
Etiology and management of spontaneous neck of femur fracture.
Dr. Duwarkesh B Kavlekar, Department of Orthopaedic Surgery, Goa Medical College, Bambolim, Goa, India. E-mail: duwa.kavlekar@gmail.com
Introduction: Spontaneous bilateral neck femur fracture occurs following many conditions. It is very rare event. It can be seen in young, middle aged, and elderly people with no preceding trauma. We report a case in middle aged person who got fracture secondary to chronic liver disease and Vitamin D3 deficiency and who underwent bilateral hemiarthroplasty.
Case Report: A 46-year-old man came with sudden onset of bilateral hip pain with no history of trauma. It was started with difficulty in moving the left lower limb since February 2020 and after about 1-month period patient got right hip pain which made the patient completely bedridden. He also complained of yellowish discoloration of eyes associated with weight loss, malaise. No history of tremors in hand. No history of seizures.
Conclusion: It is a not a common condition. Spontaneous bilateral neck femur fracture occurs following chronic liver disease and Vitamin D3 deficiency. Both these conditions lead to increase osteoporosis and osteomalacia thus making it more susceptible to fracture.
Keywords: Spontaneous, bilateral, chronic liver disease, Vitamin D3, neck femur.
Spontaneous bilateral neck femur fracture is very rare event. In chronic liver disease due to complication of osteoporosis, it results in high fragility fractures. It significantly affects the quality of life. The prevalence of osteoporosis in patients with cirrhosis is approximately 12–55% higher than in healthy people. Notably, up to 40% of patients with chronic liver disease may experience a fracture [1]. Vitamin D3 deficiency is now recognized as pandemic [2]. It also results in osteoporosis thus precipitated it and resulting in atraumatic fractures. Vitamin D3 is hydroxylated in the liver to 25-hydroxy vitamin D (25-OH-vitamin D) and then in the kidneys to 1, 25-hydroxyvitamin D. Decreased 25-OH-vitamin D production is associated with altered liver function which results in impaired osteoclast-mediated bone resorption, impaired osteoblast-mediated mineralization and decreased calcium resorption in the gastrointestinal tract [3, 8, 9, 10].
A 46-years-old man came with sudden onset of bilateral hip pain with no history of trauma. It was started with difficulty in moving the left lower limb since February 2020 and after about 1-month period patient got right hip pain which made the patient completely bedridden. He also complained of yellowish discoloration of eyes associated with weight loss, malaise. No history of tremors in hand. No history of seizures. He was a known case of diabetes mellitus on antidiabetic medications for the past 5 years and known habit of drinking alcohol for many years. Patient was admitted for fracture bilateral neck femur in our hospital. There was a curiosity to find the cause of this spontaneous fracture which resulted in subjecting the patient to multiple invasive as well as non-invasive tests which has been shown below. On examination, there was striking feature of icterus and anemia. Investigation revealed Hb of 9.1 g%, PCV 26%, Platelets count 1 lakh. Liver function tests (LFTs) were deranged with total serum bilirubin of 5.6 mg/dL (n = 0.3–1.2). SGOT and SGPT were high. A/G ratio reversed −2.0/4.2. Se calcium was raised 12 (9–11 mg/dL). Se 25 OH VIT D was low 7.0 (n = 20–50 ng/mL). Se vit D 1,25-Dihydroxy found to be low <5.00 (n = 19.9–79.3 pg/mL). Se PTH was low 11.1 (n = 15–68.3 pg/mL). Same time malignancy was ruled out by doing. Bone marrow aspiration which showed emperipolesis by megakaryocytes with mild hyperplasia of myeloid series and mild shift to left. No evidence of malignancy. Ct scan thorax and abdomen revealed features of cirrhosis of liver and likely to represent metabolic bone disease like osteomalacia rather than metastasis. It also revealed old healed fractures of dorsal vertebrae and rib fractures. In our setting, there was no bone mineral density test done in our hospital and since patient was not affordable could not get it done from private. Other investigation like ECG, 2DECHO, and ABG was normal. Patient was diagnosed as spontaneous bilateral neck femur fracture secondary to chronic liver disease and Vitamin D3 deficiency. Treatment was started with medications for liver disease and doses of Vitamin D3. Following which LFTs started improving and Serum ca came to normal. As a result, with endocrine consultation, we did not start any PTH hormone replacement therapy and patient was not affordable too. Finally, decision of B/L Hemiarthroplasty was taken and patient was operated on March 25, 2020, under combined spinal epidural anesthesia. Patient was operated one hip at a time in lateral position with cemented bipolar prosthesis, followed by other hip with change in position with cemented bipolar prosthesis in same setting. Following post-operative day 1, patient was put on LMW enoxaparin subcutaneously, Vitamin D3 dose and injection zoledronic acid dose was given. Physiotherapy was started with static quadriceps exercises and full weight bearing was started on post-operative day 4 as patient tolerated pain. Patient was discharged after stitch removal (post-operative day 14) and called for follow-up after 1 month. After 3 months of time, patient came to OPD walking without walker. In august, patient resumed back to his work. Patient was follow-up for further time period at 6 months, 12 months, and 24 months with minimal symptoms but with symptomatic treatment, he was able to do his work.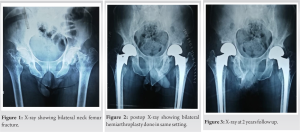
Bilateral neck femur fracture without preceding trauma is very rare injury. There are many causes wherein it occurs in patients following osteomalacia, primary hyperparathyroidism, renal osteodystrophy, and similar metabolic bone disease [5]. It has also been associated with pregnancy, pelvic irradiation, and the use of corticosteroid and antacid drugs [4, 5]. Before in 1960s, such injuries were also attributed to violent muscular contractions following seizures [11]. Since then, this pattern of injury is reported as high energy trauma. Other cases include amenorrheic athletes and patient who has received fluoride treatment also has been reported. In another study, it is mention that alteration in normal leg axis following post bilateral total knee prosthesis also developed spontaneous femoral fractures [12]. In Marfans syndrome, patient with bilateral protrusio acetabulli also has shown similar case. It can present as bilateral groin pain with X-rays may be normal initially and higher suspicion is needed to diagnose these cases. The literature suggests that patients usually complain of bilateral groin or thigh pain that persists over a period of a few weeks to several months [6]. In the present case scenario, we clearly make out from X-ray; hence, MRI or CT scan was needed. In our study, the cause of spontaneous bilateral fracture femur was due to chronic liver disease following alcohol abuse which leads to osteoporosis and Vitamin D deficiency osteomalacia. To improve the prognosis in this rare and serious condition, diagnosing and treating the underlying etiology of osteoporosis and osteomalacia are essential.
It is a not a common condition. Spontaneous bilateral neck femur fracture occurs following chronic liver disease and Vitamin D3 deficiency. Both these condition leads to increase osteoporosis and osteomalacia thus making it more susceptible to fracture.
It is important to have knowledge regarding this case in terms of treating liver cirrhosis and Vitamin D3 deficiency and anticipate fracture in future and thus help in prophylactically to prevent fracture by taking necessary precautions.
References
- 1.Jeong HM, Kim DJ. Bone diseases in patients with chronic liver disease. Int J Mol Sci 2019;20:4270. [Google Scholar]
- 2.Desai M, Nadkarni S. Spontaneous bilateral fracture neck of femur secondary to Vitamin D deficiency: A case report. Clin Cases Miner Bone Metab 2015;12:282-4. [Google Scholar]
- 3.Handzlik-Orlik G, Holecki M, Wilczyński K, Duława J Osteoporosis in liver disease: Pathogenesis and management. Ther Adv Endocrinol Metab 2016;7:128-35. [Google Scholar]
- 4.Kalaci A, Yanat AN, Sevinç TT, Doğramaci Y. Insufficiency fractures of both femoral necks in a young adult caused by osteoporosis: A case report. Arch Orthop Trauma Surg 2008;128:865-8. [Google Scholar]
- 5.Nagao S, Ito K, Nakamura I. Spontaneous bilateral femoral neck fractures associated with a low serum level of Vitamin D in a young adult. J Arthroplasty 2009;24:322.e1-4. [Google Scholar]
- 6.Chadha M, Balain B, Maini L, Dhal A. Spontaneous bilateral displaced femoral neck fractures in nutritional osteomalacia--a case report Acta Orthop Scand 2001;72:94-6. [Google Scholar]
- 7.Duckworth AD, Bennet SJ, Aderinto J, Keating JF. Fixation of intracapsular fractures of the femoral neck in young patients: Risk factors for failure. J Bone Joint Surg Br 2011;93:811-6. [Google Scholar]
- 8.Ross AC, Manson JE, Abrams SA, Aloia JF, Brannon PM, Clinton SK, et al. The 2011 report on dietary reference intakes for calcium and Vitamin D from the Institute of Medicine: What clinicians need to know. J Clin Endocrinol Metab 2011;96:53-8. [Google Scholar]
- 9.Robinson CM, Court-Brown CM, McQueen MM, Christie J. Hip fractures in adults younger than 50 years of age. Epidemiology and results. Clin Orthop Relat Res 1995;312:238-46. [Google Scholar]
- 10.Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, treatment, and prevention of Vitamin D deficiency: An Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2011;96:1911-30. [Google Scholar]
- 11.McGoldrick NP, Dodds MK, Green C, Synnott K. Management of simultaneous bilateral neck of femur fractures in an elderly patient. Geriatr Orthop Surg Rehabil 2013;4:71-3. [Google Scholar]
- 12.Gurdezi S, Trehan RK, Rickman M. Bilateral undisplaced insufficiency neck of femur fractures associated with short-term steroid use: A case report. J Med Case Rep 2008;2:79. [Google Scholar]





