
Muscle-type flexor carpi radialis brevis can be sutured to the hypoplastic pronator quadratus to cover the volar locking plate.
Dr. Takafumi Hosokawa, Department of Orthopaedics Surgery, Tone Chuo Hospital, Numata, Japan. E-mail: thosokawa310@gmail.com
Abstract
Introduction: The flexor carpi radialis brevis (FCRB) is a rare anatomical variation, with a reported prevalence ranging from 0.9% to 8.7%. Our previous report showed three cases of FCRB in distal radius fracture (DRF) and found that hypoplastic pronator quadratus (PQ) adjacent to the FCRB muscle made it difficult to cover a volar locking plate (VLP). As we subsequently experienced additional six FCRBs, we report on new findings and surgical tips.
Case Report: VLP fixation was performed on DRF with FCRB in nine limbs of eight patients. The prevalence was 2.9% (9 of 310 limbs). Of the seven patients that underwent unilateral surgery, six were muscle type and one was tendon type. One patient who underwent bilateral surgery had a muscle type on the left and a tendon type on the right. In three muscle types, as the FCRB muscle belly was widely attached to the radial side of the radius and the radial side of the PQ was hypoplastic, postoperative covering of the plate by repair of the PQ was impossible. Then, in two of those cases, the PQ and FCRB were sutured and the plate was covered. FCRB muscle could be retracted to the radial side in all cases. One patient with a tendon type had a ruptured tendon, which was left unrepaired. All patients had no postoperative problems.
Conclusion: In the muscle-type FCRB, the muscle should be retracted to the radial side for VLP fixation. The muscle belly might occupy the radial side of the radius, and the PQ might be hypoplastic and unrepairable. However, the plate can be covered by suturing the PQ and FCRB.
Keywords: Flexor carpi radialis brevis, distal radius fracture, hypoplastic pronator quadratus.
The flexor carpi radialis brevis (FCRB) is a rare anatomical variation, with a reported prevalence ranging from 0.9% to 8.7% [1-13]. Nowadays, the most common distal radius fracture (DRF) surgery is volar locking plate (VLP) fixation, and there are many opportunities to expose the palmar side of the radius. The presence of the FCRB has been reported [1-8], and its morphology has been reported to be of the muscle type and tendon type [1,2]. Our previous report showed three cases of FCRB in DRF and found that hypoplastic pronator quadratus (PQ) adjacent to the FCRB muscle made it difficult to cover a VLP [3]. As we subsequently experienced additional six FCRBs, we report on new findings and surgical tips.
VLP fixation was performed on DRF with FCRB in eight cases and nine limbs from April 2011 to March 2023 (Table 1).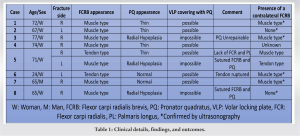 The operation was performed with a transflexor carpi radialis (FCR) approach in all cases. Nine of 310 limbs (2.9%) had FCRB. Of the patients with FCRB, five of seven patients (71%) had bilateral FCRB (checked by ultrasonography; GE Healthcare Japan L4-12r-RS6). All patients had no FCRB-related symptoms before the injury. Six of the seven patients that underwent unilateral surgery had muscle-type FCRB and one had tendon-type FCRB. One patient with bilateral DRF underwent bilateral surgery and FCRB was identified in both hands (Case 5); a muscle type on the left and a tendon type on the right. In all cases, the FCRB could be retracted to the radial side and did not interfere with the surgery. In three of the muscle types (Cases 3, 5, and 8), the FCRB was widely attached to the radial side of the radius and the radial side of the PQ was hypoplastic, so postoperative repair of the PQ was impossible. In Case 3, as previously reported, the PQ could not be repaired, so a new procedure was performed from that experience; in Cases 5 and 8, the PQ and FCRB were sutured so that the plate was covered. One patient with a tendon type had a torn FCRB tendon but was left unrepaired (Case 6). However, there were no subsequent complaints. In all cases, the fractures healed and there were no severe complications.
The operation was performed with a transflexor carpi radialis (FCR) approach in all cases. Nine of 310 limbs (2.9%) had FCRB. Of the patients with FCRB, five of seven patients (71%) had bilateral FCRB (checked by ultrasonography; GE Healthcare Japan L4-12r-RS6). All patients had no FCRB-related symptoms before the injury. Six of the seven patients that underwent unilateral surgery had muscle-type FCRB and one had tendon-type FCRB. One patient with bilateral DRF underwent bilateral surgery and FCRB was identified in both hands (Case 5); a muscle type on the left and a tendon type on the right. In all cases, the FCRB could be retracted to the radial side and did not interfere with the surgery. In three of the muscle types (Cases 3, 5, and 8), the FCRB was widely attached to the radial side of the radius and the radial side of the PQ was hypoplastic, so postoperative repair of the PQ was impossible. In Case 3, as previously reported, the PQ could not be repaired, so a new procedure was performed from that experience; in Cases 5 and 8, the PQ and FCRB were sutured so that the plate was covered. One patient with a tendon type had a torn FCRB tendon but was left unrepaired (Case 6). However, there were no subsequent complaints. In all cases, the fractures healed and there were no severe complications.
Representative cases
Case 3 (muscle type)
A 77-year-old woman with a right DRF underwent surgery. Trans-FCR approach was performed and a muscle-type FCRB appeared, occupying the radial side of the radius. Retracting the FCRB muscle to the radial side, a radial-side hypoplastic PQ appeared. VLP fixation was performed as planned, however, the PQ was unrepairable, and the plate could not be covered (Fig. 1).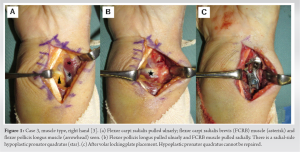 Ultrasonography 3 months after surgery showed that FCRB and flexor pollicis longus (FPL) were close to the plate, and the FCRB muscle was also found on the healthy side (Fig. 2). Although the patient’s progress was good, the plate was removed 9 months postoperatively to avoid FPL tendon rupture.
Ultrasonography 3 months after surgery showed that FCRB and flexor pollicis longus (FPL) were close to the plate, and the FCRB muscle was also found on the healthy side (Fig. 2). Although the patient’s progress was good, the plate was removed 9 months postoperatively to avoid FPL tendon rupture.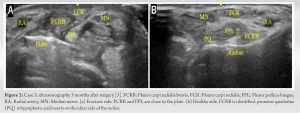
Case 8 (muscle type)
A 65-year-old woman with a right DRF underwent surgery. Muscle-type FCRB and hypoplastic PQ were confirmed as in Case 3. The radial portion of the PQ was attached to the FCRB. VLP fixation was performed as planned, however, the hypoplastic PQ was likewise unrepairable. Therefore, the FCRB and PQ were sutured and the plate was successfully covered (Fig. 3). The postoperative course was good, with no signs of FPL interference with the plate, so plate removal was not performed.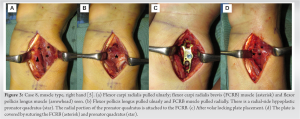
Case 5 (tendon type)
A 71-year-old woman with bilateral DRF underwent surgery. On the right hand, tendon-type FCRB was confirmed. The present case additionally lacked the palmaris longus and FCR (Fig. 4). The PQ was thin but repairable after VLP fixation.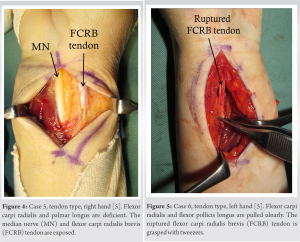
Case 6 (tendon type)
A 27-year-old woman with a left DRF underwent surgery. Tendon-type FCRB was identified and ruptured (Fig. 5). There were no tendon degeneration or synovial hyperplasia findings. The tendon component of the FCRB tendon was not found proximally in this surgical field, so it was left unrepaired. The PQ was normal. VLP fixation was performed as planned and the PQ was repaired. The postoperative course was good and there were no subsequent complaints.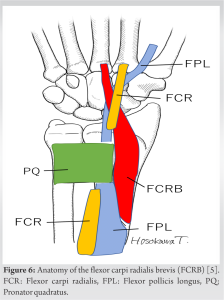
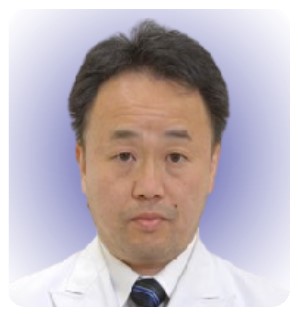
FCRB was present in 2.9% (9 of 310) of DRF limbs, similar to previous reports (0.9 to 8.7%) [1-13] (Table 2).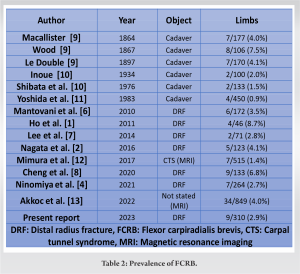 First described by Fano in 1851, FCRBs have been sporadically reported in cadavers [9- 11]. Since 2010, FCRBs in DRF surgery have been reported [1- 8]. The anatomy is reported to begin on the radial palmar surface of the radius between the distal insertion of the pronator teres and the PQ, run along the palmar aspect of the PQ into the fibrous sheath of the FCR, and insert at the base of the 2nd–4th metacarpals or at the radial carpal bone (Fig. 6) [9]. In addition to the presence of muscle type and tendon type, there is a possibility that various anomalies may be present, such as hypoplastic PQ as in the present case, deficient FCR and PL as in Case 5, and those that FCRB join the extensor carpi radialis brevis at the palm [10] or pass within the carpal tunnel [11] as reported in previous anatomical studies. Regarding the surgical approach, the authors retracted all FCRBs radially and had no difficulty with VLP placement; Ninomiya et al. also recommended that the FCRB muscle, which has a large muscle belly, be moved away radially for VLP fixation [4]. Whereas, Dodds stated that the FCRB could be usually retracted ulnarly but may require complete elevation of the muscle if the origin is distal [14]. To achieve reduction and plate fixation in DRF treatment, Laugharne and Power fully released the FCRB [15], and Werntz et al. resected the FCRB [16]. Because variation in FCRBs has been reported, depending on the shape and size of the FCRB, it might be impossible to move the FCRB to the radial side. Fortunately, we may just not have encountered such a case. However, in the VLP fixation for DRF, because of the importance of exposure of the distal ulnar side of the radius related to the fixation of the volar rim [17], we believe it is better to retract the FCRB to the radial side if possible. When a VLP is placed on a DRF, covering the plate by repairing the PQ is recommended to prevent interference between the FPL tendon and the plate [18]. However, past reports noted that if the muscle belly of the FCRB is developed, it may occupy the PQ insertion on the distal radius and cause hypoplastic radial portion of the PQ [2,3,4,5,14]. We sutured the FCRB muscle and PQ and covered the plate in Cases 5 and 8, based on our experience in Case 3, in which a hypoplastic PQ could not be repaired. Although only two cases, no complaints related to FCRB muscle occurred during the course of the treatment, and we believe that this is a good technique in cases like these. Meanwhile, when the FCRB is of the tendon type, inflammation and rupture due to interference with the plate are concerned. Nagata et al. reported tenosynovitis of the FCRB tendon in one of two patients with DRF with tendon-type FCRB [2]. In addition, cases of FCRB tendon rupture and tenosynovitis have been reported, although they were not associated with DRF [19,20]. These reports suggest that the FCRB tendon should be treated with attention to tenosynovitis and that the PQ should be repaired to avoid interference not only with the FPL tendon but also with the FCRB tendon when a VLP is placed on the DRF. However, since the FCRB tendon itself was not functionally important, and no complaints occurred even when the rupture was left untreated as in Case 6, it is considered that repair of the FCRB tendon is not necessarily important when it is ruptured, as long as the FCR is not deficient.
First described by Fano in 1851, FCRBs have been sporadically reported in cadavers [9- 11]. Since 2010, FCRBs in DRF surgery have been reported [1- 8]. The anatomy is reported to begin on the radial palmar surface of the radius between the distal insertion of the pronator teres and the PQ, run along the palmar aspect of the PQ into the fibrous sheath of the FCR, and insert at the base of the 2nd–4th metacarpals or at the radial carpal bone (Fig. 6) [9]. In addition to the presence of muscle type and tendon type, there is a possibility that various anomalies may be present, such as hypoplastic PQ as in the present case, deficient FCR and PL as in Case 5, and those that FCRB join the extensor carpi radialis brevis at the palm [10] or pass within the carpal tunnel [11] as reported in previous anatomical studies. Regarding the surgical approach, the authors retracted all FCRBs radially and had no difficulty with VLP placement; Ninomiya et al. also recommended that the FCRB muscle, which has a large muscle belly, be moved away radially for VLP fixation [4]. Whereas, Dodds stated that the FCRB could be usually retracted ulnarly but may require complete elevation of the muscle if the origin is distal [14]. To achieve reduction and plate fixation in DRF treatment, Laugharne and Power fully released the FCRB [15], and Werntz et al. resected the FCRB [16]. Because variation in FCRBs has been reported, depending on the shape and size of the FCRB, it might be impossible to move the FCRB to the radial side. Fortunately, we may just not have encountered such a case. However, in the VLP fixation for DRF, because of the importance of exposure of the distal ulnar side of the radius related to the fixation of the volar rim [17], we believe it is better to retract the FCRB to the radial side if possible. When a VLP is placed on a DRF, covering the plate by repairing the PQ is recommended to prevent interference between the FPL tendon and the plate [18]. However, past reports noted that if the muscle belly of the FCRB is developed, it may occupy the PQ insertion on the distal radius and cause hypoplastic radial portion of the PQ [2,3,4,5,14]. We sutured the FCRB muscle and PQ and covered the plate in Cases 5 and 8, based on our experience in Case 3, in which a hypoplastic PQ could not be repaired. Although only two cases, no complaints related to FCRB muscle occurred during the course of the treatment, and we believe that this is a good technique in cases like these. Meanwhile, when the FCRB is of the tendon type, inflammation and rupture due to interference with the plate are concerned. Nagata et al. reported tenosynovitis of the FCRB tendon in one of two patients with DRF with tendon-type FCRB [2]. In addition, cases of FCRB tendon rupture and tenosynovitis have been reported, although they were not associated with DRF [19,20]. These reports suggest that the FCRB tendon should be treated with attention to tenosynovitis and that the PQ should be repaired to avoid interference not only with the FPL tendon but also with the FCRB tendon when a VLP is placed on the DRF. However, since the FCRB tendon itself was not functionally important, and no complaints occurred even when the rupture was left untreated as in Case 6, it is considered that repair of the FCRB tendon is not necessarily important when it is ruptured, as long as the FCR is not deficient.
FCRB was present in 2.9% (9 of 310 limbs) of DRF limbs, and 71% (5 of 7 patients) had bilateral FCRB. In the muscle-type FCRB, the muscle should be retracted to the radial side for VLP fixation. The PQ might be hypoplastic and unrepairable. Then, the plate can be covered by suturing the PQ and FCRB.
With the current mainstream of volar plate fixation for DRFs, FCRB is not unlikely to be encountered. Orthopedic surgeons need to be aware of it and deal with it appropriately.
References
- 1.Ho SY, Yeo CJ, Sebastin SJ, Tan TC, Lim AY. The flexor carpi radialisbrevis muscle - an anomaly in forearm musculature: A review article. Hand Surg 2011;16:245-9. [Google Scholar | PubMed]
- 2.Nagata J, Kojima Y, Satomura K, Ishiko T, Ajiki T. Anatomic variations of the flexor carpi radialis brevis: A report of five cases. J Hand Surg Asian Pac Vol 2016;21:113-5. [Google Scholar | PubMed]
- 3.Hosokawa T, Suto M, Tajika T, Chikuda H. Volar locking plate fixation of distal radius fracture with a flexor carpi radialis brevis and a hypoplastic pronator quadratus. J Orthop Case Rep 2019;9:11-4. [Google Scholar | PubMed]
- 4.Ninomiya H, Watanabe M, Kamimura K. Surgical exposure technique for volar locking plate fixation of distal radius fractures in patients with flexor carpi radialis brevis muscle anomaly. Case Rep Orthop 2021;2021:4512843. [Google Scholar | PubMed]
- 5.Hosokawa T, Tajika T, Suto M, Okano S, Chikuda H. Distal radius fractures with flexor carpi radialis brevis; case series. J Jpn Soc Surg Hand 2021;37:478-82. [Google Scholar | PubMed]
- 6.Mantovani G, Lino W Jr., Fukushima WY, Cho AB, Aita MA. Anomalous presentation of flexor carpi radialis brevis: A report of six cases. J Hand Surg Eur Vol 2010;35:234-5. [Google Scholar | PubMed]
- 7.Lee YM, Song SW, Sur YJ, Ahn CY. Flexor carpi radialis brevis: An unusual anomalous muscle of the wrist. Clin Orthop Surg 2014;6:361-4. [Google Scholar | PubMed]
- 8.Cheng BL, Yau EL, Yip NW. Prevalence of flexor carpi radialis brevis in Chinese patients with volar wrist plating performed for distal radius fracture. J Hand Surg Asian Pac Vol 2020;25:328-31. [Google Scholar | PubMed]
- 9.Carleton A. Flexor carpi radialis brevis vel profundus. J Anat 1935;69:292-3. [Google Scholar | PubMed]
- 10.Nakahashi T, Izumi R. Anomalous interconnection between flexor and extensor carpi radialis brevis tendons. Anat Rec 1987;218:94-7. [Google Scholar | PubMed]
- 11.Yoshida Y, Yasutaka S, Seki Y. Flexor radialis profundus and palmaris profundus muscles in man. Kaibogaku Zasshi 1983;58:59-67. [Google Scholar | PubMed]
- 12.Mimura T, Uchiyama S, Hayashi M, Uemura K, Moriya H, Kato H. Flexor carpi radialis brevis muscle: A case report and its prevalence in patients with carpal tunnel syndrome. J Orthop Sci 2017;22:1026-30. [Google Scholar | PubMed]
- 13.Akkoc RF, Aksu F, Emre E, Ogeturk M. The prevalence and distribution of the flexor carpi radialis brevis muscle in the Turkish population. Sci Rep 2022;12:416. [Google Scholar | PubMed]
- 14.Dodds SD. A flexor carpi radialis brevis muscle with an anomalous origin on the distal radius. J Hand Surg Am 2006;31:1507-10. [Google Scholar | PubMed]
- 15.Laugharne E, Power D. Surgical exposure of the distal radius in a patient with a flexor carpi radialis brevis muscle anomaly. J Surg Case Rep 2010;2010:1. [Google Scholar | PubMed]
- 16.Werntz RL, Hadeed AJ, Cappelleti GL, Orbay JL. Flexor carpi radialis brevis resection for treatment of a distal radius fracture: A case report. J Wrist Surg 2021;10:536-8. [Google Scholar | PubMed]
- 17.Wolfe SW, Pederson WC, Kozin SH, Cohen MS. Green‘s Operative Hand Surgery. 8th ed. Amsterdam: Elsevier; 2022. p. 639-53. [Google Scholar | PubMed]
- 18.Orbay JL, Touhami A. Current concepts in volar fixed-angle fixation of unstable distal radius fractures. Clin Orthop Relat Res 2006;445:58-67. [Google Scholar | PubMed]
- 19.Kosiyatrakul A, Luenam S, Prachaporn S. Symptomatic flexor carpi radialis brevis: Case report. J Hand Surg Am 2010;35:633-5. [Google Scholar | PubMed]
- 20.Kordahi AM, Sarrel KL, Shah SB, Chang EY. Flexor carpi radialis brevis: Case report of a symptomatic tear. Skeletal Radiol 2018;47:1705-8. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Nonvascularized Iliac Crest Autograft for Wrist and Hand Reconstructions: A Report of Two Clinical Cases and Literature Review
June 1, 2026 Nonvascularized Iliac Crest Autograft for Wrist and Hand Reconstructions: A Report of Two Clinical Cases and Literature Review March 1, 2026 An Economically Feasible Solution for Distal Radius Fractures Treated with Column-specific Fixation
March 1, 2026 An Economically Feasible Solution for Distal Radius Fractures Treated with Column-specific Fixation December 1, 2025 Functional and Radiological Outcomes Following Volar Locking Plate Fixation for Distal Radius Fractures: A Prospective Analytical Study
December 1, 2025 Functional and Radiological Outcomes Following Volar Locking Plate Fixation for Distal Radius Fractures: A Prospective Analytical Study November 1, 2025 The Use of a Tendon Protector Sheath for Prevention of First Extensor Compartment Tendon Adhesions after Radial Column Plating for Distal Radius Fracture: A Case Report
November 1, 2025 The Use of a Tendon Protector Sheath for Prevention of First Extensor Compartment Tendon Adhesions after Radial Column Plating for Distal Radius Fracture: A Case Report