
A differential of nodular fasciitis presenting as fibroma even though uncommon should always be kept as a differential in a case of a popliteal baker’s syst.
Dr Aashay Sonkusale, Department of Orthopaedics, Indira Gandhi Government Medical College and Hospital, Nagpur, Maharashtra, India. E-mail: Aashay49@gmail.com
Abstract
Introduction: This is a case of a popliteal swelling which was clinically misdiagnosed as a simple popliteal cyst, which turned out to be a benign fibroblastic tumor featuring nodular fasciitis (NF). A swelling in the popliteal fossa by and large is considered to be a Baker’s cyst. However, an array of other lesions which can be encountered such as fibroma featuring NF, meniscal cysts, lipoma, aneurysms, bursitis of the biceps femoris tendon, and schwannoma should also be borne in mind since clinical and radiological evaluation may not always be conclusive. This case report presents fibroma featuring NF masquerading as Baker’s cyst, which has not been described in any literature that the authors could find hitherto, making it a unique case.
Case Report: A 20-year-old male man presented to the outpatient department with a solitary palpable mass on the posterior aspect of his right knee for the past 3 years associated with difficulty in squatting for the past 3 months. The mass gradually was well defined and increased gradually in size to the current size of 10*9 cm, irregular soft to firm in consistency, spherical, non-tender, and non-reducible on the posterior aspect of the popliteal fossa. Local ultrasonography showed evidence of heterogeneous hypoechoic lesion with signs of inflammation; underlying bony cortices appeared to be normal. A clinical diagnosis of Baker’s cyst was made and an excisional biopsy was performed. Microscopically, histologic sections showed fibroblasts arranged in loose fascicular patterns intermixed with small amount of collagen and myxoid stroma.
Conclusion: Popliteal masses need not always be simple Baker’s cyst, and careful evaluation of the mass in the popliteal fossa is always mandatory. Radiologic investigations may not always be conclusive and biopsy is the gold standard for diagnosis.
Keywords: Popliteal cyst, nodular fasciitis, benign, excisional biopsy.
Baker’s cyst is the most common mass encountered around the popliteal fossa. These are benign enlargements of the gastrocnemius-semimembranosus bursa that lies between the two muscles and are usually treated conservatively with identification of the underlying conditions [1]. However, one should also have a high index of suspicion of other pathologies of the popliteal fossa since a number of other differentials are also present, namely, fibroma featuring nodular fasciitis (NF), meniscal cysts, popliteal aneurysm, bursitis of the biceps femoris tendon, schwannoma, and ganglion [1,2]. NF is a benign reactive, self-limiting soft-tissue lesion, frequently found in the subcutaneous tissues and muscle fascia, which shows proliferation of myofibroblasts and fibroblasts. NF was first described by Konwaler et al. as a subcutaneous pseudosarcomatous fibromatosis and has subsequently been named infiltration fasciitis and pseudosarcomatous fasciitis [3,4,5]. NF has been frequently reported at many anatomic sites, namely, the upper extremities (12%) [6,7], the trunk (15–18%), the head and neck (7–20%) [8], and finally, the lower extremities [8,9]. We present a case of soft-tissue swelling of the popliteal fossa, which turned out to be benign fibroma featuring NF. This clinical entity is rare and unheard of, which makes this case report an intriguing and exceptional one.
A 20-year-old man presented to the outpatient department with a palpable mass in the posterior aspect of his knee for the past 3 years. The mass was painless, gradual in onset, and slowly progressed to a size of 10*9 cm when he presented to the outpatient department. The patient had difficulty in squatting for the last 3 months. On local examination, the mass was non-tender, had soft-to-firm consistency, well-defined edges, was smooth, and non-movable with no visible or palpable pulsations. The mass was non-reducible and was not fixed to the overlying skin. Overlying skin showed no signs of local inflammation. Knee flexion was slightly decreased due to the mass effect of swelling with associated discomfort. Distal pulsations were symmetric with no neural deficit. Lateral plain radiography of the right knee showed a diffuse, non-specific soft-tissue density, with no evidence of calcifications or connection to the underlying bone. Local ultrasonography revealed a heterogeneously hypoechoic lesion of size 9.6*8.6 cm in the right popliteal fossa increased with internal vascularity and signs of inflammation. No associated knee effusion was noted. Due to financial constraints, magnetic resonance imaging (MRI) could not be performed. The patient was counseled about the importance of obtaining an MRI; informed consent was taken to proceed with an excisional biopsy. An excisional biopsy was performed using a posterior approach. The mass was located between the two heads of gastrocnemius, under the superficial fascia (Fig. 1). 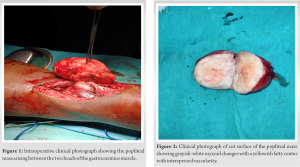 It was encapsulated with no major adhesions, and separation from the surrounding soft tissue was relatively easy using blunt dissection considering the proximity of the mass to nearby neurovascular structures. A solid and brownish-red mass was excised and sent to a pathologist for further histopathological examination. The mass was well circumscribed and the cut surface showed gray-white myxoid change with a yellowish fatty center with interspersed vascularity (Fig. 2). On histopathology, spindle-shaped fibroblasts arranged in fascicular pattern showing “a tissue culture appearance.” Cells were slender, and elongated with oval nuclei and prominent nucleoli. Intervening collagenous stroma shows myxoid changes with a few blood vessels and focal inflammation (Fig. 3).
It was encapsulated with no major adhesions, and separation from the surrounding soft tissue was relatively easy using blunt dissection considering the proximity of the mass to nearby neurovascular structures. A solid and brownish-red mass was excised and sent to a pathologist for further histopathological examination. The mass was well circumscribed and the cut surface showed gray-white myxoid change with a yellowish fatty center with interspersed vascularity (Fig. 2). On histopathology, spindle-shaped fibroblasts arranged in fascicular pattern showing “a tissue culture appearance.” Cells were slender, and elongated with oval nuclei and prominent nucleoli. Intervening collagenous stroma shows myxoid changes with a few blood vessels and focal inflammation (Fig. 3). 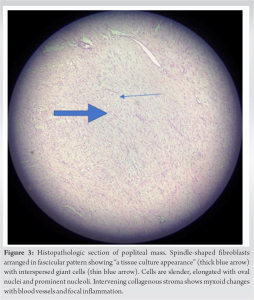 There were no neurological or vascular complications post-operatively. Three months post-operatively, the patient showed clinical improvement in symptoms and could squat without discomfort.
There were no neurological or vascular complications post-operatively. Three months post-operatively, the patient showed clinical improvement in symptoms and could squat without discomfort.
Popliteal cyst, synonymous with Baker’s cyst is the most common differential of a popliteal swelling with a prevalence rate of 5–19% on a series of MRI studies [10,11]. The high prevalence of Baker’s cyst along with its typical location and characteristics makes it almost a clinical decision to diagnose it-ultrasonography and aspiration of the cyst being the routine evaluation steps. However, one should also have a high index of suspicion for other pathologies of the popliteal fossa since a number of other lesions are also possible, namely, fibroma featuring NF, lipoma, popliteal aneurysm, bursitis of the biceps femoris tendon, schwannoma, and ganglion [1,2]. Rare differentials include osteochondrolipoma, localized hypertrophy of the semimembranosus muscle, aggressive fibromatosis, neurofibroma, and synovial sarcoma to name a few, should also be kept at the back of the mind while evaluating swelling in the back of the knee. Popliteal mass accompanied by erythema, pedal edema, and pulsations points toward an aneurysm. Schwannomas usually present with numbness or parasthesia of the limb with a positive Tinel’s sign. Lipomas are soft, non-fluctuant, and painless unless causing mass effect on neurovascular structures. A swelling which moves on movement of the knee and disappears on knee flexion can point toward a localized hypertrophy of the semimembranosus muscle. In any case, an atypical finding on physical examination warrants further investigation in the form of local ultrasonography and MRI. Ultrasonography is a cheap and useful imaging modality to differentiate between cystic and solid swelling but may not always be sufficient or precise. Tatari et al. [12] reported a well-circumscribed mass, resembling Baker’s cyst using USG, finally confirmed the diagnosing of the lesion to be pigmented villonodular synovitis. This emphasizes on the need for biopsy, which remains the gold standard for diagnosing any soft-tissue mass. In this case, the slow and gradual progression of the lesion with soft-to-firm consistency and the absence of neurovascular and constitutional symptoms pointed toward a benign entity. Furthermore, due to financial restraints, our patient could not undergo MRI. We decided to go for an open excisional biopsy for confirmation of our lesion, which was the next best course of action since it would include both diagnostic and therapeutic modes of management. Histopathologic picture of spindle-shaped fibroblasts arranged in fascicular pattern showing “a tissue culture appearance” with intervening collagenous stroma with myxoid changes with signs of focal inflammation; cells had oval nucleus with prominent nucleoli. A diagnosis of benign fibroma featuring NF was made. NF is most commonly seen in young adults between the ages of 20 and 40 years [6,7]. In this case report, the lesion was seen in a 20-year-old male fitting well in the literature-described age group. Histologically, NF is classified into three subtypes, on the basis of the plane of tissue involved: subcutaneous, intramuscular, and fascial [13]. In this case, the mass was seen to be between the epimysial planes of the two heads of gastrocnemius, attached to the surrounding subcutaneous fat, and relatively superficial. As described above, the popliteal mass that was initially misdiagnosed as simple popliteal cyst, finally turned out to be fibroblastic benign tumor featuring NF. Local excision is usually an effective treatment for most lesions with recurrences rates of 1–2% reported.
Popliteal masses as not necessarily always popliteal cysts and a thorough examination aided by necessary investigations in case of any doubt or dilemma should be performed without hesitation. All popliteal swellings should always be evaluated with a reasonably high index of suspicion.
A differential of NF presenting as fibroma should always be kept in mind while evaluating a case of popliteal swelling.
References
- 1.Baker WM. On the formation of synovial cysts in the leg in connection with disease of the knee-joint. 1877. Clin Orthop Relat Res 1994;299:2-10. [Google Scholar | PubMed]
- 2.Fritschy D, Fasel J, Imbert JC, Bianchi S, Verdonk R, Wirth CJ. The popliteal cyst. Knee Surg Sports Traumatol Arthrosc 2006;14:623-8. [Google Scholar | PubMed]
- 3.Konwaler BE, Keasbey L, Kaplan L. Subcutaneous pseudosarcomatous fibromatosis (fasciitis). Am J Clin Pathol 1955;25:241-52. [Google Scholar | PubMed]
- 4.Hutter RV, Stewart FW, Foote FW Jr. Fasciitis. A report of 70 cases with follow-up proving the benignity of the lesion. Cancer 1962;15:992-1003. [Google Scholar | PubMed]
- 5.Martínez-Blanco M, Bagán JV, Alba JR, Basterra J. Maxillofacial nodular fasciitis: A report of 3 cases. J Oral Maxillofac Surg 2002;60:1211-4. [Google Scholar | PubMed]
- 6.Khanna V, Rajan M, Reddy T, Alexander N, Surendran P. Nodular fasciitis mimicking a soft tissue sarcoma – A case report. Int J Surg Case Rep 2018;44:29-32. [Google Scholar | PubMed]
- 7.Katz MA, Beredjiklian PK, Wirganowicz PZ. Nodular fasciitis of the hand: A case report. Clin Orthop Relat Res 2001;382:108-11. [Google Scholar | PubMed]
- 8.Jang EJ, Park TI, Nam SC, Park JY. Nodular fasciitis in the submandibular gland. Diagn Cytopathol 2008;36:805-8. [Google Scholar | PubMed]
- 9.Dayan D, Nasrallah V, Vered M. Clinico-pathologic correlations of myofibroblastic tumors of the oral cavity: 1. Nodular fasciitis. J Oral Pathol Med 2005;34:426-35. [Google Scholar | PubMed]
- 10.Miller TT, Staron RB, Koenigsberg T, Levin TL, Feldman F. MR imaging of baker cysts: Association with internal derangement, effusion, and degenerative arthropathy. Radiology 1996;201:247-50. [Google Scholar | PubMed]
- 11.Sansone V, De Ponti A. Arthroscopic treatment of popliteal cyst and associated intra-articular knee disorders in adults. Arthroscopy 1999;15:368-72. [Google Scholar | PubMed]
- 12.Tatari H, Baran O, Lebe B, Kiliç S, Manisali M, Havitçioglu H. Pigmented villonodular synovitis of the knee presenting as a popliteal cyst. Arthroscopy 2000;16:13. [Google Scholar | PubMed]
- 13.Al-Hayder S, Warnecke M, Hesselfeldt-Nielsen J. Nodular fasciitis of the face: A case report. Int J Surg Case Rep 2019;61:207-9. [Google Scholar | PubMed]
- 14.Fiori R, Chiappa R, Gaspari E, Simonetti G. A rare case of popliteal venous aneurysm. Case Rep Med 2010;2010:579256. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2025 Melorheostosis: A Rare Case Report with Pelvic and Lumbar Involvement
August 1, 2025 Melorheostosis: A Rare Case Report with Pelvic and Lumbar Involvement November 1, 2024 An Unusual Giant Osteochondroma of Distal Tibia: A Case Report with Literature Review
November 1, 2024 An Unusual Giant Osteochondroma of Distal Tibia: A Case Report with Literature Review October 1, 2024 Atypical Location of Enchondroma and its Management – A Case Report
October 1, 2024 Atypical Location of Enchondroma and its Management – A Case Report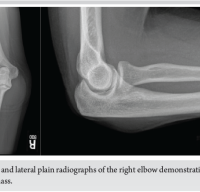 July 10, 2024 Intramuscular Myxoma of the Flexor Carpi Ulnaris Causing Cubital Tunnel Syndrome: A Case Report
July 10, 2024 Intramuscular Myxoma of the Flexor Carpi Ulnaris Causing Cubital Tunnel Syndrome: A Case Report