
Segmental rupture of Achilles tendon is a rarity, so an appropriate intervention helps to salvage the tendon segment, avoid complications secondary to its precarious vascularity, and preserve the repaired construct; eventually yielding a good functional outcome.
Dr. Soutrik Mukherjee, Department of Orthopaedics, North Bengal Medical College and Hospital, Darjeeling, West Bengal - 734 012, India. E-mail: drsoutrikmukherjee@gmail.com
Abstract
Introduction: Achilles tendon is the thickest and strongest tendon of the body, spanning from the middle of the calf up to its insertion into the calcaneal tuberosity, and it is estimated to be the third most frequent tendon to rupture. Segmental Achilles tendon rupture, however, is a very rare occurrence and it comes with challenges of salvaging the tendon segment, preventing necrosis of the overlying skin, preventing infection, and preserving the repaired construct to regain good functional outcome. We present a rare case of an acute traumatic segmental rupture of Achilles tendon in a young male, its management and outcome.
Case Report: A 25-year-old male suffered a direct blow to the posterior aspect of his left ankle above the heel and presented to us on the same day. On examination, a lacerated wound with visible ruptured ends of the tendon was found. A palpable gap was also felt over a proximal sutured wound and a real-time ultrasonography revealed a complete tear of Achilles tendon in the proximal site as well. Both the wounds were explored and a segmental Achilles tendon rupture was found. A dual level Krackow’s suturing was done with augmentation of the distal repair with anchorage in the calcaneus. Following a stringent post-operative rehabilitation, the patient was allowed weight-bearing from 12 weeks onward. At 6-month follow-up, the tendon continuity was intact both clinically and radiologically, and the patient was able to ambulate bearing full weight having bilaterally comparable ankle range of motion.
Conclusion: Rupture of Achilles tendon is relatively common; however, a segmental rupture of the tendon is very rare and poses a challenge for optimum management. Awareness about the possible complications and addressing them with a timely intervention followed by a well-balanced rehabilitation can salvage the tendon and yield good results.
Keywords: Segmental tendoachilles rupture, dual level Krackow’s repair, traumatic tendoachilles rupture
The Achilles tendon is the thickest and strongest tendon of the body [1], spanning approximately 15 cm from the middle of the calf to its insertion into the calcaneal tuberosity [2]; and it has been estimated to be the third most frequent tendon to rupture [3]. The peak age for rupture in both men and women is between 30 and 50 years of age [4]. The most common site of rupture has been related to a relatively hypovascular area of the tendon, shown by angiography between 2 cm and 6 cm from its insertion into the calcaneus. The cause of Achilles tendon rupture, however, probably is a combination of a relatively hypovascular area and repetitive microtrauma superimposed on a stiff and less viscoelastic tendon, secondary to age dependant changes in collagen crosslinking; that is unable to keep up with the stresses and a mechanical overload completes the rupture [3]. Segmental Achilles tendon rupture, however, is a very rare occurrence and it comes with challenges of salvaging the tendon segment, preventing flap necrosis of the overlying skin, preventing and controlling infection, and preserving the repaired construct as well as to regain near native functional outcome. To address, all these is difficult due to minimal reported incidence of such cases in literature. We present a rare case of an acute traumatic segmental rupture of Achilles tendon in a young male, its management and outcome.
A 25-year-old male suffered an injury by a direct blow from the lower edge of steel cupboard, on the posterior aspect of his left ankle above the heel. He presented to us on the same day, after initially being treated at a local subcentre, with pain and a bleeding lacerated wound over the retro calcaneal region of his left ankle, and a sutured wound of 2 cm linear dimension (suturing done elsewhere), 5 cm proximal to the open wound. The patient was unable to walk. On examination, a lacerated wound of 4 cm * 2 cm dimensions was seen, about 2.5 cm proximal to the insertion of the Achilles tendon of his left ankle, with a palpable gap between the visible ruptured ends of the tendon. Thompson squeeze test and Matles test were positive. Toe raise on the affected side was absent. A palpable gap was also felt over the proximal sutured wound and a real-time ultrasonography (USG) revealed a complete tear of Achilles tendon in the proximal site as well (Fig. 1). The patient had no history of any medical illness. His routine blood investigations were normal. Informed patient consent was obtained for treatment. Both the wounds were explored on the operating table and a segmental Achilles tendon rupture was found (Fig. 2). 
Initially, an attempt to repair without incising the intervening skin was tried; however, the skin was eventually incised along the midline preserving the cutaneous vascularity to facilitate better exposure. A dual level Krackow’s suturing was done (Fig. 3); along with augmentation of the distal repair with anchorage in the calcaneus using ethibond no. 5 sutures. To ensure the preservation of tendon segment vascularity, the para-tenon was maintained in its position. Skin was repaired without tension (Fig. 4).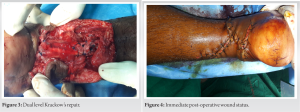 Entire procedure was done applying tourniquet that was released after complete closure. An above knee plaster of paris slab with the ankle in 20 degrees of plantar flexion was applied for 4 weeks followed by a below knee plaster for another 2 weeks, to facilitate knee mobilisation. At 6 weeks, the plaster was removed and non-weight-bearing range of motion exercises of the ankle was begun. However, 3 weeks later, the patient presented with restricted dorsiflexion, for which weekly manipulation followed by below knee plaster casts with ankle in maximum possible dorsiflexion was done for another 3 weeks. The patient was allowed weight-bearing as bearable from 12 weeks onward with weight-bearing range of motion exercises.
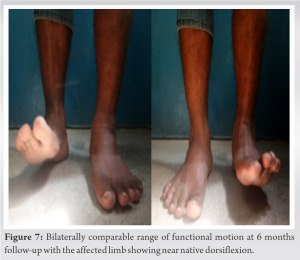
Entire procedure was done applying tourniquet that was released after complete closure. An above knee plaster of paris slab with the ankle in 20 degrees of plantar flexion was applied for 4 weeks followed by a below knee plaster for another 2 weeks, to facilitate knee mobilisation. At 6 weeks, the plaster was removed and non-weight-bearing range of motion exercises of the ankle was begun. However, 3 weeks later, the patient presented with restricted dorsiflexion, for which weekly manipulation followed by below knee plaster casts with ankle in maximum possible dorsiflexion was done for another 3 weeks. The patient was allowed weight-bearing as bearable from 12 weeks onward with weight-bearing range of motion exercises.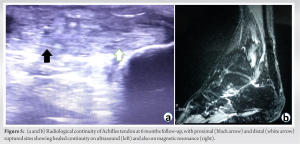 At 6-month follow-up, the tendon continuity was intact both clinically and radiologically (Fig. 5a and b), and the patient has been able to ambulate bearing full weight (Fig. 6) and with bilaterally comparable range of motion of the ankle (Fig. 7).
At 6-month follow-up, the tendon continuity was intact both clinically and radiologically (Fig. 5a and b), and the patient has been able to ambulate bearing full weight (Fig. 6) and with bilaterally comparable range of motion of the ankle (Fig. 7).
Initial descriptions of Achilles tendon injuries dates back to the time of Hippocrates [5]. Complete rupture of Achilles tendon, traumatic or non-traumatic was relatively rare but the frequency of these injuries is increasing as more people remain active in recreational sports for longer times [3]. Repeated microtrauma and healing leads to accumulation of Type III collagen at the rupture site, with thin collagen fibres and decreased tensile strength [6]. This, in association with the hypovascularity of the rupture site, gives way to mechanical stresses. Patients usually present with pain in the leg at the time of the injury and are unable to bear weight [7]. Disruption of the tendon from a direct blow can lead to a laceration. The diagnosis of Achilles tendon rupture can be reliably made with a palpable tendon defect along with some tell-tale diagnostic tests and signs. Real-time high-resolution USG of the Achilles tendon is more sensitive than soft-tissue radiography and gives dynamic images of the tendon [8]. The USG image shows heterogeneous hypoechoic areas with discontinuity and fluid-filled spaces, which is suggestive of a ruptured tendon. For the management of simple rupture of Achilles tendon, there are well-established indications for non-operative management as well as different modalities of operative intervention[1]. However, the incidence of segmental rupture of tendoachilles is very minimal in literature and thus there exists no convention regarding the approach to management and more importantly the rehabilitation. Delay in presentation moreover poses a significant difficulty in reconstruction, more so in a case of segmental rupture. The blood supply to the Achilles tendon is precarious (Fig. 8), with predominant artery being the recurrent branch of the posterior tibial artery supplying through the paratendinous tissues [9,10]. 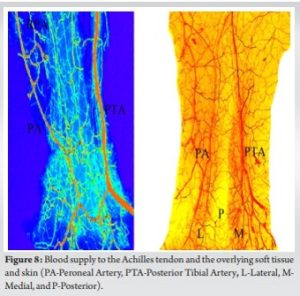 Minimal paratendinous dissection was done with maximal preservation of the paratenon so as to salvage the vascularity of the tendon segment. The skin flap overlying the tendon segment receives cutaneous supply from the posterior tibial artery and the peroneal artery from medial and lateral aspects, respectively (Fig. 8). Hence, the skin was incised in midline to facilitate tendon repair, preserving as much vascularity and was, repaired without tension to prevent skin flap necrosis. Due to a lack of consensus regarding the management and rehabilitation protocol in a case of segmental rupture of Achilles tendon, there needs to be a fine balance between the onset of non-weight-bearing functional rehabilitation to prevent stiffness, contracture, deformities, and to initiate progressive weight-bearing keeping the repaired construct intact. In our case, we initiated non-weight-bearing rehabilitation exercises from 6 weeks onward with ankle range of motion and stretching exercises and allowed progressive weight-bearing from 12 weeks onward. Our patient achieved satisfactory healing and at 6 months follow-up was bearing full weight during ambulation with bilaterally comparable ankle range of motion.
Minimal paratendinous dissection was done with maximal preservation of the paratenon so as to salvage the vascularity of the tendon segment. The skin flap overlying the tendon segment receives cutaneous supply from the posterior tibial artery and the peroneal artery from medial and lateral aspects, respectively (Fig. 8). Hence, the skin was incised in midline to facilitate tendon repair, preserving as much vascularity and was, repaired without tension to prevent skin flap necrosis. Due to a lack of consensus regarding the management and rehabilitation protocol in a case of segmental rupture of Achilles tendon, there needs to be a fine balance between the onset of non-weight-bearing functional rehabilitation to prevent stiffness, contracture, deformities, and to initiate progressive weight-bearing keeping the repaired construct intact. In our case, we initiated non-weight-bearing rehabilitation exercises from 6 weeks onward with ankle range of motion and stretching exercises and allowed progressive weight-bearing from 12 weeks onward. Our patient achieved satisfactory healing and at 6 months follow-up was bearing full weight during ambulation with bilaterally comparable ankle range of motion.
Rupture of Achilles tendon is a relatively common entity; however, a segmental rupture of the tendon is very rare and comes with challenges of salvaging the tendon segment, preventing flap necrosis of the overlying skin, preventing and controlling infection and preserving the repaired construct; as well as to regain near native functional outcome. Awareness about the possible complications and addressing them with a timely intervention followed by a well-balanced rehabilitation protocol can salvage the tendon and yield good results.
A traumatic segmental rupture of Achilles tendon is a rare complex presentation which not only needs a diligent, meticulous management but more importantly a rigid rehabilitation protocol so as to restore the near native functional abilities.
References
- 1.Yang X, Meng H, Quan Q, Peng J, Lu S, Wang A. Management of acute Achilles tendon ruptures: A review. Bone Joint Res 2018;7:561-9. [Google Scholar | PubMed]
- 2.Standring S, Borley NR, Gray, H. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 40th ed., Anniversary ed. Edinburgh: Churchill Livingstone/Elsevier; 2008. p. 1451. [Google Scholar | PubMed]
- 3.Azar FM, Beaty JH, Canale ST. Campbell’s Operative Orthopaedics. Philadelphia, PA: Elsevier; 2017. p. 2415-16. [Google Scholar | PubMed]
- 4.Hanlon DP. Bilateral Achilles tendon rupture: An unusual occurrence. J Emerg Med 1992;10:559-60. [Google Scholar | PubMed]
- 5.Haines JF. Bilateral rupture of the Achilles tendon in patients on steroid therapy. Ann Rheum Dis 1983;42:652-4. [Google Scholar | PubMed]
- 6.Eriksen HA, Pajala A, Leppilahti J, Risteli J. Increased content of Type III collagen at the rupture site of human Achilles tendon. J Orthop Res 2002;20:1352-7. [Google Scholar | PubMed]
- 7.Hattrup SJ, Johnson KA. A review of ruptures of the Achilles tendon. Foot Ankle 1985;6:34-8. [Google Scholar | PubMed]
- 8.Fornage BD, Rifkin MD. Ultrasound examination of tendons. Radiol Clin North Am 1988;26:87-107. [Google Scholar | PubMed]
- 9.Ahmed IM, Lagopoulos M, McConnell P, Soames RW, Sefton GK. Blood supply of the Achilles tendon. J Orthop Res 1998;16:591-6. [Google Scholar | PubMed]
- 10.Chen TM, Rozen WM, Pan WR, Ashton MW, Richardson MD, Taylor GI. The arterial anatomy of the Achilles tendon: anatomical study and clinical implications. Clin Anat. 2009 Apr;22(3):377-85. doi: 10.1002/ca.20758. PMID: 19173244. [Google Scholar | PubMed | CrossRef]


Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2025 Hybrid External Fixation as A Comprehensive, Safe, and Effective Solution for Periarticular Tibial Fracture with Soft Tissue Compromise
March 1, 2025 Hybrid External Fixation as A Comprehensive, Safe, and Effective Solution for Periarticular Tibial Fracture with Soft Tissue Compromise July 1, 2025 The Power of Monotony
July 1, 2025 The Power of Monotony April 1, 2025 Bilateral Anterior Shoulder Dislocations with Greater Tuberosity Fractures Study Design: A Case Report
April 1, 2025 Bilateral Anterior Shoulder Dislocations with Greater Tuberosity Fractures Study Design: A Case Report December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System
December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System