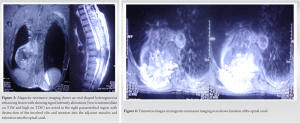
Chondrosarcoma occurs commonly in long bones and pelvis [5]. Due to its relative rarity, its often not suspected when it involves the chest wall. The tumor can be often confused with more common pathology involving the chest wall such as breast carcinoma and metastasis [3, 4]. It often presents between the age of 30 and 50 years as a slowly painless mass which progressively becomes painful [6]. On plain radiography, they appear as an abnormal shadow which requires a detailed work up, which is often very resource extensive for the patient. Most chondrosarcomas are of lower grade which often do not metastasize. Wide surgical resection of the tumor has been shown to be effective. Post excision and 5-and 10-year survival rate of patients are also high. Five-year survival rates have been reported to be 90% for primary disease with a local recurrence rate of 17% and metastasis rate of 12%. Ten-year survival for high grade chondrosarcoma has been reported to be 40–70% [7, 8, 9, 10, 11, 12]. Our patient presented with lower limb weakness, constitutional complaints, and chest wall mass. This often is a common presentation of extrapulmonary/spinal tuberculosis which is a prevalent disease in developing countries. This rare combination of clinical features, that is, chest wall with paraplegia not only led to misdiagnosis at outset rather ultimately led to a fatal outcome. The patient was started on anti-tubercular treatment empirically by the primary treating doctor assuming Potts’s spine as the diagnosis. When the patient presented to us, we performed an MRI, the findings of which surprised our team too, changing the complete course of management. This situation is often very common among young doctors practicing in peripheral regions that treatment for more common disease is started at the outset and response is awaited due to which rare entities are missed. Many patients may struggle for months with no improvement. Final diagnosis could usually be sought when patient comes to a tertiary care center seeking medical treatment. Usually by this time, the disease also reaches an advanced stage and management becomes more complicated. An early and prompt diagnosis and appropriate management could have improved the prognosis of such patient drastically which can only be achieved if such rare disorders will be kept in mind which managing such patients. Chest wall tumors are a relatively rare entity and can be misdiagnosed as tuberculosis especially in developing countries. Keeping vigilant regarding the clinical condition of the patient and the response management may indicate need for further assessment or a revisiting the diagnosis made at the outset.
Chondrosarcoma of the chest wall causing paraplegia has not been reported in literature. It can be misdiagnosed as extrapulmonary tuberculosis especially in a setting with limited resources. A detailed investigation of the patient at initial work up can detect such rare occurrences and may improve outcomes. The possibility of chondrosarcoma or other chest wall tumors should be considered as a differential while managing a patient of chest wall mass with unusual associated symptoms of paraplegia.
Empirical therapy is often started for commonly perceived complaints without obtaining a definitive diagnosis. While it often proves to be beneficial considering the time and financial costs to the patients, it can have devastating consequences for less common disorders as it inevitably causes delay in diagnosis and initiation of appropriate treatment as highlighted in this case report.
References
- 1.Arnold PG, Pairolero PC. Chest-wall reconstruction: An account of 500 consecutive patients. Plast Reconstr Surg 1996;98:804-10. [Google Scholar]
- 2.Balasubramaniyan M, Verma S, Dhawan SR, Saxena AK. Chest wall tuberculosis in children: A mimicker of bone tumour. BMJ Case Rep 2021;14:e242802. [Google Scholar]
- 3.Matsuoka K, Ueda M, Miyamoto Y. Costal chondrosarcoma requiring differential diagnosis from metastatic tumor. Asian Cardiovasc Thorac Ann 2017;25:154-6. [Google Scholar]
- 4.Tounsi N, Zemni I, Abdelwahed N, Jbir I, Charfi L, Nasser RB, et al. Costal chondrosarcoma mimicking a breast cancer: Case report and review of literature. Int J Surg Case Rep 2019;56:37-9. [Google Scholar]
- 5.Dorfman HD, Czerniak B. Bone cancers. Cancer 1995;75(Suppl 1):203-10. [Google Scholar]
- 6.Thomas M, Shen KR. Primary tumors of the osseous chest wall and their management. Thorac Surg Clin 2017;27:181-93. [Google Scholar]
- 7.Burt M, Fulton M, Wessner-Dunlap S, Karpeh M, Huvos AG, Bains MS, et al. Primary bony and cartilaginous sarcomas of chest wall: Results of therapy. Ann Thorac Surg 1992;54:226-32. [Google Scholar]
- 8.Fiorenza F, Abudu A, Grimer RJ, Carter SR, Tillman RM, Ayoub K, et al. Risk factors for survival and local control in chondrosarcoma of bone. J Bone Joint Surg Br 2002;84:93-9. [Google Scholar]
- 9.McAfee MK, Pairolero PC, Bergstralh EJ, Piehler JM, Unni KK, McLeod RA, et al. Chondrosarcoma of the chest wall: Factors affecting survival. Ann Thorac Surg 1985;40:535-41. [Google Scholar]
- 10.Roos E, van Coevorden F, Verhoef C, Wouters MW, Kroon HM, Hogendoorn PC, et al. Prognosis of primary and recurrent chondrosarcoma of the rib. Ann Surg Oncol 2016;23:811-7. [Google Scholar]
- 11.van Geel AN, Wouters MW, Lans TE, Schmitz PI, Verhoef C. Chest wall resection for adult soft tissue sarcomas and chondrosarcomas: Analysis of prognostic factors. World J Surg 2011;35:63-9. [Google Scholar]
- 12.Wouters MW, van Geel AN, Nieuwenhuis L, van Tinteren H, Verhoef C, van Coevorden F, et al. Outcome after surgical resections of recurrent chest wall sarcomas. J Clin Oncol 2008;26:5113-8. [Google Scholar]






