
Tibial tuberosity avulsion fractures with epiphyseal injury are prone to develop deformities later in the life; therefore, adequate and prompt diagnosis with good fixation is crucial to provide better clinical outcomes.
Dr. Adnan Anwer, Department of Orthopaedic Surgery, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh, Uttar Pradesh, India. E-mail: dr.adnan.amu@gmail.com
Abstract
Introduction: Acute avulsion of the tibial tubercle is an uncommon fracture, with reported incidence rates of 0.4–2.7% of all epiphyseal injuries and <1% of all physeal injuries. Typically, these fractures present with marked displacement of the entire proximal apophysis, with or without intra-articular extension, and variable associated soft-tissue injury. The Ogden classification has historically directed both non-operative and operative treatment of this injury. The overarching objective of several fracture fixation techniques has been outlined as being to restore the joint surface and the extensor mechanism.
Case Report: This case report describes the management of a 14-year-old male who sustained a rare avulsion fracture of the left tibial tuberosity with epiphyseal injury during a soccer game. The fracture was classified as Ogden Type III-B, indicating an intra-articular extension. The patient underwent open reduction and internal fixation with three cannulated screws and tension band wiring.
Conclusion: The fracture united with no residual deformity and return of full range of motion. Tension band wiring provides stable reduction; hence, prompt diagnosis and appropriate surgical intervention in similar cases is important to optimize outcomes.
Keywords: Tibial tuberosity, avulsion fracture, epiphyseal injury, open reduction, tension band wiring.
Avulsion fractures of the tibial tuberosity with associated epiphyseal injuries are rare but significant traumatic injuries, typically occurring in adolescents during high-energy activities such as sports. In the management of tibial plateau fractures, health-care professionals have at their disposal a range of treatment options. Non-operative methods often involve the application of a long leg cast in extension for a period of 6 weeks. This approach is typically recommended for type I injuries or those with minimal displacement (<2 mm) that maintain an acceptable alignment following closed reduction and cast application. Conversely, operative treatment options come into play for more complex cases. These may require open reduction, internal fixation, and sometimes arthrotomy or arthroscopy, along with soft-tissue repair. This surgical intervention is indicated for Type II to IV fractures, where the joint surface needs to be visualized for precise reduction, and evaluation for potential intra-articular pathology is crucial. Moreover, Type V fractures, specifically those involving a periosteal sleeve, often necessitate soft-tissue repair as part of the operative approach. The choice between non-operative and operative methods depends on the specific characteristics of the tibial plateau fracture and its associated complexities [1]. Ogden Type III-B fractures [2], characterized by intra-articular extension, are particularly challenging to manage. We present a case of a 14-year-old male who sustained an Ogden Type III-B avulsion fracture of the left tibial tuberosity with epiphyseal injury while playing soccer. The patient was managed with open reduction and internal fixation (ORIF) using three cannulated screws and tension band wiring. The purpose of this case report is to highlight this rare injury and prompt identification of the same.
A 14-year-old male presented to the emergency department with severe left knee pain and an inability to bear weight on the left lower limb following an injury sustained while playing soccer. The patient described a twisting mechanism during a tackle while trying to kick the football, resulting in immediate pain and swelling of the left knee. On physical examination, there was deformity, localized tenderness over the left tibial tuberosity, limited range of motion, and diffuse swelling.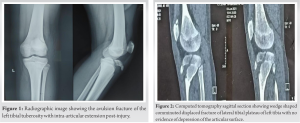
Radiographic evaluation, including anteroposterior and lateral knee views (Fig. 1) and a computed tomography scan (Fig. 2) of the knee, revealed an avulsion fracture of the left tibial tuberosity with intra-articular extension, consistent with an Ogden Type III injury.
Given the displacement of the fracture fragment and the intra-articular extension, surgical intervention was recommended [3]. The patient was taken to the operating room for open reduction and internal fixation under spinal anesthesia.
A standard anterior longitudinal incision was made over the left knee. Careful dissection was carried out to expose the fracture site. The fracture was reduced anatomically, and the reduction was maintained with provisional Kirschner wires.
Three 4.5 mm cannulated screws were inserted through the tibial tuberosity, securing it to the proximal tibia. A tension band wire was applied to enhance fixation stability (Fig. 3).
Post-operative care
Postoperatively, the patient was placed in a hinged knee brace with gradual physiotherapy and knee range of motion for 6 weeks. Weight-bearing was restricted for 8 weeks, after which a gradual return to full activity was allowed.

The patient had an uneventful recovery with no surgical site infection or any other complication. Serial radiographs demonstrated progressive fracture healing, and the patient regained full knee range of motion (Fig. 4), including a return to sports activities, 6 months post-surgery. On the follow-up X-rays, it was observed that the fracture had healed satisfactorily (Fig. 5). This was followed by implant removal 1 year postoperatively (Fig. 6).
Avulsion fractures of the tibial tuberosity with epiphyseal involvement, especially those classified as Ogden Type III-B fractures, pose a complex surgical dilemma due to their specific characteristics, notably the intra-articular extension. To ensure favorable outcomes and minimize the risk of enduring complications, such as growth disturbances, it is crucial to promptly diagnose these injuries and implement appropriate surgical strategies [4,5]. These injuries are easily missed if minimally displaced, and on the other hand, they can lead to recurvatum deformity if displaced [6].
Acute tibial tubercle avulsion fractures may be linked to further knee injuries, such as anterior cruciate ligament, medial collateral ligament, lateral collateral ligament, and meniscus injuries [7,8]. However, we did not encounter any such injuries in our case.
The aim of management of acute tibial tubercle avulsion fracture is restoration of the extensor mechanism and articular congruency of the tibial articular surface. This is accomplished by anatomically reducing the fracture fragment, avoiding any medial or lateral placement of the tuberosity fragment. A systematic review by Pretell-Mazzini et al. reported that up to 88% of cases of tibial tubercle fractures are candidates for surgery, with open reduction and internal fixation (ORIF) accounting for 98% of surgical correction [9]. Treatment with ORIF is recommended for tibial tubercle fractures of Types IIIA, B, and IV to restore congruency of the articular surface and address other intra-articular injuries, such as disruption of the extensor mechanism [10]. The surgical approach employed in this particular case involved open reduction and internal fixation, which proved to be an effective solution. This technique entailed the utilization of three cannulated screws, along with tension band wiring, to achieve stable fixation. We did tension band wiring to augment the fixation. Although no literature is available about the use of tension band wiring in these kinds of injuries, in our case, it proved to be a worthful intervention and helped in an early return to sports activities. The selection of this approach was likely influenced by several factors, including the fracture’s severity, the patient’s age, the patient’s keen interest in returning to sports activity as soon as possible, and the surgeon’s expertise.
The use of cannulated screws in the fixation process is advantageous because they can be accurately placed through small incisions, minimizing soft-tissue disruption. However, augmentation of fixation with tension band wire (TBW) converts the distracting forces into compression forces on the avulsed fragment, thereby promoting stability and consequently early physiotherapy and uncomplicated bone healing. Addition of TBW requires extension of incision. One of the noteworthy benefits of this surgical intervention is that it permits the early initiation of the rehabilitation process. Early rehabilitation is essential in such cases to prevent joint stiffness, muscle atrophy, and other complications associated with prolonged immobilization. It allows the patient to regain strength and function more rapidly, improving their overall quality of life during the recovery period. The successful recovery of the patient in this case underscores the critical importance of timely intervention, augmentation with tension band wiring, and adherence to postoperative rehabilitation protocols. Timely intervention ensures that the fracture is appropriately managed before it leads to long-term complications such as recurvatum deformity, growth disturbances, and limb length discrepancies, which can be especially concerning in younger patients with open growth plates.
Tibial tuberosity avulsion fractures with epiphyseal injuries are uncommon but can be severely disabling, particularly in teenagers playing high-impact sports. This case report underscores the importance of surgical intervention, specifically open reduction and internal fixation, to achieve anatomic reduction and stable fixation in Ogden Type III-B fractures. Tension band wiring for tibial tuberosity avulsion fractures has drawbacks such as invasiveness, hardware issues, non-union risk, limited versatility, complications, and additional cost concerns. Augmented fixation using cancellous screws and TBW is a novel concept which enhances the stability and thereby, early physiotherapy and uncomplicated bone healing, on the cost of extension of surgical incision. More studies will be indispensable to compare the augmented fixation using cancellous screws and TBW with the already existing techniques for a definitive opinion. Patient suitability and careful evaluation are essential. Proper post-operative care and rehabilitation are crucial for optimal outcomes.
This article summarizes the management of Ogden Type IIIB Tibial tuberosity fractures, their identification, diagnosis, and fracture fixation. Tension Band Wiring helps toward better fixation outcomes in such fractures by providing stability and enhanced bone healing.
References
- 1.Cole WW 3rd, Brown SM, Vopat B, Heard WM, Mulcahey MK. Epidemiology, diagnosis, and management of tibial tubercle avulsion fractures in adolescents. JBJS Rev 2020;8:e0186. [Google Scholar | PubMed]
- 2.Ogden JA, Tross RB, Murphy MJ. Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-15. [Google Scholar | PubMed]
- 3.Frey S, Hosalkar H, Cameron DB, Heath A, David Horn B, Ganley TJ. Tibial tuberosity fractures in adolescents. J Child Orthop 2008;2:469-74. [Google Scholar | PubMed]
- 4.Mansour AA, Mubarak SJ, Pennock AT. Tibial tuberosity fractures in adolescents: Is anatomic reduction necessary? J Pediatr Orthop 2016;36:642-7. [Google Scholar | PubMed]
- 5.Christie MJ, Dvonch VM. Tibial tuberosity avulsion fracture in adolescents. J Pediatr Orthop 1981;1:391-4. [Google Scholar | PubMed]
- 6.Franz P, Luderowski E, Tuca M. Tibial tubercle avulsion fractures in children. Curr Opin Pediatr 2020;32:86-92. [Google Scholar | PubMed]
- 7.Bolesta MJ, Fitch RD. Tibial tubercle avulsions. J Pediatr Orthop 1986;6:186-92. [Google Scholar | PubMed]
- 8.Shelton WR, Canale ST. Fractures of the tibia through the proximal tibial epiphyseal cartilage. J Bone Joint Surg Am 1979;61:167-73. [Google Scholar | PubMed]
- 9.Pretell-Mazzini J, Kelly DM, Sawyer JR, Esteban EM, Spence DD, Warner WC Jr., et al. Outcomes and complications of tibial tubercle fractures in pediatric patients: A systematic review of the literature. J Pediatr Orthop 2016;36:440-6. [Google Scholar | PubMed]
- 10.Mosier SM, Stanitski CL. Acute tibial tubercle avulsion fractures. J Pediatr Orthop 2004;24:181-4. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 11, 2014 Complete Traumatic Separation of Proximal Femoral Epiphysis in A 2 Year Old Child
July 11, 2014 Complete Traumatic Separation of Proximal Femoral Epiphysis in A 2 Year Old Child October 1, 2025 A Missed Case of Langerhans Cell Histiocytosis of the Proximal Femur after Total Hip Arthroplasty in an Adult: A Case Report
October 1, 2025 A Missed Case of Langerhans Cell Histiocytosis of the Proximal Femur after Total Hip Arthroplasty in an Adult: A Case Report July 1, 2025 An Observational Study on Pre-natal Diagnosis of Congenital Talipes Equinovarus
July 1, 2025 An Observational Study on Pre-natal Diagnosis of Congenital Talipes Equinovarus June 10, 2023 A Rare Case of Exostosis of the Medial Sesamoid Bone
June 10, 2023 A Rare Case of Exostosis of the Medial Sesamoid Bone