
Remote Cerebellar Hemorrhage can also occur in spinal surgery without dural injury, especially in patients with a history of intracranial lesions.
Dr. Shinsuke Sato, Department of Orthopedic Surgery, Ibaraki Prefectural Central Hospital, Kasama Shi, Ibaraki Ken, 309 1703, Japan. E-mail: shinsuke.0918@gmail.com
Abstract
Introduction: Remote cerebellar hemorrhage (RCH) has been reported as a serious complication of spine surgery and is considered to be caused by dural injury. However, we have experienced a case in which intracranial hemorrhage occurred immediately after lumbar spine surgery without dural tear. There were no reports of RCH in spinal surgery without dural injury as far as we could find.
Case Report: We described a rare presentation of an 80-year-old male who suffered a loss of consciousness after lumbar surgery. He was diagnosed with impaired consciousness due to chronic and acute intracranial hemorrhage. He went through two hematoma removal surgeries and his consciousness improved.
Conclusion: RCH can occur in spinal surgery in patients with predicted cerebrovascular fragility, even in the absence of dural injury. Pre-operative imaging evaluation could be useful in assessing cerebrovascular fragility.
Keywords: Remote cerebellar hemorrhage, dural injury, spine surgery.
Dural injury is an avoidable complication of spine surgery. A serious sequela associated with dural injury is remote cerebellar hemorrhage (RCH), which causes intracranial hemorrhage. Although there are reports of RCH due to intended or unintended dural tears [1,2], such as from surgery for intradural tumors, we found no reports of RCH after spinal surgery in which dural injury was absent. In this report, we describe a rare case of a patient who developed a consciousness disorder immediately after lumbar spine surgery. Even though there was no apparent dural injury, an intracranial hematoma was found. Further, we discuss the reasons for the intracranial hematoma.
An 80-year-old man came to our hospital with chief complaints of low back pain and leg pain. He had no muscle weakness in his lower extremities. He was diagnosed with lumbar spinal canal stenosis after various examinations including magnetic resonance imaging (MRI) (Fig. 1). 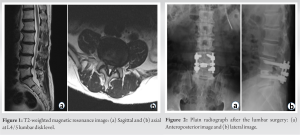 One month after the initial visit, he was admitted for an examination and underwent myelography and root block. As the pain improvement was temporary, the patient requested surgery for the improvement of symptoms. He had a history of a right capsular hemorrhage treated conservatively 9 years earlier; however, there were no sequelae. There was no subsequent episode of falls. In addition, there was no history of heavy alcohol consumption. Before lumbar spine surgery, the patient was in a normal state of consciousness and was able to communicate normally. Lumbar posterior slow pressure fusion (L4/5 transforaminal lumbar interbody fusion) was performed 2.5 months after the initial diagnosis (Fig. 2). The procedure was performed under general anesthesia in a prone position with an anesthesia time of 4 h 18 min and an operation time lasting 2 h 50 min. The associated blood loss was 34 mL and the operation was completed without complications such as an intraoperative dural tear. There were no significant changes in vital signs perioperatively. After surgery, he was unable to move his limbs according to the instructions, although he was able to open his eyes due to pain stimulation. However, there were no abnormalities in his respiration or vital signs, and he was extubated. He was considered to be poorly awake due to anesthesia, and he was shifted to the ward. However, several hours post-surgery, his state of consciousness did not improve from the very low Glasgow coma scale (GCS) (E4V1M1). Computed tomography (CT) scan of the head taken to identify the cause of prolonged loss of consciousness showed a chronic subdural hematoma with some fresh hemorrhage (Fig. 3a).
One month after the initial visit, he was admitted for an examination and underwent myelography and root block. As the pain improvement was temporary, the patient requested surgery for the improvement of symptoms. He had a history of a right capsular hemorrhage treated conservatively 9 years earlier; however, there were no sequelae. There was no subsequent episode of falls. In addition, there was no history of heavy alcohol consumption. Before lumbar spine surgery, the patient was in a normal state of consciousness and was able to communicate normally. Lumbar posterior slow pressure fusion (L4/5 transforaminal lumbar interbody fusion) was performed 2.5 months after the initial diagnosis (Fig. 2). The procedure was performed under general anesthesia in a prone position with an anesthesia time of 4 h 18 min and an operation time lasting 2 h 50 min. The associated blood loss was 34 mL and the operation was completed without complications such as an intraoperative dural tear. There were no significant changes in vital signs perioperatively. After surgery, he was unable to move his limbs according to the instructions, although he was able to open his eyes due to pain stimulation. However, there were no abnormalities in his respiration or vital signs, and he was extubated. He was considered to be poorly awake due to anesthesia, and he was shifted to the ward. However, several hours post-surgery, his state of consciousness did not improve from the very low Glasgow coma scale (GCS) (E4V1M1). Computed tomography (CT) scan of the head taken to identify the cause of prolonged loss of consciousness showed a chronic subdural hematoma with some fresh hemorrhage (Fig. 3a).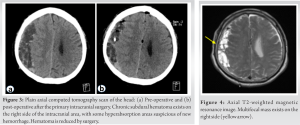 The patient developed generalized tonic chronic convulsions and anticonvulsant drugs were administered and the seizures stopped. The patient consulted a neurosurgeon and underwent emergency perforator drainage under local anesthesia on the same day. The drained blood also contained fresh hemorrhage (Fig. 3b). The day after surgery, he was still unconscious with GCS 6 (E4V1M1), therefore, head MRI and an electroencephalogram (EEG) were performed. MRI showed a small hemorrhage on the surface of the brain, but there was no evidence of a cerebral aneurysm or cerebral infarction (Fig. 4). The EEG revealed that he was in a state of epileptic agglutination, which was the likely cause of unconsciousness. No cerebrospinal fluid (CSF) drainage was observed from the lumbar spine surgical drain; hence, it was removed 2-day postoperatively. Despite the adjustment of anticonvulsant medications, the patient continued to suffer from prolonged loss of consciousness. A multifocal subdural hematoma that could not be removed during initial surgery was considered the cause of prolonged epileptic convulsions. A craniotomy was performed 14 days after the initial surgery to remove the hematoma (Fig. 5a). The day after the craniotomy, he was able to speak. His consciousness gradually improved, and 3 months after the surgery, his speech improved. In addition, he was able to walk on parallel bars and was transferred to a rehabilitation hospital (Fig. 5b).
The patient developed generalized tonic chronic convulsions and anticonvulsant drugs were administered and the seizures stopped. The patient consulted a neurosurgeon and underwent emergency perforator drainage under local anesthesia on the same day. The drained blood also contained fresh hemorrhage (Fig. 3b). The day after surgery, he was still unconscious with GCS 6 (E4V1M1), therefore, head MRI and an electroencephalogram (EEG) were performed. MRI showed a small hemorrhage on the surface of the brain, but there was no evidence of a cerebral aneurysm or cerebral infarction (Fig. 4). The EEG revealed that he was in a state of epileptic agglutination, which was the likely cause of unconsciousness. No cerebrospinal fluid (CSF) drainage was observed from the lumbar spine surgical drain; hence, it was removed 2-day postoperatively. Despite the adjustment of anticonvulsant medications, the patient continued to suffer from prolonged loss of consciousness. A multifocal subdural hematoma that could not be removed during initial surgery was considered the cause of prolonged epileptic convulsions. A craniotomy was performed 14 days after the initial surgery to remove the hematoma (Fig. 5a). The day after the craniotomy, he was able to speak. His consciousness gradually improved, and 3 months after the surgery, his speech improved. In addition, he was able to walk on parallel bars and was transferred to a rehabilitation hospital (Fig. 5b).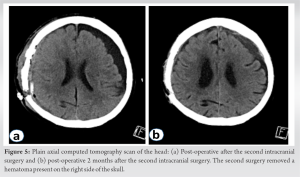
A typical complication of spine surgery is intraoperative dural injury. Leakage of CSF due to dural injury may lead to the appearance of hypomyelination syndrome, wound infection, respiratory complications, ileus, deep vein thrombosis, meningitis, epidural hematoma, prolonged hospital stay, and rehospitalization [3,4,5,6,7,8]. In addition, a serious complication resulting from a dural injury is RCH [1,2]. It has been reported that the cause of RCH is the flexion and occlusion of subdural veins due to downward traction of the brain caused by leakage of spinal fluid. This may be attributed to dural injury, and vascular disruption caused by an increased difference in pressure gradient between intracranial vessels and intrathecal pressure [9,10,11]. Even though, there was no intraoperative dural injury and no obvious post-operative CSF leakage, we discuss the reasons for the intracranial hemorrhage in our case. We believe that intracranial vascular fragility was the cause of acute subdural hematoma. The fragility of the blood vessels is suggested by the chronic subdural hematoma that occurred despite the absence of major trauma, and by the history of the conservative treatment of capsular hemorrhage. The fluctuating difference between intracranial vascular pressure and intrathecal pressure in the vulnerable vessels was the direct cause of the acute subdural hematoma. It is believed to be a combination of both intrathecal pressure changes due to spinal decompression surgery [12] and intracranial intravascular pressure changes caused by blood pressure fluctuations during intubation, intraoperative, and extubation. Surve et al. have shown that blood pressure fluctuation is greater under general anesthesia than under local anesthesia in surgery for chronic subdural hematoma [13]. Another possible cause of subdural hemorrhage is CSF leakage due to an undetected dural tear. However, the absence of CSF leakage from the post-operative drain and the lack of obvious fluid retention in the surgical site on the post-operative lumbar CT scan suggest that this was not the cause. In addition, the coagulation system was examined for the cause, and no abnormality was found in the blood sample.
This case report describes a post-operative intracranial hemorrhage resulting in impaired consciousness in a spinal surgery without dural injury. The fragility of intracranial blood vessels can cause new intracranial hemorrhage even under the influence of decompression surgery or general anesthesia. In this case, no pre-operative findings suggested intracranial disease; therefore, the presence of a chronic subdural hematoma could not be suspected beforehand. However, in the future, imaging studies such as a head CT scan may be required before spinal surgery if there is a history of intracranial hemorrhage or if an intracranial lesion is suspected on pre-operative assessment. Depending on the results, neurosurgical consultation and intervention may be required.
RCH is a rare but serious complication in spine surgery. RCH can occur even in surgeries without dural injury and pre-operative CT imaging of the head is useful in assessing intracranial vascular fragility.
References
- 1.Worm PV, Dalla-Corte A, Brasil AV, Perondi G, Sfreddo E, Vial AD, et al. Cerebellar hemorrhage as a complication of spine surgery. Surg Neurol Int 2019;10:85. [Google Scholar | PubMed]
- 2.Lim CH, Salkade PR, Peter AC. Remote cerebellar hemorrhage as a complication of lumbar spine surgery. J Radiol Case Rep 2020;14:1-11. [Google Scholar | PubMed]
- 3.Alluri R, Kang HP, Bouz G, Wang J, Hah RJ. The true effect of a lumbar dural tear on complications and cost. Spine (Phila Pa 1976) 2020;45:E155-62. [Google Scholar | PubMed]
- 4.Yoshihara H, Yoneoka D. Incidental dural tear in lumbar spinal decompression and discectomy: Analysis of a nationwide database. Arch Orthop Trauma Surg 2013;133:1501-8. [Google Scholar | PubMed]
- 5.Strömqvist F, Jönsson B, Strömqvist B, Swedish Society of Spinal Surgeons. Dural lesions in lumbar disc herniation surgery: Incidence, risk factors, and outcome. Eur Spine J 2010;19:439-42. [Google Scholar | PubMed]
- 6.Takenaka S, Makino T, Sakai Y, Kashii M, Iwasaki M, Yoshikawa H, et al. Dural tear is associated with an increased rate of other perioperative complications in primary lumbar spine surgery for degenerative diseases. Medicine (Baltimore) 2019;98:e13970. [Google Scholar | PubMed]
- 7.Khan MH, Rihn J, Steele G, Davis R, Donaldson WF 3rd, Kang JD, et al. Postoperative management protocol for incidental dural tears during degenerative lumbar spine surgery: A review of 3,183 consecutive degenerative lumbar cases. Spine (Phila Pa 1976) 2006;31:2609-13. [Google Scholar | PubMed]
- 8.Ghobrial GM, Theofanis T, Darden BV, Arnold P, Fehlings MG, Harrop JS. Unintended durotomy in lumbar degenerative spinal surgery: A 10-year systematic review of the literature. Neurosurg Focus 2015;39:E8. [Google Scholar | PubMed]
- 9.Thomas G, Jayaram H, Cudlip S, Powell M. Supratentorial and infratentorial intraparenchymal hemorrhage secondary to intracranial CSF hypotension following spinal surgery. Spine (Phila Pa 1976) 2002;27:E410-2. [Google Scholar | PubMed]
- 10.Konya D, Ozgen S, Pamir MN. Cerebellar hemorrhage after spinal surgery: Case report and review of the literature. Eur Spine J 2006;15:95-9. [Google Scholar | PubMed]
- 11.Lu CH, Ho ST, Kong SS, Cherng CH, Wong CS. Intracranial subdural hematoma after unintended durotomy during spine surgery. Can J Anaesth 2002;49:100-2. [Google Scholar | PubMed]
- 12.Kwon BK, Curt A, Belanger LM, Bernardo A, Chan D, Markez JA, et al. Intrathecal pressure monitoring and cerebrospinal fluid drainage in acute spinal cord injury: A prospective randomized trial. J Neurosurg Spine 2009;10:181-93. [Google Scholar | PubMed]
- 13.Surve RM, Bansal S, Reddy M, Philip M. Use of dexmedetomidine along with local infiltration versus general anesthesia for burr hole and evacuation of chronic subdural hematoma (CSDH). J Neurosurg Anesthesiol 2017;29:274-80. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 10, 2020 Trochanteric Advancement and Limb Lengthening by Monorail External Fixator in Sequelae of the Septic Hip in Children – A Simpler Alternative to Other Complex Procedures
August 10, 2020 Trochanteric Advancement and Limb Lengthening by Monorail External Fixator in Sequelae of the Septic Hip in Children – A Simpler Alternative to Other Complex Procedures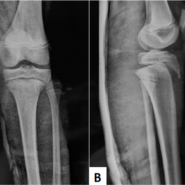 July 10, 2021 Salter-Harris I Injury of the Proximal Tibial Physis with Vascular Compromise: A Case Report and Review of Literature
July 10, 2021 Salter-Harris I Injury of the Proximal Tibial Physis with Vascular Compromise: A Case Report and Review of Literature June 1, 2026 Two-Stage Reconstruction for Failed Subtrochanteric Femur Fixation with Peri-Implant Infection and Severe Proximal Femoral Bone Loss: A Case Report
June 1, 2026 Two-Stage Reconstruction for Failed Subtrochanteric Femur Fixation with Peri-Implant Infection and Severe Proximal Femoral Bone Loss: A Case Report January 10, 2021 Dry Arthroscopy” is a Valuable Tool in the Excisional Curettage of Chondroblastoma: A Case Series
January 10, 2021 Dry Arthroscopy” is a Valuable Tool in the Excisional Curettage of Chondroblastoma: A Case Series