
In cases with proximal fibular osteochondroma, care should be taken to identify the entire nerve before removal of osteochondroma as failure to identify the anatomy of the nerve by the unwary surgeon may result in neurologic injury.
Dr. Pranav Gupta, Department of Orthopaedics, Guru Gobind Singh Medical College and Hospital, Faridkot, Punjab, India. E-mail: pranavchd88@gmail.com
Abstract
Introduction: Osteochondroma is the most common benign tumor of bone. Tumors are metaphyseal in origin and commonly involve distal femur, proximal tibia, and proximal fibula in the lower extremity. Osteochondroma located at proximal fibula can change the normal path of nerves and it may lead to the compression of vessels or peroneal nerve, leading to paralysis.
Case Report: We are reporting a case of an 18-year-old female with proximal fibular osteochondroma causing splitting of common peroneal nerve without any neuropathy.
Conclusion: We strive to make the surgeons aware that, when removing osteochondroma located at proximal fibula, care should be taken to identify the entire nerve at the site of lesion before the removal as a procedure done in a hurry in such a case can cause irreversible damage to the patient.
Keywords: Cartilage cap, peroneal nerve, osteochondroma.
Osteochondroma is the most common benign tumor of bone [1]. Tumors are metaphyseal in origin and commonly involve distal femur, proximal tibia, and proximal fibula in lower extremity [1]. Osteochondromas increase in size throughout the growth period but stop when the epiphyseal plates close [2]. Osteochondroma of proximal fibula is very close to the neurovascular bundle which can lead to compressive neuropathy of peroneal nerve [2]. It is usually a painless mass without associated symptoms. Symptoms when present may be due to impingement of contiguous tendons, major blood vessels or nerves, contusions, or fractures in rare instances. Osteochondroma located at proximal fibula can change the normal path of nerves and it may lead to the compression of vessels or peroneal nerve, leading to paralysis [3]. Here, we are describing a rare case of proximal fibular osteochondroma in an 18–year- old female, in which osteochondroma is growing through the midsubstance of common peroneal nerve without causing any neurological deficit.
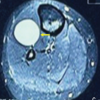
An 18-year-old female presented with pain and swelling over anterolateral aspect of the right proximal leg. Initially, it was small and painless, but gradually, over a period of 3 years, it increased in size and started causing pain. Pain was dull aching in nature, which was aggravated on movement and relieved on rest. There was no history of trauma or fever. On examination, we noted a sizeable swelling of size approximately 6 × 4 × 3 cm on proximal one-third right leg over its anterolateral aspect. The swelling was irregular, bony hard in consistency, and fixed to the underlying bone. Tenderness was absent. Knee range of motion (ROM) was comparable to the normal side, and neurovascular function was intact. X-ray and magnetic resonance imaging (MRI) were done as a part of pre-operative evaluation which revealed an eccentric large cauliflower-like growth arising from proximal fibula (Fig. 1). Indication for surgery was painful ROM around knee joint. After a thorough assessment, the patient was planned for en bloc excision of osteochondroma. In supine position, a longitudinal incision was made along the posterior border of fibula. Common peroneal nerve was explored and isolated and when traced distally, it was found to be split from midsubstance by tumor into two limbs (Fig. 2). Both the limbs of nerve were mobilized and were brought anteriorly using a suction catheter. Tumor was excised en-bloc (Fig. 3). Excised tumor was sent for histopathological examination which confirmed it to be osteochondroma, and there was no evidence of a malignant transformation. Post-operatively, distal neurovascular status was intact, and the patient was put on weight-bearing as per pain tolerance.
Both the limbs of nerve were mobilized and were brought anteriorly using a suction catheter. Tumor was excised en-bloc (Fig. 3). Excised tumor was sent for histopathological examination which confirmed it to be osteochondroma, and there was no evidence of a malignant transformation. Post-operatively, distal neurovascular status was intact, and the patient was put on weight-bearing as per pain tolerance. The patient continued to follow-up till 1 year after surgery during which there was no evidence of any recurrence.
The patient continued to follow-up till 1 year after surgery during which there was no evidence of any recurrence.
Osteochondroma was initially reported by Sir Astley Cooper, in 1818 [4]. Osteochondroma is seen in 2–3% of the general population and represents approximately 36–41% of all benign bone tumors [5,6]. Incidence of primary bone tumors involving fibula is 2.5% [7]. In our case, osteochondroma was located in proximal fibula. In 90% of the cases, osteochondromas are solitary, and these can be sessile or pedunculated [2]. In our case also, it was solitary and sessile. Osteochondromas located at proximal fibula can not only cause compression of neurovascular structures but can also distort their normal anatomical course, thus increasing the chances of their injury [4]. Furthermore, continuous increase in size of the tumor may create mass effect on adjacent tendons. In our case, main concern was growing size of the tumor along with its abnormal location which was creating mass effect, leading to pain; however, distal neurovascular function was unharmed. MRI is the best radiologic imaging method evaluating hyaline cartilage cap [8]. It is also important for visualizing the effect of the lesion on surrounding structures and shows cortical and medullary continuity between the parent bone and osteochondroma [8]. . Normally, common peroneal nerve bifurcates into the superficial and deep peroneal nerves. However, this bifurcation can take place distal to the fibular neck, proximal to the joint line or distal to the joint line, and proximal to the fibular neck [9]. In our case, nerve was bifurcating distal to fibular neck. Furthermore, before the bifurcation could occur, we were surprised during our dissections to find the tumors actually growing through the peroneal nerve. Gray et al. in 2004 reported two such cases of an osteochondroma of the proximal fibula that was noted at surgery to grow through the common peroneal nerve, splitting it into two limbs [10]. Wankhade et al. in 2016 also reported a case of proximal fibular osteochondroma causing splitting of common peroneal nerve, leading to neuropathy in an adult [2]. Incidence of nerve compression caused by osteochondroma is <1% [11]. Moreover, it is even more rare to find nerve palsy due to osteochondroma growing through midsubstance of common peroneal nerve as was also the finding in our case [2]. Surgery for proximal fibular osteochondromas varies from simple debulking to the complete excision of proximal fibula (Malawer type I resection) [12]. In our case, tumor was excised from its base rather than removing the proximal fibula. Although the recurrence of osteochondroma after its surgical excision is rare, it may occur if a lesion which is in continuation with the physis in a growing child is not completely removed or if there is incomplete removal of the cartilaginous cap [4]. In our case, follow-up was done for a period of 1-year duration, and no recurrence was noted. Clinical features suspicious for malignant transformation comprise new onset of pain in a previously stable lesion, rapid or new growth, growth after skeletal maturity, and/or large lesions [13,14]. In our case, there was no clinical indication of any malignant transformation and histopathology report also confirmed our clinical finding.
Thus, we conclude that, by turning up such a rare case, we strive to make the surgeons aware that when removing osteochondroma located at proximal fibula, care should be taken to identify the entire nerve before removal as one may encounter such a situation where tumor is extending through the common peroneal nerve and procedure done in a hurry in such a case can cause irreversible damage to the patient.
Proximal fibula is a common site for symptomatic osteochondromas, and before excising them, it is very important to identify the anatomy of the nerve to avoid neurological injury.
References
- 1.Cardelia JM, Dormans JP, Drummond DS, Davidson RS, Duhaime C, Sutton L. Proximal fibular osteochondroma with associated peroneal nerve palsy: A review of six cases. J Pediatr Orthop 1995;15:574-7. [Google Scholar | PubMed]
- 2.Wankhade UG, Kale AR, Rawate P, Bathala G. Proximal fibular osteochondroma causing splitting of common peroneal nerve leading to neuropathy in an adult- a rare case report. Int J Med Res Rev 2016;4:1310-4. [Google Scholar | PubMed]
- 3.Mootha AK, Saini R, Dhillon M, Bali K, Dhatt SS, Kumar V. Modified resection technique for proximal fibular osteochondromas. Orthop Traumatol Surg Res 2011;97:569-73. [Google Scholar | PubMed]
- 4.Kumar M, Malgonde M, Jain P. Osteochondroma arising from the proximal fibula: A rare presentation. J Clin Diagn Res 2014;8:LD01-3. [Google Scholar | PubMed]
- 5.Karasick D, Schweitzer ME, Eschelman DJ. Symptomatic osteochondromas: Imaging features. AJR Am J Roentgenol 1997;168:1507-12. [Google Scholar | PubMed]
- 6.Griffiths HJ, Thompson RC Jr., Galloway HR, Everson LI, Suh JS. Bursitis in association with solitary osteochondromas presenting as mass lesions. Skeletal Radiol 1991;20:513-6. [Google Scholar | PubMed]
- 7.Unni K. Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases. Philadelphia, PA: Lippincot-Raven Publishers; 1996. [Google Scholar | PubMed]
- 8.Koplay M, Toker S, Sahin L, Kilincoglu V. A calcaneal osteochondroma with recurrence in a skeletally mature patient: A case report. Cases J 2009;2:7013. [Google Scholar | PubMed]
- 9.Deutsch A, Wyzykowski RJ, Victoroff BN. Evaluation of the anatomy of the common peroneal nerve. Defining nerve-at-risk in arthroscopically assisted lateral meniscus repair. Am J Sports Med 1999;27:10-5. [Google Scholar | PubMed]
- 10.Gray KV, Robinson J, Bernstein RM, Otsuka NY. Splitting of the common peroneal nerve by an osteochondroma: Two case reports. J Pediatr Orthop B 2004;13:281-3. [Google Scholar | PubMed]
- 11.Paik NJ, Han TR, Lim SJ. Multiple peripheral nerve compressions related to malignantly transformed hereditary multiple exostoses. Muscle Nerve 2000;23:1290-4. [Google Scholar | PubMed]
- 12.Malawer MM. Surgical management of aggressive and malignant tumors of the proximal fibula. Clin Orthop Relat Res 1984;186:172-81. [Google Scholar | PubMed]
- 13.Blitz NM, Lopez KT. Giant solitary osteochondroma of the inferior medial calcaneal tubercle: A case report and review of the literature. J Foot Ankle Surg 2008;47:206-12. [Google Scholar | PubMed]
- 14.Malik R, Kapoor N, Malik R. Transformation of solitary osteochondroma calcaneum to chondrosarcoma--a case report. Indian J Pathol Microbiol 2004;47:42-3. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Schwannoma Arising from the Deep Peroneal Nerve: A Case Report
July 1, 2026 Schwannoma Arising from the Deep Peroneal Nerve: A Case Report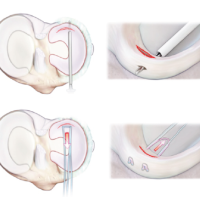 December 1, 2024 Lateral Meniscal Tears Can be Safely Repaired “All-Inside” Without Peroneal Nerve Injury: Case Series and Literature Review
December 1, 2024 Lateral Meniscal Tears Can be Safely Repaired “All-Inside” Without Peroneal Nerve Injury: Case Series and Literature Review November 10, 2023 Unusually Giant Solitary Osteochondroma of the Ilium: A Case Report with Review of Literature
November 10, 2023 Unusually Giant Solitary Osteochondroma of the Ilium: A Case Report with Review of Literature July 10, 2015 Isolated Coronal Fracture of Trapezium- A Case Report with Review of Literature
July 10, 2015 Isolated Coronal Fracture of Trapezium- A Case Report with Review of Literature