
Bilateral metatarsal stress fractures are a very uncommon event and when it occurs, foot deformity and osteoarthritis should be investigated.
Dr. Giulia Rescigno, Department of Trauma and Orthopaedics, Sant’Andrea Hospital, Sapienza University of Rome, Rome, Italy. E-mail: giuliarescigno@gmail.com
Abstract
Introduction: Metatarsal stress fractures typically occur in the second and third metatarsus metaphysis, with only rare cases in the fourth and first. The main factors influencing its onset are repetitive stress from prolonged training, biomechanical factors and bone weakness. There is only a paucity of literature documenting first metatarsal stress fractures; the authors present a rare bilateral first metatarsal stress fracture.
Case Report: A Caucasian 52-years-old amateur female runner with no other risk factors or medical condition was admitted in our institute with complaints of severe bilateral forefoot pain for 2 weeks arisen after a 20 km run of an amateur race. The patient presented bilateral hallux valgus (HVA) and advanced osteoarthritis of the first metatarsal-phalangeal joint, which is not usually considered a biomechanical risk factor for metatarsal stress fractures. Radiographs of both feet showed linear sclerosis, perpendicular to the diaphysis of the first metatarsal, approximatively in the half of the bone. Signs of osteoarthritis of the first metatarsal-phalangeal were also detected bilaterally. The patient was treated with rest, bilateral post-operative rocker sole shoes that she has worn for 6 weeks, cryotherapy, analgesics as needed and pulsed electromagnetic fields for 8 h per day for 40 days with a complete resolution of symptoms and the previous radiological findings.
Conclusion: The authors believed that the bilateral HVA condition could be considered an indirect sign of overuse, and it may be investigated and eventually treated as a responsible for this pathologic condition.
Keywords: Stress fracture, first metatarsal, pulsed electromagnetic fields.
Metatarsal stress fractures are the most common stress fracture in the foot. They typically involve athletes, soldiers, and ballet dancers and represent up to 22.5% of all stress fractures; Metatarsal stress fractures are caused by repetitive stress and were first described in 1985 and are also known as “March fractures,” because of Prussian soldiers who suffered this injury as they used to practice long marches [1,2,3,4,5,6]. Metatarsal fractures represent 5–6% of fractures encountered in primary care [7]. Most metatarsal stress fractures occur in the second or third metatarsal, with fewer occurring in the fourth metatarsal [8]. The first metatarsal is rarely involved in this kind of lesion, accounting for less than 8% of all metatarsal stress fractures; When they occur, they have a typically metaphyseal location [5,9]. The most common location of metatarsal stress fractures in the second metatarsal neck; it is due to low flexibility and the higher torsional forces given by its strong ligamentous attachment to the first and second cuneiforms [10]. Bone stress injuries result from repetitive stresses, which may be created by prolonged training and overuse and can be influenced by weight distribution on foot. Precipitating factors are repetitive traumas, rapid uncontrolled muscular forces, and pathologic bone weakness [11,12]. The forefoot has unique biomechanical features: Loads are distributed asymmetrically across the bones; Griffin and Richmond have shown that the second, third, and fourth metatarsals have the weakest geometrical properties; moreover, the second and third metatarsals usually experience high relative peak pressures [13]. Biomechanical factors associated with multiple stress fractures include high longitudinal arch of the foot, leg-length discrepancy or lower limb malalignment, and forefoot varus [14,15,16]. Runners and militaries with high weekly training mileage are at risk for lower extremities’ initial and recurrent stress fractures. Non-modifiable risk factors also include female sex, increased age, and race [16]. Half of all female patients with stress fractures have menstrual irregularities; hormone changes influence bone metabolism, leading to stress fractures [17]. Here, the authors report a rare bilateral simultaneous fist metatarsal fracture as in the literature, only one other case is reported [18].
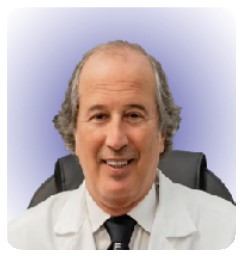
A 52-year-old female lawyer, Caucasian, came to our clinic complaining of bilateral forefoot pain for 2 weeks. Her referred symptoms have arisen after a 20 km run of an amateur race. She was used to running 10 km per week as an amateur runner. She denied any relevant trauma or joint sprain. She described the pain increasing during walking or jumping and decreasing at rest. She was ambulatory without any supporting tools. She had been taking non-steroidal anti-inflammatory drugs with mild benefits. The patient had no relevant medical history, and she was not taking any other medications or supplements. On physical examination, she had local swelling without erythema over the first metatarsal dorsum bilaterally, especially on the medial side. Tenderness to palpation was noted in this area as well. She suffered moderate pain during gait and the flexion and extension of the first metatarsal-cuneiform (Lisfranc’s) joint. The pain did not modify with ankle or significant toe motion, neither passive nor active. She had a bilateral unpainful, non-rigid hallux valgus (HVA), more pronounced on the left foot. No other foot deformity was detected. She was 165 cm tall and weighed 56 kg (body mass index 20.6 kg/m2). X-ray of both feet showed linear sclerosis, perpendicular to the diaphysis of the first metatarsal, approximatively in the half of the bone. Signs of osteoarthritis of the first metatarsal-phalangeal were also detected bilaterally. HVA bilateral was confirmed (on the left foot, HVA angle 25° and intermetatarsal angle (IMA) 16°, on the right foot HVA 27° and IMA 12°) (Fig. 1). 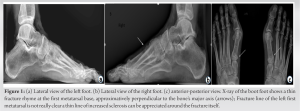 In the left foot, magnetic resonance imaging (MRI) revealed a fracture at the base of the first metatarsal with bone marrow edema extending from the base into the shaft, consistent with a stress fracture (Fig. 2). In the right foot, MRI showed a fracture of the dorsal base of the first metatarsal with associated bone marrow edema. The radiologist also noted bone bruising of the first cuneiform posteriorly (Fig. 3). It is possible to appreciate initial radiological sign of osteoarthritis of the fist metatarsal-phalangeal joint (subchondral sclerosis and narrowing of the joint space) The patient was treated with bilateral post-operative rocker sole shoes that she has worn for 6 weeks. Then, she transitioned to rigid sole shoes. She was allowed to walk with free weight-bearing. She was also instructed to use cryotherapy and prescribed analgesics as needed. Pulsed electromagnetic fields (PEF) were also prescribed; the device used was BIOSTIM (IGEA, Carpi, Italy), which generates pulses 1.3 milliseconds in duration, with a frequency of 75 Hz. She underwent PEF for 8 h per day for 40 days. Sports activities were restricted for 1 more month. After an overall period of 10 weeks, a new MRI showed a complete resolution of the previous finding; at the clinical evaluation, no symptoms were recorded. The patient returned to sport with no limitation. No specific shoes were suggested. At the last follow-up, 1 year after the injury, she reported no problem, and she reports that she has returned to running and practicing sport at the same level she had before the fractures. At the last follow-up, she was given the American Orthopaedic Foot and Ankle Society Hallux Metatarsophalangeal-Interphalangeal questionnaire [19], and the scores obtained were 93 for both sides underlying an excellent resumption of patients’ daily life activities [19].
In the left foot, magnetic resonance imaging (MRI) revealed a fracture at the base of the first metatarsal with bone marrow edema extending from the base into the shaft, consistent with a stress fracture (Fig. 2). In the right foot, MRI showed a fracture of the dorsal base of the first metatarsal with associated bone marrow edema. The radiologist also noted bone bruising of the first cuneiform posteriorly (Fig. 3). It is possible to appreciate initial radiological sign of osteoarthritis of the fist metatarsal-phalangeal joint (subchondral sclerosis and narrowing of the joint space) The patient was treated with bilateral post-operative rocker sole shoes that she has worn for 6 weeks. Then, she transitioned to rigid sole shoes. She was allowed to walk with free weight-bearing. She was also instructed to use cryotherapy and prescribed analgesics as needed. Pulsed electromagnetic fields (PEF) were also prescribed; the device used was BIOSTIM (IGEA, Carpi, Italy), which generates pulses 1.3 milliseconds in duration, with a frequency of 75 Hz. She underwent PEF for 8 h per day for 40 days. Sports activities were restricted for 1 more month. After an overall period of 10 weeks, a new MRI showed a complete resolution of the previous finding; at the clinical evaluation, no symptoms were recorded. The patient returned to sport with no limitation. No specific shoes were suggested. At the last follow-up, 1 year after the injury, she reported no problem, and she reports that she has returned to running and practicing sport at the same level she had before the fractures. At the last follow-up, she was given the American Orthopaedic Foot and Ankle Society Hallux Metatarsophalangeal-Interphalangeal questionnaire [19], and the scores obtained were 93 for both sides underlying an excellent resumption of patients’ daily life activities [19].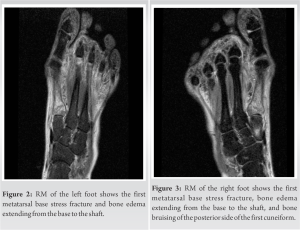
A first metatarsal stress fracture is an unusual diagnosis and there is only one other case in the literature reporting a bilateral condition in a young athlete [18]. Stress fractures of the first metatarsal occur in the cancellous bone at the base near the medial cuneiform as it occurred with this case [20]. March fractures usually occur in militaries or athletes because they are typically subjected to cyclic overload that is not properly the patient’s condition. Even if she was an amateur runner, her activity level seems not high enough to justify the fractures, as a deficit of Vitamin D, low body mass density, and menstrual disorders can play their role in the pathophysiology of stress fractures, the patient was also prescribed an endocrinological examination, which did not show any pathological condition [10]. In the author’s opinion, it is crucial to consider the HVA and the advanced osteoarthritis of the first metatarsal-phalangeal joint, which can be considered an indirect sign of overuse; those two conditions could have played a role in the pathogenesis [21]. Even if the patient had no symptoms due to her HVA, it could be interesting to investigate if the correction of HVA could have prevented, somehow, these fractures.
Although uncommon, first metatarsal stress fractures can occur in a non-high-risk population and could be bilateral. This case report highlights the risk of first metatarsal stress fractures in a non-common high-risk population, which, however, present as a risk factor for an asymptomatic HVA with significant osteoarthritis of the first metatarsal-phalangeal joint.
Diagnosing a metatarsal stress fracture can be challenging. First metatarsal stress fractures’ risk factors commonly admitted are cyclic overload, deficit of Vitamin D, low body mass density, and menstrual disorders. In the author’s opinion, it is crucial to consider two more conditions that could play a role in the pathogenesis: The HVA and the advanced osteoarthritis of the first metatarsal-phalangeal joint, which can be considered an indirect sign of overuse. A detailed evaluation is essential.
References
- 1.Chuckpaiwong B, Cook C, Pietrobon R, Nunley JA. Second metatarsal stress fracture in sport: Comparative risk factors between proximal and non-proximal locations. Br J Sports Med 2007;41:514-4. [Google Scholar | PubMed]
- 2.Gehrmann RM, Renard RL. Current concepts review: Stress fractures of the foot. Foot Ankle Int 2006;27:750. [Google Scholar | PubMed]
- 3.Hulkko A, Orava S. Stress fractures in athletes. Int J Sports Med 1987;8:221-6. [Google Scholar | PubMed]
- 4.Rammelt S, Heineck J, Zwipp H. Metatarsal fractures. Injury 2004;35:SB77-86. [Google Scholar | PubMed]
- 5.Queen RM, Crowder TT, Johnson H, Ozumba D, Toth AP. Treatment of metatarsal stress fractures: Case reports. Foot Ankle Int 2007;28:506-10. [Google Scholar | PubMed]
- 6.Briethaupt M. To the pathology of the humanfoot. Med Zeitung 1855;24:169-71, 175-7. [Google Scholar | PubMed]
- 7.Hatch RL, Rosenbaum CI. Fracture care by family physicians. A review of 295 cases. J Fam Pract 1994;38:238-44. [Google Scholar | PubMed]
- 8.Mandell JC, Khurana B, Smith SE. Stress fractures of the foot and ankle, part 2: Site-specific etiology, imaging, and treatment, and differential diagnosis. Skeletal Radiol 2017;46:1165-86. [Google Scholar | PubMed]
- 9.Levy JM. Stress fractures of the first metatarsal. Am J Roentgenol 1978;130:679-81. [Google Scholar | PubMed]
- 10.Pegrum J, Dixit V, Padhiar N, Nugent I. The pathophysiology, diagnosis, and management of foot stress fractures. Phys Sportsmed 2014;42:87-99. [Google Scholar | PubMed]
- 11.Sterling JC, Calvo RD, Holden SC. An unusual stress fracture in a multiple sport athlete. Med Sci Sports Exerc 1991;23:298-303. [Google Scholar | PubMed]
- 12.Mert M, Unkar EA, Ozluk AV, Tuzuner T, Erdoğan S. Multiple simultaneous metatarsal stress fractures in the same foot. J Am Podiatr Med Assoc 2015;105:177-80. [Google Scholar | PubMed]
- 13.Griffin NL, Richmond BG. Cross-sectional geometry of the human forefoot. Bone 2005;37:253. [Google Scholar | PubMed]
- 14.Korpelainen R, Orava S, Karpakka J, Siira P, Hulkko A. Risk factors for recurrent stress fractures in athletes. Am J Sports Med 2001;29:304-10. [Google Scholar | PubMed]
- 15.Theodorou DJ, Theodorou SJ, Boutin RD, Chung C, Fliszar E, Kakitsubata Y, et al. Stress fractures of the lateral metatarsal bones in metatarsus adductus foot deformity: A previously unrecognized association. Skeletal Radiol 1999 28:679-84. [Google Scholar | PubMed]
- 16.Jacobs JM, Cameron KL, Bojescul JA. Lower extremity stress fractures in the military. Clin Sports Med 2014;33:591-613. [Google Scholar | PubMed]
- 17.Warren MP, Brooks-Gunn J, Fox RP, Lancelot C, Marzouki Y, Souissi W, et al. Lack of bone accretion and amenorrhea: Evidence for a relative osteopenia in weight-bearing bones. J Clin Endocrinol Metab 1991;72:847-53. [Google Scholar | PubMed]
- 18.Metz JP. Bilateral first metatarsal stress fractures in a field hockey player. Phys Sportsmed 2005;33:50-8. [Google Scholar | PubMed]
- 19.Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int 1994;15:349-53. [Google Scholar | PubMed]
- 20.Lucas MJ, Baxter DE. Stress fracture of the first metatarsal. Foot Ankle lnt 1997;18:373-4. [Google Scholar | PubMed]
- 21.Kennedy JG, Collumbier AJ. Bunions in dancers. Clin Sports Med 2008;27:321-8. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Malleolar Stress Fracture as the First Manifestation of Undiagnosed Crohn’s Disease: A Case Report
June 1, 2026 Malleolar Stress Fracture as the First Manifestation of Undiagnosed Crohn’s Disease: A Case Report June 1, 2026 A Rare Case of Giant Cell Tumor of the First Metatarsal: En Bloc Resection and Fibular Autograft Reconstruction
June 1, 2026 A Rare Case of Giant Cell Tumor of the First Metatarsal: En Bloc Resection and Fibular Autograft Reconstruction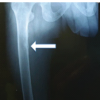 December 1, 2025 Adult-Onset Fanconi Syndrome Presenting as Stress Fractures: A Case Report
December 1, 2025 Adult-Onset Fanconi Syndrome Presenting as Stress Fractures: A Case Report September 1, 2025 Calcaneus and Traumatic Stress Fracture
September 1, 2025 Calcaneus and Traumatic Stress Fracture