
Arthroscopic excision with a tailored rehabilitation will result in excellent pain relief and a return to full sporting activity in case of a symptomatic bipartite patella.
Dr. Vivek Anbarasan, Department of Arthroscopy and Sports Medicine, Sri Ramachandra Institute of Higher Education and Research No. 1, Ramachandra Nagar, Porur, Chennai, Tamil Nadu, India. E-mail: vivekanbarasan@gmail.com
Abstract
Introduction: Bipartite patella is usually an asymptomatic anatomical variant estimated to have a prevalence of 0.2–6% in an adult population.
Case Report: A 28-year-old league-level football player presented with the left anterior knee pain of 6 months duration. Imaging studies revealed bilateral bipartite patella. Arthroscopic excision of the fragment was performed following which he returned to play 6 weeks after accelerated sports-specific rehabilitation. Atraumatic knee pain should raise suspicion of the bipartite patella. Surgical intervention plays a key role in patients with refractory pain after careful exclusion of other causes of anterior knee pain.
Conclusion: Arthroscopic excision is preferred in the case of a high-demand athlete to accelerate recovery and fasten the return to sport duration.
Keywords: Patellofemoral pain, overuse injury, return to sports, arthroscopic surgery.
Bipartite patella is usually an asymptomatic anatomical variant estimated to have a prevalence of 0.2–6% in an adult population [1]. Despite it being an incidental finding in most cases, it becomes one of the causes of anterior knee pain in symptomatic individuals. The pain related to overuse/sporting activities can be attributed to excessive traction over the fibrous articulation of the bipartite fragment. We present a successful case of a league-level international footballer with a bipartite patella, managed by an arthroscopic, and tailored rehabilitation program aiding in the early return to sports.
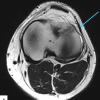
A 28-year-old professional male footballer with 18 training years and with body mass index of 23.2 presented with complaints of atraumatic left anterior knee pain for 6 months. He had intermittent disabling pain, aggravated on training and playing which limited his field time, and significantly affected his performance. The athlete had no complaints of knee swelling, instability, or mechanical symptoms. On examination, a visible and palpable, immobile hard bump on the superolateral aspect of the patella was present (Fig. 1).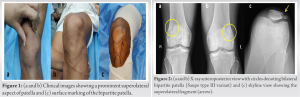 It was tender to touch, and terminal extension was restricted due to pain. Radiographs of the bilateral knee revealed a bipartite patella, Saupe type three variant (Superolateral) [2]. Further, magnetic resonance imaging was done to rule out associated meniscligamentous pathologies (Fig. 2 and 3).
It was tender to touch, and terminal extension was restricted due to pain. Radiographs of the bilateral knee revealed a bipartite patella, Saupe type three variant (Superolateral) [2]. Further, magnetic resonance imaging was done to rule out associated meniscligamentous pathologies (Fig. 2 and 3).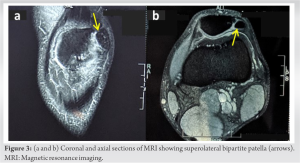
Treatment
Non-operative
In season, the player had significant symptoms for 6 months. The anterior knee pain was more predominant following the training sessions and matches significantly limiting performance and field time. He was conservatively managed with oral analgesics, Kinesio offloading taping, bracing, interferential therapy, cryocompression, and intermittent immobilization with a mild reduction in symptoms during the early presentation.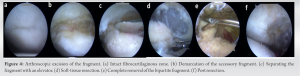
Operative
Arthroscopic surgery was advised during the off-season. Arthroscopic superolateral bipartite patella excision with ablation chondroplasty was done. Three portals anteromedial, anterolateral, and superolateral were used. The findings were firm attachment of bipartite patella with chondromalacia – II changes in the superomedial and inferolateral aspect of the articular surface. The arthroscopic steps and findings are shown in Fig. 4. The excised fragment along with fibrocartilaginous tissue measured 4 × 2 cm (Fig. 5). The athlete’s post-operative course was uneventful.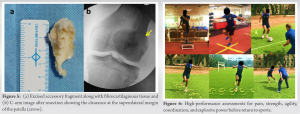
Rehabilitation
Postoperatively, an accelerated rehabilitation protocol was tailored for the athlete.
- Phase 1 (Week 1): Cryotherapy, patellar mobilization, quadriceps strengthening, straight leg raises, range of motion, and weight-bearing as tolerated
- Phase 2 (Week 2): Isometric cocontraction exercises, Hamstring and quadriceps stretches, active-assisted range of motion exercises, resistance band, and Thera-tube exercises to improve terminal extension
- Phase 3 (Week 3–4): Straight leg raises in all planes with weights, Aqua therapy inclusive of pool walking, step-ups and stretches, core strengthening, balance, and proprioceptive exercises
- Phase 4 (Week 5): Progression of open and closed kinetic chain exercises depending on the pain intensity.
Return to sports
After strict adherence to phased rehabilitation, the footballer was escalated to a high-performance strength training during the last phase of rehabilitation. Exercises were focused to improve his core strength, agility, explosive power, and aerobic capacity. Resistance training resorted to the last phase of the strength and conditioning program. A return to sports assessment both indoors and on-field was performed by a bio kineticist supervised by a sports physician. Box jumps, hurdle hops, quadrant pattern hops, football drills, tackling, change of direction speed, and agility were tested at varying intensities (Fig. 6). The player was cleared to return to sports 6 week after the arthroscopic procedure and was followed up for 1 year.
Erich Saupe classified bipartite patella into three types: Type I involving the inferior pole (5%), type II the lateral margin (20%), and type III the superolateral quadrant (75%) of the patella of which type III is more common [2]. An unresolved painful bipartite patella is a rare condition. All the conservative modalities recommended in the literature were tried in our case except for local injections. Continued conservative treatment returned only around 38% of the athletes to play without symptoms according to a systematic review by Matic and Flanigan [3]. When incapacitating pain persists despite non-operative treatment, surgical excision is preferred. The surgical options are open excision of fragment [4], arthroscopic excision of fragment [5], tension band wiring, open reduction, and internal fixation [6,7], open or arthroscopic vastus lateralis release, and lateral retinacular release [8]. Arthroscopic management of painful bipartite patella is a safe and effective alternative to open surgical excision or release [9]. Distinctive advantages of arthroscopic intervention are minimal access, no damage to the extensor mechanism, assessing the knee for concurrent pathology, extensile denervation for pain relief, quick recovery, and early return to sport. Studies have shown, excision of the accessory fragment resulted in 100% success in returning patients to prior activities, with 91% returning to their respective sports without symptoms and 9% returning with residual symptoms [3,10]. Being an elite player, we offered arthroscopic surgery to our patient. He re-joined the team within a span of 6 weeks. Surgical complications such as anterior knee pain, quadriceps weakness, and extensor lag were anticipated and avoided in our patient by a focused rehabilitation program as explained above. The footballer was followed up for 1 year for the recurrence of symptoms. The athlete had no complaints of knee pain or knee-related injury and performed well with the team. The largest series on the bipartite patella is from Finland, where Weckström et al. [4] Followed 32 military recruits who were treated with fragment excision (28 open and four arthroscopic) for 10 years. Out of 25 subjects available for 10 years follow-up, three patients had knee pain, two chondromalacia patella, and one early osteoarthritis, all treated conservatively. Excision of the painful fragment should come sooner in the surgeon’s treatment algorithm for athletes who fail conservative options initially [3].
Arthroscopic excision of the bipartite patella allowed the player to do accelerated rehabilitation and aid in an early return to play. This case report also signifies the need for tailored rehabilitation and sports-specific assessments before returning to the field to achieve optimal performance which is often neglected while treating sports persons.
Anterior knee pain in an athlete, in the absence of injury, should raise suspicion of the bipartite patella. When non-operative management fails, arthroscopic excision of a painful bipartite patellar fragment should be the surgeon’s first choice keeping in view the following advantages: Less invasive technique than open surgeries allows for the early and aggressive post-operative rehabilitation; expedited return to competition; and results in a good functional long-term outcome.
References
- 1.Kavanagh EC, Zoga A, Omar I, Ford S, Schweitzer M, Eustace S. MRI findings in the bipartite patella. Skeletal Radiol 2007;36:209-14. [Google Scholar | PubMed]
- 2.Saupe H. PrimÄre knochenmarkseiterung der kniescheibe. Dtsch Z Chir 1943;258:386-92 . [Google Scholar | PubMed]
- 3.Matic GT, Flanigan DC. Return to activity among athletes with a symptomatic bipartite patella: A systematic review. Knee 2015;22:280-5. [Google Scholar | PubMed]
- 4.Weckström M, Parviainen M, Pihlajamäki HK. Excision of painful bipartite patella: Good long-term outcome in young adults. Clin Orthop Relat Res 2008;466:2848-55. [Google Scholar | PubMed]
- 5.Azarbod P, Agar G, Patel V. Arthroscopic excision of a painful bipartite patella fragment. Arthroscopy 2005;21:1006. [Google Scholar | PubMed]
- 6.Tauber M, Matis N, Resch H. Traumatic separation of an uncommon bipartite patella type: A case report. Knee Surg Sports Traumatol Arthrosc 2007;15:83-7. [Google Scholar | PubMed]
- 7.Vaishya R, Chopra S, Vijay V, Vaish A. Bipartite patella causing knee pain in young adults: A report of 5 cases. J Orthop Surg (Hong Kong) 2015;23:127-30. [Google Scholar | PubMed]
- 8.Felli L, Formica M, Lovisolo S, Capello AG, Alessio-Mazzola M. Clinical outcome of arthroscopic lateral retinacular release for symptomatic bipartite patella in athletes. Arthroscopy 2018;34:1550-8. [Google Scholar | PubMed]
- 9.Loewen A, Ge SM, Marwan Y, Burman M, Martineau PA. Arthroscopic management for bipartite patella: A systematic review. Orthop J Sports Med 2021;9:23259671211022248. [Google Scholar | PubMed]
- 10.Pan T, Hennrikus WL. Outcomes of surgical treatment of symptomatic bipartite patella in teenage athletes. J Pediatr Orthop B 2022;31:371-5. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 Unusual Case of Lateral Knee Pain: Magnetic Resonance Imaging Evidence of Isolated Lateral Patellotibial Ligament Enthesopathy
December 1, 2025 Unusual Case of Lateral Knee Pain: Magnetic Resonance Imaging Evidence of Isolated Lateral Patellotibial Ligament Enthesopathy July 10, 2024 Return to Sports in Stress Reaction and Stress Fractures in Indian Athletes: A Case Series
July 10, 2024 Return to Sports in Stress Reaction and Stress Fractures in Indian Athletes: A Case Series November 10, 2023 Patellofemoral Arthroplasty for Irreducible Chronic Bilateral Patella Dislocation-A Case Report
November 10, 2023 Patellofemoral Arthroplasty for Irreducible Chronic Bilateral Patella Dislocation-A Case Report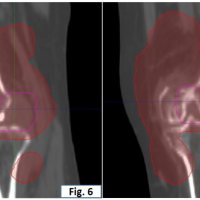 August 10, 2023 A Rare Case of Anaplastic Large Cell Lymphoma of the Knee Joint
August 10, 2023 A Rare Case of Anaplastic Large Cell Lymphoma of the Knee Joint