
The mechanism of trauma and the physical examination is relevant aid for the diagnosis of a dorsal DRUJ dislocation; the X-rays and CT scan confirm the diagnosis. In our case, the early elbow motion helped us to achieve a faster recovery.
Dr. Maria Grazia Minicelli, Department of Orthopaedic Surgery, University Hospital Renato Dulbecco, viale Pio X n. 83, 88100 Catanzaro, Italy. E-mail: mariagraziaminicelli@tiscali.it
Abstract
Introduction: Isolated acute distal radioulnar joint (DRUJ) dislocation is a rare condition and easy undiagnosed. Few cases are reported in the literature about its treatment. We reported a case of an isolated acute traumatic dorsal DRUJ dislocation treated with early reduction and immobilization.
Case Report: We present a case of a 12-year-old female with an isolated dorsal acute DRUJ dislocation. We performed for the early diagnosis a clinical examination, X-rays, and computed tomography scan. We treated this condition with a closed reduction and immobilization in an above-elbow cast for 4 weeks and in a below-elbow brace for 2 weeks. The outcome was good.
Conclusion: Isolated acute dorsal DRUJ dislocation is an uncommon injury; the early diagnosis and timely treatment usually result in good outcome. In our case, an early transition to below-elbow brace results in a faster recovery.
Keywords: Isolated dorsal distal radioulnar joint dislocation, closed reduction, case report.
Isolated acute dorsal distal radioulnar joint (DRUJ) dislocation is an uncommon injury with only few cases reported in the literature [1,2,3,4,5,6]. The routinely treatment of this injury consists in a closed reduction with a cast immobilization. Instead, in case of instability or irreducibility, the open reduction and surgical repair are necessary [7]. We present a case of an isolated acute traumatic dorsal DRUJ dislocation treated with cast immobilization.
A 12-year-old female student, right-handed and healthy, presented with her mother to our emergency room after a trauma of the right wrist. This trauma occurred in the car following road accident and was due to the forced pronation on outstretched forearm with the right hand in a fixed position against the windshield of the car. At physical examination, the wrist was painful, swollen with a dorsal ulnar head prominence, limited forearm supination, and limited wrist motion. The head of ulna showed a moderate ballottement compared with contralateral wrist and there were no wound and neurovascular deficit. We performed anteroposterior (AP) and lateral views of wrist X-rays that revealed a dorsal ulnar dislocation of the DRUJ without any fractures (Fig. 1).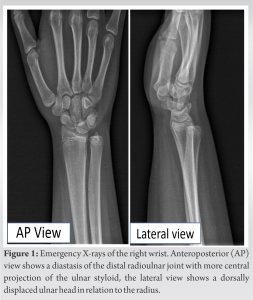 Furthermore, for an accurate diagnosis, we did a computed tomography (CT) scan that showed a dorsal ulnar dislocation (Fig. 2).
Furthermore, for an accurate diagnosis, we did a computed tomography (CT) scan that showed a dorsal ulnar dislocation (Fig. 2). At emergency room, without sedation, we performed a closed reduction by direct pressure on the ulnar head while the traction of the wrist and the gentle supination of the forearm in 90° elbow flexion were applied. We blocked the reduction with the above-elbow cast with an imprint on ulnar head at 90° of elbow flexion and a forearm in neutral position. The X-rays in AP and lateral views confirmed the DRUJ reduction (Fig. 3).
At emergency room, without sedation, we performed a closed reduction by direct pressure on the ulnar head while the traction of the wrist and the gentle supination of the forearm in 90° elbow flexion were applied. We blocked the reduction with the above-elbow cast with an imprint on ulnar head at 90° of elbow flexion and a forearm in neutral position. The X-rays in AP and lateral views confirmed the DRUJ reduction (Fig. 3).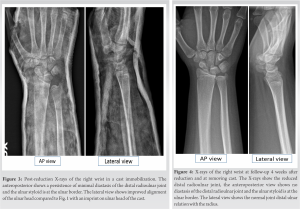 After 7 days, a radiographic examination showed the maintenance of the reduction. Twenty-eight days after casting reduction, the cast was removed and given the continuation of the reduction to new X-rays (Fig. 4); it was replaced with a below-elbow brace for 2 weeks to encourage elbow motion. After the removal of the brace, the right wrist was stable and painless and the patient started a rehabilitation program with range of motion (ROM) exercises and laser therapy within 10-day period. At follow-up, 2 months after the trauma, she presented normal ROM at wrist with any pain and instability, and no restrictions in any activity.
After 7 days, a radiographic examination showed the maintenance of the reduction. Twenty-eight days after casting reduction, the cast was removed and given the continuation of the reduction to new X-rays (Fig. 4); it was replaced with a below-elbow brace for 2 weeks to encourage elbow motion. After the removal of the brace, the right wrist was stable and painless and the patient started a rehabilitation program with range of motion (ROM) exercises and laser therapy within 10-day period. At follow-up, 2 months after the trauma, she presented normal ROM at wrist with any pain and instability, and no restrictions in any activity.
Isolated dislocation of the DRUJ is rare. This dislocation is described as volar or dorsal by the ulnar position relative to the radius. Approximately 50% of isolated RDUJ dislocations are undiagnosed or diagnosed late with significant functional consequences [8]. For the early diagnosis, it is important to investigate the mechanism of trauma and to perform a meticulous physical examination. An isolated dorsal DRUJ dislocation occurs generally during a fall onto an outstretched forearm and is due to overpronation force [1]. Furthermore, in our case, probably, the forced pronation of the wrist on outstretched forearm with the hand fixed to defend from the impact caused the isolated acute dorsal DRUJ dislocation. This injury clinically may present with a dorsal prominence of the ulnar head and the forearm fixed in pronation, but these usual signs may be confounding due to swelling and pain of injured wrist. Therefore, in case of clinical suspicion, the diagnosis should be supported with X-rays in AP and lateral views of the wrist and confirmed with a CT scan. The limit of the diagnostic value of the radiography is due both to the difficulty of performing a true lateral X-ray view of the wrist because the pain and limited motion and to the difficulty of seeing in AP X-ray view the subtle alterations between the distal radius and ulna and the atypical projection of the ulnar styloid which is not always pathognomonic of dislocation. While a single CT scan is diagnostic in all positions of forearm rotation and can assess more the subtle DRUJ instability [9]. Magnetic resonance can be performed to investigate the presence and entity of soft-tissue injuries 5–8 days after the injury [8,10]. The standard treatment of this condition consists of a closed reduction under local or general anesthesia followed by immobilization in the position of greatest stability by above-elbow cast for 6 weeks duration. In a dorsal dislocation, this is accomplished by gentle traction with direct dorsal pressure on ulnar head and fully supinating the forearm in 90° elbow flexion and held by above-elbow cast for 6 weeks [1]. We treated this dislocation with a closed reduction and immobilization by above-elbow cast in a forearm in neutral position. This position was in our case, the one with the greatest stability. We performed a closed reduction and immobilization without local or general anesthesia due to the high collaboration and pain tolerance of our patient and due to modest swollen of the wrist and the relaxation of the muscles. In case of instability or irreducibility, the open reduction and surgical repair of the triangular fibrocartilage complex are necessary [2,7]. We immobilized the wrist for 6 weeks and the elbow for 4 weeks. Four weeks after the reduction, we removed the log cast, and we applied the wrist brace. We decided for the early elbow mobilization because 28 days after the reduction, the wrist was stable and the reduction was maintained. Since the isolated acute dorsal DRUJ dislocation is rare, the treatment and its outcome are described by the series of cases reported in the literature. Daradkeh et al. [1] reported a case of early elbow motion after isolated acute dorsal DRUJ dislocation treated with closed reduction and K-wire pinning along with cast immobilization. Our case is the only one in the literature that describes the result of a conservative treatment with an early elbow motion after 4 weeks of immobilization and the use of a below-elbow brace when reduction and stability are maintained.
We believe that the information about the mechanism of trauma, the accurate physical examination as possible, and the correct radiographic projections integrated with CT scan are all necessary for the early diagnosis of isolated acute dorsal DRUJ dislocation. In our case, the maintenance of reduction and wrist stability with a long cast at 4 weeks induced us to early elbow mobilization achieving a shorter and complete recovery.
The mechanism of trauma, the physical examination, the correct X-ray’s projections, and in case of doubt, the CT scan, are all necessary for the timely diagnosis of isolated acute dorsal DRUJ dislocation. In the case of stability and maintenance of wrist, reduction may be appropriate an early elbow motion for a faster recovery.
References
- 1.Daradkeh ST, Elayan B, Daradkeh YT, Al Dabouby FS. Case report: Isolated acute dorsal distal radioulnar joint (DRUJ) dislocation. Int J Surg Case Rep 2022;95:107190. [Google Scholar | PubMed]
- 2.Wassink S, Lisowski LA, Schutte BG. Traumatic recurrent distal radioulnar joint dislocation: A case report. Strategies Trauma Limb Reconstr 2009;4:141-3. [Google Scholar | PubMed]
- 3.Alexander AH. Bilateral traumatic dislocation of the distal radioulnar joint, ulna dorsal: Case report and review of the literature. Clin Orthop Relat Res 1977;129:238-44. [Google Scholar | PubMed]
- 4.Russo MT, Maffulli N. Dorsal dislocation of the distal end of the ulna in a judo player. Acta Orthop Belg 1991;57:442-6. [Google Scholar | PubMed]
- 5.Haouzi MA, Bassir RA, Boufettal M, Kharmaz M, Lamrani MO, Mahfoud M, et al. Isolated dorsal dislocation of the distal radioulnar joint: A case report. Trauma Case Rep 2020;29:100349. [Google Scholar | PubMed]
- 6.Tarallo L, Adani R, Catani F. Closed reduction of acute volar dislocation of the distal radioulnar joint. J Hand Surg Eur Vol 2013;38:572-4. [Google Scholar | PubMed]
- 7.Szabo RM. Distal radioulnar joint instability. J Bone Joint Surg Am 2006;88:884-94. [Google Scholar | PubMed]
- 8.Dukan R, Kassab Hassan S, Delvaque JG, Khaled I, Nizard R. Isolated volar dislocation of the distal radioulnar joint: A case report. J Orthop Case Rep 2020;10:97-100. [Google Scholar | PubMed]
- 9.Duryea DM, Payatakes AH, Mosher TJ. Subtle radiographic findings of acute, isolated distal radioulnar joint dislocation. Skeletal Radiol 2016;45:1243-7. [Google Scholar | PubMed]
- 10.Starnoni M, Colzani G, De Santis G, Leti Acciaro A. Management of locked volar radio-ulnar joint dislocation. Plast Reconstr Surg Glob Open 2019;7:e2480. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Traumatic Obturator Variant of Anterior Hip Dislocation – A Case Series
May 1, 2026 Traumatic Obturator Variant of Anterior Hip Dislocation – A Case Series April 1, 2026 Dislocation and Iatrogenic Dissociation of Bipolar Hip Hemiarthroplasty: A Case Series and Literature Review
April 1, 2026 Dislocation and Iatrogenic Dissociation of Bipolar Hip Hemiarthroplasty: A Case Series and Literature Review December 1, 2025 Humerus Shaft Fracture in Adult Managed with Elastic Nails: A Case Report and Literature Review of Management Options
December 1, 2025 Humerus Shaft Fracture in Adult Managed with Elastic Nails: A Case Report and Literature Review of Management Options October 1, 2025 Simultaneous Bilateral Anterior Shoulder Dislocation Following Epileptic Seizure in a Middle-Aged Male: A Rare Case Report and Review of Literature
October 1, 2025 Simultaneous Bilateral Anterior Shoulder Dislocation Following Epileptic Seizure in a Middle-Aged Male: A Rare Case Report and Review of Literature