
A bilateral paired calcaneal spur is a rare radiological entity and has not been reported yet in the literature.
Dr. Sanjay K Rai, Department of Orthopaedics, Military Hospital, Ambala, Haryana, India. E-mail: skrai47@yahoo.com
Abstract
Introduction: Heel pain is one of the most common painful conditions of the foot. There are many causes of heel pain, which are usually associated with calcaneal spurs. Hence, it becomes imperative to diagnose and treat them effectively. The development of calcaneal spur is somewhat not well known but is often said to be developed from inflamed plantar fascia. Heel being weight-bearing part of the body, it is very painful something and adversely affects the activity of daily living. Calcaneal spurs are fibrocartilaginous triangular projections from an insertional area of the plantar fascia. Calcaneal spurs are usually single in number but can vary in size. Paired or double calcaneal spurs are not yet reported in the literature and further, the occurrence of bilateral paired calcaneal spurs is extremely rare too. The aim of this case report is to report the occurrence of bilateral paired or double calcaneal spurs.
Case Report: A 56-year-old man presented himself at the orthopedics outpatient department with spontaneous onset bilateral heel pain for the past few months. The pain was more in the morning as soon as he gets up from bed and persisted throughout the day with variable intensity.
Conclusion: The presence of calcaneal spur is usually symptomatic and may be asymptomatic sometimes. The presence of symptomatic bilateral paired calcaneal spur is rare and the present case report may be helpful for further study.
Keywords: Paired calcaneal spur, calcaneal spur, heel pain, plantar fasciitis.
Plettner [1] in 1990 described exostoses of the heel bone. Calcaneal spurs are fibro-cartilaginous triangular projections arising from an insertional area from the calcaneus (calcaneal tuberosity) and with variable sizes described by Kuyucu et al. [2]. Şahin and Sabri Balik [3] have studied the correlation of heel pain with various slop and length of the calcaneal spur and found that slope of <30° and length of <10 mm do not create much pain. Two types of calcaneal spur have been reported depending on their location, dorsal calcaneal spur on dorsum of calcaneus, and plantar calcaneal spur on the plantar surface [4]. Further Zhou et al. [5] described another two types of calcaneal spurs, Type A calcaneal spurs which are present superior to the plantar fascial insertion, and Type B calcaneal spurs present within the plantar fascia. Plantar calcaneal spurs may arise from medial or lateral calcaneal tuberosity. Calcaneal tuberosity is related to the plantar fascia, which is a dense connective tissue rich in fibrocytes. Plantar fascia is attached to the medial aspect of the calcaneal tuberosity and extends to the digits of the foot. The latter is supposed to maintain the medial foot arch and act as a shock absorber during weight bearing [4].
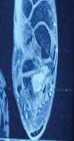
A 56-year-old man presented himself at orthopedics outpatient department with spontaneous onset bilateral heel pain for the past few months. The pain was more in the morning as soon as he gets up from bed and persisted throughout the day with variable intensity. He has no medical comorbidities such as obesity, diabetes, hypertension, autoimmune disease, and rheumatic disorder.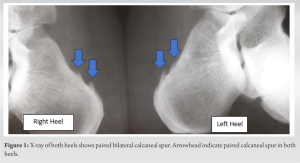 He was a sedentary office worker with no history of smoking; however, he was a social drinker. His both heel’s physical examination revealed point tenderness over the medial aspect of both heels on the plantar aspect with mild swelling. His medial plantar arch was well maintained and no neurological disturbance over the foot was detected. Based on clinical presentation, diagnosis of plantar fasciitis was made and he was advised for a plain X-ray of both heel axial and lateral view which revealed a bilateral paired calcaneal spur (proximal spur was about 4 mm long and distal spur 3 mm long in both heel), as shown in Figure 1. Ultrasonography of both heels showed thickened plantar fascia. Other hematological and rheumatological investigations were unremarkable, Table 1. There are various pharmacological and non-pharmacological treatment modalities available. Still, patients are usually suffering from heel pain due to the lack of standardized treatment modalities used clinically. Non-pharmacological treatment modalities include ultrasound, radiofrequency, extracorporeal shock wave therapy, laser therapy, silicon medial arch support, modified shoes, splints, physiotherapy, stretching, and taping. Pharmacological therapy includes non-steroidal anti-inflammatory drugs, local steroids infiltration, and local infiltration of steroids combined with a long-acting local anesthetic agent. Our patient received combined pharmacological therapy (non-steroidal anti-inflammatory drugs, Naproxen 500 mg twice a day for 7 days and non-pharmacological treatment modalities, ultrasound therapy with the dose at 0.5 w/cm 2, 3 MHz, pulsed 1:4, for 8 min, for 7 days, with this combined therapy, he has improved as far as in pain intensity is concerned.
He was a sedentary office worker with no history of smoking; however, he was a social drinker. His both heel’s physical examination revealed point tenderness over the medial aspect of both heels on the plantar aspect with mild swelling. His medial plantar arch was well maintained and no neurological disturbance over the foot was detected. Based on clinical presentation, diagnosis of plantar fasciitis was made and he was advised for a plain X-ray of both heel axial and lateral view which revealed a bilateral paired calcaneal spur (proximal spur was about 4 mm long and distal spur 3 mm long in both heel), as shown in Figure 1. Ultrasonography of both heels showed thickened plantar fascia. Other hematological and rheumatological investigations were unremarkable, Table 1. There are various pharmacological and non-pharmacological treatment modalities available. Still, patients are usually suffering from heel pain due to the lack of standardized treatment modalities used clinically. Non-pharmacological treatment modalities include ultrasound, radiofrequency, extracorporeal shock wave therapy, laser therapy, silicon medial arch support, modified shoes, splints, physiotherapy, stretching, and taping. Pharmacological therapy includes non-steroidal anti-inflammatory drugs, local steroids infiltration, and local infiltration of steroids combined with a long-acting local anesthetic agent. Our patient received combined pharmacological therapy (non-steroidal anti-inflammatory drugs, Naproxen 500 mg twice a day for 7 days and non-pharmacological treatment modalities, ultrasound therapy with the dose at 0.5 w/cm 2, 3 MHz, pulsed 1:4, for 8 min, for 7 days, with this combined therapy, he has improved as far as in pain intensity is concerned.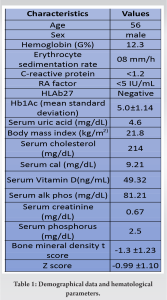
Calcaneal spur arises from the calcaneal tuberosity, situated at the posterior plantar surface of the calcaneus. However, usually, calcaneal spurs arise from the medial aspect of calcaneal tuberosity, but they can also arise from the lateral processes and the sulcus [6,7,8]. Many authors recorded the variable anatomical appearance of calcaneal spurs as simple or irregular [9,10]. Duvries [11] and Brody [12] recorded that the simple calcaneal spurs are triangular with a sharp point and with a wider base. Rubin and Witten [8] and Resnick et al. [10] have described calcaneal spurs as smooth sclerotic cortical borders and well-developed trabeculae. Conventionally, plantar fasciitis was considered an inflammatory condition; however, recent studies have shown a degenerative process [13]. Repeated biomechanical stress and microtrauma by prolonged running, standing jumping, or parade, thus causing microtears at the calcaneal fascia’s and are responsible for the degeneration of the plantar fascia [14]. Many studies reported the presence of calcaneal spur in 75.9–89% of the cases with plantar fasciitis [2,3,15]. However, the presence of calcaneal spurs in asymptomatic patients was reported in 16–46% in various studies [2,15,16]. Vaish and Vaishya also reported painful non-union of broken calcaneal spur [17]. Later on, Aliessa [18] reported a fracture of the calcaneal spur following the fall. The presence of calcaneal spur is usually symptomatic and may be asymptomatic sometimes. Various types of calcaneal spur have been described in the literature such as its length, slop, location, types, and fractured spur may affect the intensity of pain and management protocol. However, the presence of symptomatic bilateral paired calcaneal spur has not yet been reported in the literature so far.
The presence of calcaneal spur is usually symptomatic and may be asymptomatic sometimes. The presence of symptomatic bilateral paired calcaneal spur is rare and the present case report may be helpful for further study.
Various types of calcaneal spur have been described in the literature such as short, long, slopped, and fractured; however, bilateral paired calcaneal spur has not been reported so far in the literature.
References
- 1.Plettner P. Exostoses of the Heel Bone. Annual Report of the Society for Nature and Medicine in Dresden; 1900. [Google Scholar | PubMed]
- 2.Kuyucu E, Koçyiğit F, Erdil M. The association of calcaneal spur length and clinical and functional parameters in plantar fasciitis. Int J Surg 2015;21:28-31. [Google Scholar | PubMed]
- 3.Şahin R, Sabri Balik M. Does the slope and length of the plantar calcaneal spur affect the clinic? Acta Orthop Belg 2023;89:146-51. [Google Scholar | PubMed]
- 4.Menz HB, Thomas MJ, Marshall M, Rathod-Mistry T, Hall A, Chesterton LS, et al. Coexistence of plantar calcaneal spurs and plantar fascial thickening in individuals with plantar heel pain. Rheumatology (Oxford) 2019;58:237-45. [Google Scholar | PubMed]
- 5.Zhou B, Zhou Y, Tao X, Yuan C, Tang K. Classification of calcaneal spurs and their relationship with plantar fasciitis. J Foot Ankle Surg 2015;54:594-600. [Google Scholar | PubMed]
- 6.Kirkpatrick J, Yassaie O, Mirjalili SA. The plantar calcaneal spur: A review of anatomy, histology, etiology and key associations. J Anat 2017;230:743-51. [Google Scholar | PubMed]
- 7.Roland O. Pathogenesis of spur formation on the os calcis. J Bone Joint Surg 1912;2:257-74. [Google Scholar | PubMed]
- 8.Rubin G, Witten M. Plantar calcaneal spurs. Am J Orthop 1963;5:38-41. [Google Scholar | PubMed]
- 9.Mason RM, Murray RS, Oates JK, Young AC. A comparative radiological study of Reiter’s disease, rheumatoid arthritis and ankylosing spondylitis. J Bone Joint Surg Br 1959;41-B:137-48. [Google Scholar | PubMed]
- 10.Resnick D, Feingold ML, Curd J, Niwayama G, Goergen TG. Calcaneal abnormalities in articular disorders. Rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, and Reiter syndrome. Radiology 1977;125:355-66. [Google Scholar | PubMed]
- 11.Duvries HL. Heel spur (calcaneal spur). AMA Arch Surg 1957;74:536-42. [Google Scholar | PubMed]
- 12.Brody B. Progressive changes in the pathology of a heel spur. J Am Podiatry Assoc 1962;52:754-5. [Google Scholar | PubMed]
- 13.Tu P, Bytomski JR. Diagnosis of heel pain. Am Fam Physician 2011;84:909-16. [Google Scholar | PubMed]
- 14.Thomas JL, Christensen JC, Kravitz SR, Mendicino RW, Schuberth JM, Vanore JV, et al. The diagnosis and treatment of heel pain: A clinical practice guideline-revision 2010. J Foot Ankle Surg 2010;49:S1-19. [Google Scholar | PubMed]
- 15.Johal KS, Milner SA. Plantar fasciitis and the calcaneal spur: Fact or fiction? Foot Ankle Surg 2012;18:39-41. [Google Scholar | PubMed]
- 16.Menz HB, Zammit GV, Landorf KB, Munteanu SE. Plantar calcaneal spurs in older people: Longitudinal traction or vertical compression? J Foot Ankle Res 2008;1:7. [Google Scholar | PubMed]
- 17.Vaish A, Vaishya R. Bilateral broken calcaneal spurs. BMJ Case Rep 2020;13:e234138. [Google Scholar | PubMed]
- 18.Aliessa KA. A case report of bilateral calcaneal spur fracture after fall from a height. J Orthop Case Rep 2022;12:68-70. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report
July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report May 1, 2026 Surgical Treatment of Anchor-induced Heel Pain after Minimally Invasive Repair of Acute Achilles Tendon Rupture Using Percutaneous Achilles Repair System Achilles Midsubstance SpeedBridge™ Repair: A Case Report
May 1, 2026 Surgical Treatment of Anchor-induced Heel Pain after Minimally Invasive Repair of Acute Achilles Tendon Rupture Using Percutaneous Achilles Repair System Achilles Midsubstance SpeedBridge™ Repair: A Case Report December 1, 2025 A Prospective Case Series: Functional Outcomes after Calcaneal Tuberosity Partial Resection for Haglund’s Syndrome
December 1, 2025 A Prospective Case Series: Functional Outcomes after Calcaneal Tuberosity Partial Resection for Haglund’s Syndrome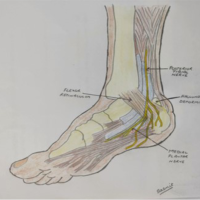 February 10, 2024 Heel Pain Management in Haglund’s Deformity Targeting Sural Nerve Branches under Ultrasound Guidance: Case Report
February 10, 2024 Heel Pain Management in Haglund’s Deformity Targeting Sural Nerve Branches under Ultrasound Guidance: Case Report