
The management of extruded fracture dislocation of Talus is time-dependent and involves meticulous planning for favorable outcome.
Dr. S K Rai, Department of Orthopaedics, Military Hospital, Ambala, Haryana, India. E-mail: skrai47@yahoo.com
Abstract
Introduction: Extrusion of the talus with fracture dislocation is a very rare and devastating ankle injury usually caused by high-energy impact. There is no common consensus on the management for this type of injury. We intend to report on our experiences with its management and outcomes.
Case Report: We received a total of five cases of extruded fracture dislocation of the talus between March 2016 and April 2020. All fracture talus was Hawkins Type IV fracture. All five patients were male with an age range between 18 and 54 years and have sustained an injury in road traffic accidents. They were managed with wound debridement, talar preservation open reduction, and internal fixation with an application of an external fixator for wound care. All were followed up for 2 years.
Conclusion: Extruded fracture dislocation of the talus is a rare and devastating ankle injury. Its management is time-dependent and involves meticulous planning for a favorable outcome.
Keywords: Extruded fracture dislocation of talus, devastating ankle injury, open talus fracture dislocation, ankle injury.
Extrusion of the talus with fracture dislocation is a very rare and devastating ankle injury usually caused due to a high-energy impact. The actual incidence of these cases is still not known. However, extrusion of the talus constitutes approximately 0.06% of all dislocations and 2% of all talar injuries [1,2]. There are multiple methods described, dependent on time of presentation since injury and vascular status, immediate fixation or reimplantation of the talus, talar replacement, or tibiocalcaneal arthrodesis. In the present literature, appropriate treatment guidelines are still debatable and controversial. Few authors advocating reimplantation of the extruded talus despite the high chances of complications, such as post-operative infection, non-union of talus, avascular necrosis (AVN), osteoarthritis, and bone resorption. We did not find concrete evidence in the literature regarding talar reimplantation, which has high complication rates and difficult long-term outcome follow-up. In the current literature available, the data are scanty regarding its classification, management, and outcomes. The mechanism of injury is excessive plantar flexion of the tibiotalar combined with extreme supination or pronation.
Our index case no 3 and 5 (index case, we called because all relevant pictures has been shown in this manuscript, whereas only data were included for remaining patients) involves a 39-year-old male patient with no significant medical history, who was presented to the emergency department with polytrauma due to a road traffic accident. He reported an episode of transient loss of consciousness after the accident and indicated feeling pain throughout the body, particularly severe in the right ankle, upper back, and right shoulder. Physical evaluation revealed full consciousness, and alertness, with stable vitals and without any neurological deficits. Multiple abrasions and hematomas across the chest, shoulders, knees, and abdomen were noted. Over his left ankle, there was a 4 cm × 8 cm deep contaminated laceration wound over the anterolateral aspect of the ankle with oozing blood (Gustilo-Anderson grade 3B wound). Extruded talus was lying outside of the ankle mortise on the lateral aspect of the ankle with a few attached soft tissues. Distal pulsation was present, and no neurological deficit was detected clinically. The wound was washed with a copious amount of saline and broad-spectrum antibiotics were administered. The wound was covered with sterile gauze and a posterior slab was applied. Multiple radiologic studies were performed, which revealed fractures of the right 3, 4, and 5th ribs, minimal haemothorax on the right, no intracranial abnormalities, and subcutaneous swelling throughout the left upper abdomen and right chest. Left ankle radiographs revealed extruded fracture dislocation talus (Fig. 1).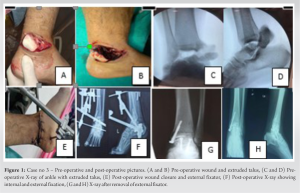 He was immediately admitted into surgery. Under spinal anesthesia debridement, relocation of the talus was performed, fixed with screws and K-wires along with an application of an external fixator for wound care (Fig. 1). The wound was loosely closed and was inspected every day. Intravenous antibiotics were administered based on the culture report for 2 weeks. The wound healed in 3 weeks and the external fixator was removed. Physiotherapy was performed thereafter, and the patient was discharged after 6 weeks. The patient was followed up at 6 months, 12 months, and finally at 2 years. On every visit X-ray, and CT scan was taken to record and monitor the talus fracture union and the range of ankle movement (Fig. 2).
He was immediately admitted into surgery. Under spinal anesthesia debridement, relocation of the talus was performed, fixed with screws and K-wires along with an application of an external fixator for wound care (Fig. 1). The wound was loosely closed and was inspected every day. Intravenous antibiotics were administered based on the culture report for 2 weeks. The wound healed in 3 weeks and the external fixator was removed. Physiotherapy was performed thereafter, and the patient was discharged after 6 weeks. The patient was followed up at 6 months, 12 months, and finally at 2 years. On every visit X-ray, and CT scan was taken to record and monitor the talus fracture union and the range of ankle movement (Fig. 2). Fifth patient (case no 5) of extrude talus was managed in similar way (Fig. 3).
Fifth patient (case no 5) of extrude talus was managed in similar way (Fig. 3). Our management algorithm is shown in Fig. 4.
Our management algorithm is shown in Fig. 4.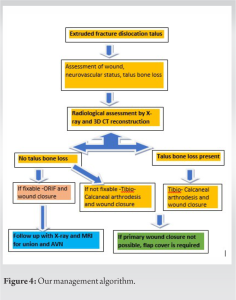 This algorithm may not be an ideal because management of this devastating injury depends on surgeon’s experience, availability of reconstruction surgeon, vascular surgeon, patient requirements, and availability of various orthopedics implants. The demographical characteristics of all five patients are shown in (Table 1).
This algorithm may not be an ideal because management of this devastating injury depends on surgeon’s experience, availability of reconstruction surgeon, vascular surgeon, patient requirements, and availability of various orthopedics implants. The demographical characteristics of all five patients are shown in (Table 1).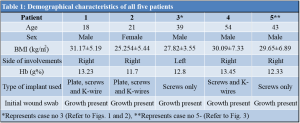 All cases were able to achieve a satisfactory range of motion at the ankle after 12 months of follow-up (Table 2).
All cases were able to achieve a satisfactory range of motion at the ankle after 12 months of follow-up (Table 2). Within 6–12 months, four cases achieved the union of fracture talus while case no 5 non-union. Two cases developed osteomyelitis. Painful subtalar joint was recorded in all cases (Table 3).
Within 6–12 months, four cases achieved the union of fracture talus while case no 5 non-union. Two cases developed osteomyelitis. Painful subtalar joint was recorded in all cases (Table 3).
We have presented a series of cases with extruded fracture dislocation of talus. A review of the literature revealed only a few reports of similar cases attributable to the uncommon nature of the ailment. Isolated closed talar extrusions are rare, and the injury is often associated with medial or lateral malleoli fractures [3]. Open total talus extrusion without associated fractures around the ankle is a rare injury. In the literature search, the largest published series include 18 and 27 ankles [4,5]. Many authors have reported a time-lapse of 30 min to 8 days between talar exposure and its reimplantation. They also noted that as this time increases, the possibility of wound infection, osteomyelitis, and AVN also increases [6,7,8,9]. It has been noted that the reimplantation that is performed under 3 h has shown a good prognosis but any time after 3 h may lead to a poor outcome. In the case of an injury that has not been treated for over 24 h, it is recommended to consider tibiocalcaneal arthrodesis. In a follow-up of 24 months, one patient developed an infection which was treated by repeated wound debridement and lavage and prolonged antibiotics, one patient developed chronic osteomyelitis of the distal tibia with prolonged discharging sinus which was managed by repeated joint lavage removal of implants and ankle joint arthrodesis. Join stiffness was seen in one patient with a planter and dorsi flexion was restricted by 10°. It has been observed that hypoplasia medial malleolar, ligament laxity around the ankle joint, peroneal muscle weakness, repeated ankle sprains, and less soft tissue around the ankle, put talus at the risk for its dislocation [10]. Various types of talar dislocations were described by Fahey and Murphy, that is, anterior, posterior, medial, lateral, upward, and the combination [11]. Mechanism dislocation of the talus was described by Leitner first stage: Dislocation of the subtalar joint, followed by talonavicular and finally total talar extrusion [12]. Anterior and posterior tibial vessels provided a major blood supply to the talus along with perforating peroneal vessels [13]. Complete talar dislocation puts the talus in an avascular state and subsequently leads to AVN. Management of complete talar extrusion is very challenging and complex too. There are no standard guidelines for the management of such a devastating injury in the literature. The literature review suggestions vary from primary talectomy to its reimplantation. In older days, immediate tibiocalcaneal arthrodesis was usually considered in place of reimplantation [14-17]. Smith and Nork have supported reimplantation of the talus even if there is a risk of collapse because it can be a useful bone stock for secondary procedures if required [5]. Gerken et al. [17] suggested that ANV can be delayed with immediate reimplantation and follow-up care. Open total talus extrusion is usually associated with fractures of either medial malleolus, lateral malleolus, or distal tibia fracture. These injuries are usually caused by high-energy impacts, like a motor vehicle accident and a fall from a height. Tibiotalar or subtalar dislocations may be associated with malleolar fractures until the talus is completely extruded laterally [8,12]. Weston et al. in a systemic review noted favorable outcomes with reimplantation and suggested this method as a first-line treatment [18]. Many authors noted good outcomes with immediate reduction and salvage of the extruded talus. [19-21]. The good outcome was may be due to revascularization of talus noted by AlMaeen et al. [20]. Complications such as infection and AVN are usually associated with such types of injury. It is noted that the talus is 60% covered with articular cartilage, without any muscle attachments, thus making the talus vulnerable to dislocation. Mohammad et al. [22] reported in their case report suggested that the prompt detection of extrusion of the talus is key and the outcome is time sensitive. Smrke et al. [23] in their case study on a 16-year-old man with totally extruded and lost talus, along with complex soft tissue injury around the ankle managed by microvascular foot reimplantation, microvascular muscle free flap transfer, temporary fixation, and later treated with tibio-calcaneal arthrodesis. Kasha and Yalamanchili [24] in their case report of talar extrusion with talar bone loss along with calcaneal fracture treated by masquelet technique in which he reconstructed the bony defect, debrided the wound, antibiotic bone cement was used as a spacer and the joints stabilized with K-wires and spanning external fixator was applied. A free flap cover was done to cover the defect and recorded a favorable outcome. Hichem et al. [25] recorded complete revascularization and satisfactory outcomes in a 30-year-old man after talus reimplantation following total talar extrusion. The key to a satisfactory outcome is thorough wound debridement and fixation. The patient should be explained the risks of long-term complications.
The present case series has few limitations firstly the short follow-up time of 2 years only where avascular necrosis of talus could not be assessed, secondly, the patients could not be recalled for follow-up after 2 years as they moved out or surgeon posted out from the hospital.
The management of extruded fracture dislocation of the talus poses great challenges for young orthopedic surgeons. Due to the lack of guidelines in the literature, its management and outcome depend on the availability of implants, and the expertise of the surgeon. Talus management is time-dependent and consists of thorough wound debridement, talar preservation, open reduction, and internal fixation with an external fixator for wound care. The multidisciplinary approach, which involves an orthopedic surgeon, plastic surgeon, radiologist, and sometimes vascular surgeon, is required for a satisfactory outcome.
The management of extruded fracture dislocation of talus is time sensitive. Its management consists of wound irrigation, thorough debridement, preservation of talus bone as much as possible, open reduction, and internal fixation with or without an external fixator for wound care. Patients should be well informed regarding the final outcome and associated complications.
References
- 1.Van Opstal N, Vandeputte G. Traumatic talus extrusion: Case reports and literature review. Acta Orthop Belg 2009;75:699-704. [Google Scholar | PubMed]
- 2.Kumar YC, Reddy S, Kumar Golla D, Ganesh N. Closed talar dislocation without associated fracture a very rare injury, a case report. J Orthop Case Rep 2014;4:10-2. [Google Scholar | PubMed]
- 3.Hammouda A, El Rayes M, El Kordy S. Posteromedial dislocation of the ankle without fracture. J Foot Ankle Surg 2006;12:169-71. [Google Scholar | PubMed]
- 4.Marsh JL, Saltzman CL, Iverson M, Shapiro DS. Major open injuries of the talus. J Orthop Trauma 1995;9:371-6. [Google Scholar | PubMed]
- 5.Smith CS, Nork SE, Sangeorzan BJ. The extruded talus: Results of reimplantation. J Bone Joint Surg Am 2006;88:2418-24. [Google Scholar | PubMed]
- 6.Montoli C, De Pietri M, Barbieri S, D’Angelo F. Total extrusion of the talus: A case report. J Foot Ankle Surg 2004;43:321-6. [Google Scholar | PubMed]
- 7.Palomo-Traver JM, Cruz-Renovell E, Granell-Beltran V, Monzonís-García J. Open total talus dislocation: Case report and review of the literature. J Orthop Trauma 1997;11:45-9. [Google Scholar | PubMed]
- 8.Hiraizumi Y, Hara T, Takahashi M, Mayehiyo S. Open total dislocation of the talus with extrusion (missing talus): Report of two cases. Foot Ankle 1992;13:473-7. [Google Scholar | PubMed]
- 9.Pradhan A, Najefi A, Patel A, Vris A, Heidari N, Malagelada F, Parker L, Jeyaseelan L. Complications after talus fractures: A trauma centre experience. Injury. 2023 Feb 1;54(2):772-7. [Google Scholar | PubMed]
- 10.Moehring HD, Tan RT, Marder RA, Lian G. Ankle dislocation. J Orthop Trauma 1994;8:167-72. [Google Scholar | PubMed]
- 11.Fahey JJ, Murphy JL. Dislocations and fractures of the talus. Surg Clin North Am 1965;45:79-102. [Google Scholar | PubMed]
- 12.Leitner B. The mechanism of total dislocation of the talus. J Bone Joint Surg Am 1955;37-A:89-95. [Google Scholar | PubMed]
- 13.Mulfinger GL, Trueta J. The blood supply of the talus. J Bone Joint Surg Br 1970;52:160-7. [Google Scholar | PubMed]
- 14.Dennis MD, Tullos HS. Blair tibiotalar arthrodesis for injuries to the talus. JBJS. 1980 Jan 1;62(1):103-7. [Google Scholar | PubMed]
- 15.Canale ST. Fractures of the neck of the talus. Orthopedics 1990;13:1105-15. [Google Scholar | PubMed]
- 16.Tezval M, Dumont C, Stürmer KM. Prognostic reliability of the Hawkins sign in fractures of the talus. J Orthop Trauma 2007;21:538-43. [Google Scholar | PubMed]
- 17.Gerken N, Yalamanchili R, Yalamanchili S, Penagaluru P, Milman EM, Cox G. Talar revascularization after a complete talar extrusion. J Orthop Trauma 2011;25:e107-10. [Google Scholar | PubMed]
- 18.Weston JT, Liu X, Wandtke ME, Liu J, Ebraheim NE. A systematic review of total dislocation of the talus. Orthop Surg 2015;7:97-101. [Google Scholar | PubMed]
- 19.Memisoglu K, Hürmeydan A. Total extrusion of the talus in an adolescent: A case report. J Am Podiatr Med Assoc 2009;99:431-4. [Google Scholar | PubMed]
- 20.AlMaeen BN, ElMaghrby IS, AlNour MK, Alrefeidi TA, Abu Adas SM. Complete Revascularization of Reimplanted Talus After Isolated Total Talar Extrusion: A Case Report. Cureus. 2020 May 3;12(5):e7947. [Google Scholar | PubMed]
- 21.Kwak, JM., Heo, SK. & Jung, GH. Six-year survival of reimplanted talus after isolated total talar extrusion: a case report. J Med Case Reports 11, 348 (2017). [Google Scholar | PubMed]
- 22.Mohammad HR, A’Court J, Pillai A. Extruded talus treated with reimplantation and primary tibiotalocalcaneal arthrodesis. Ann R Coll Surg Engl 2017;99:e115-7. [Google Scholar | PubMed]
- 23.Smrke DM, Rožman P, Gubina B, Frangež I, Smrke BR, Arnež ZM. An uncommon treatment of totally extruded and lost talus: A case report. J Med Case Rep 2014;8:322. [Google Scholar | PubMed]
- 24.Kasha S, Yalamanchili RK. The Masquelet technique in an extruded talus injury after open peri-talar dislocation- a case report. Trauma Case Rep 2021;36:100559. [Google Scholar | PubMed]
- 25.Hichem I, Mohammed-Reda F, Hatem A, Mahdi G, Ali M. Outcomes of a reimplanted talus after a total open extrusion. Cureus 2020;12:e9678. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Dual-Screw Fixation for Chronic Syndesmotic Injury: A Case Report
April 1, 2026 Dual-Screw Fixation for Chronic Syndesmotic Injury: A Case Report October 1, 2025 Management of Ipsilateral Tibia and Fibula Shaft Fracture with Trimalleolar Fracture: A Rare Case Report
October 1, 2025 Management of Ipsilateral Tibia and Fibula Shaft Fracture with Trimalleolar Fracture: A Rare Case Report January 1, 2025 Open Ankle Injury without Associated Fracture or Dislocation Requiring Surgical Intervention: A Case Report
January 1, 2025 Open Ankle Injury without Associated Fracture or Dislocation Requiring Surgical Intervention: A Case Report January 10, 2022 Adolescent-onset Local Kyphosis with Anterior Column Hypoplasia and Subluxation of the Facet Joints of the Lumbar Spine: A Case Report
January 10, 2022 Adolescent-onset Local Kyphosis with Anterior Column Hypoplasia and Subluxation of the Facet Joints of the Lumbar Spine: A Case Report