
In this report, we present a new type of double-layered meniscus that has not been described in the literature before.
Dr. Ethem Burak Oklaz, Department of Orthopaedics and Traumatology, Gazi University Faculty of Medicine, Ankara, Turkey. E-mail: burakoklaz@gmail.com
Abstract
Introduction: Abnormalities of the double-layered meniscus are rare and can be difficult to diagnose. The main pathology in this abnormality, which is predominantly seen in the lateral compartment, is an accessory meniscus lying over the normal meniscus. Anatomically, this structure can appear in different forms. Although other meniscal abnormalities associated with a double-layered meniscus have been reported, this case presents a previously undescribed type in the literature.
Case Report: A 12-year-old girl presented to our clinic with complaints of knee locking and pain. When the patient underwent arthroscopy, an accessory incomplete discoid meniscus was found overlying the normal lateral meniscus. We performed an excision of the upper accessory meniscus and the patient had no problems during 3 years of follow-up after surgery.
Conclusion: Abnormalities of the lateral meniscus are rare and can be difficult to diagnose. In cases where we suspect a meniscal abnormality, a proper arthroscopic examination should be performed and if a discoid meniscus is seen, it should be considered that this may be a double-layered meniscus.
Keywords: Double-layered meniscus, discoid meniscus, lateral meniscus abnormalities, knee arthroscopy.
Abnormalities of the meniscus are rare in the general population and tend to occur in the lateral meniscus [1]. They can cause a range of symptoms such as pain, swelling, and locking due to changes in the structure of the knee joint. Several types of meniscal abnormalities can present in the knee joint, including the most common form, discoid meniscus, as well as less common forms such as ring-shaped meniscus, Wrisberg meniscus, and double-layered meniscus [1,2]. A review of the literature has shown that only a small number of cases of double-layered meniscus have been documented [3]. In this report, we present a new type of double-layered meniscus that has not been described in the literature before. The patient and her family were informed that data concerning their case would be submitted for publication and they provided consent.
A 12-year-old girl complained of knee pain and clicking that had persisted for 3 months without trauma. Physical examination of the patient revealed limited extension (range of motion is 20°–135°) and a positive McMurray test on the lateral side. An enlarged lateral joint space with high signal intensity in the region of the lateral meniscus was observed on magnetic resonance imaging (MRI) (Fig. 1).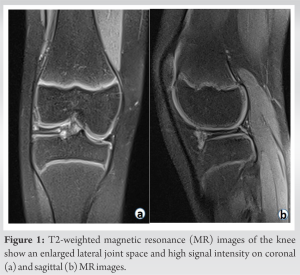 On arthroscopic visualization of the knee joint, the first structure observed was an incomplete discoid meniscus with inflammation and central vascularization (Fig. 2a). When the central part of this structure was excised, an accessory meniscus was observed overlying the normal lateral meniscus (Fig. 2b).
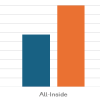
On arthroscopic visualization of the knee joint, the first structure observed was an incomplete discoid meniscus with inflammation and central vascularization (Fig. 2a). When the central part of this structure was excised, an accessory meniscus was observed overlying the normal lateral meniscus (Fig. 2b).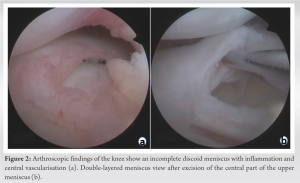 While the posterior part of the accessory meniscus was connected to the underlying normal meniscus, there was no connection between these two structures in the periphery (Fig. 3). While the thickness of the upper incomplete discoid meniscus was similar to that of the normal meniscus, its mobility was higher. Initially, the central part of the incomplete discoid meniscus was removed, resulting in the classic appearance of a double-layered meniscus and then the upper accessory meniscus was removed (Fig. 4).
While the posterior part of the accessory meniscus was connected to the underlying normal meniscus, there was no connection between these two structures in the periphery (Fig. 3). While the thickness of the upper incomplete discoid meniscus was similar to that of the normal meniscus, its mobility was higher. Initially, the central part of the incomplete discoid meniscus was removed, resulting in the classic appearance of a double-layered meniscus and then the upper accessory meniscus was removed (Fig. 4).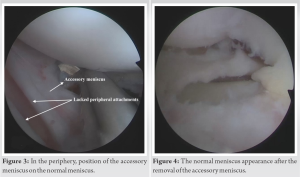
After surgery, the patient’s pain was completely gone by the end of the 1st month and the full range of motion was achieved at the end of the 6th week. Our patient performed post-operative physiotherapy compatibly and was allowed to do active sports at the end of the 3rd month. The annual follow-ups were carried out, and the patient’s 3-year follow-up showed no occurrence of any complications. At the end of the 3rd year, the International Knee Documentation Committee (IKDC) score was 95.
Since its first description by Bailey and Blundel in 1974, the presence of a double-layered lateral meniscus has only been reported in 15 cases in the literature [3,4]. An anatomical study of 437 patients to investigate meniscal abnormalities reported a prevalence rate of 0.5% for a double-layered lateral meniscus [1]. However, in arthroscopic studies involving a larger number of patients, the prevalence rate ranges from 0.06% to 0.09% [5,6]. Meniscal abnormalities typically present with symptoms such as knee pain, locking, and restricted range of motion. MRI and diagnostic arthroscopy can be used to make a differential diagnosis [7]. Because the MRI appearance of a double-layered meniscus is similar to bucket-handle tears and horizontal meniscal tears, it can be difficult to make a definitive diagnosis based on imaging alone [8]. Therefore, in most cases, a definitive diagnosis is made through arthroscopic examination. In our case, there were findings supporting this view. On examination of the MRI images in our case, a preliminary diagnosis of a horizontal tear accompanying the discoid meniscus could be considered. However, the arthroscopic examination revealed that it was a double-layered meniscus, not a tear. This distinction was made thanks to two important findings. First, the upper meniscus was in an incomplete discoid structure, whereas the lower meniscus was in a normal shape. Second, the posterior part of the accessory meniscus was found to be attached to the normal meniscus, whereas peripheral part lacked any attachment. This observation is compatible with the separated type double-layered meniscus pattern previously reported in the literature [8,9]. Although incomplete discoid meniscus is one of the most commonly observed morphological variations, there is limited information in the literature regarding its association with other meniscal abnormalities. The only information available on the relationship between discoid meniscus and double-layered meniscus is a case report by Saygi et al., in which incidentally observed a structure resembling a discoid meniscus beneath the normal meniscus during examination of the lateral meniscus in a patient who underwent surgery for medial meniscus pathology [10]. In our case, the patient presented with lateral meniscus symptoms and an incomplete discoid meniscus was observed lying the normal lateral meniscus.
We recommend arthroscopy for accurate diagnosis and treatment of lateral meniscus pathology when MRI cannot provide a definitive diagnosis. As this case shows, it is important to be aware of the possibility of rare conditions and to perform a thorough examination during arthroscopy to accurately diagnose abnormalities.
The presence of a double-layered meniscus with an incomplete discoid accessory meniscus, reported for the first time in this case, is a notable abnormality that should be considered in cases of suspected meniscal abnormalities.
References
- 1.Ryu K, Iriuchishima T, Oshida M, Saito A, Kato Y, Tokuhashi Y, et al. Evaluation of the morphological variations of the meniscus: A cadaver study. Knee Surgery, Sport Traumatol Arthrosc 2015;23:15-9. [Google Scholar | PubMed]
- 2.Kim YG, Ihn JC, Park SK, Kyung HS. An arthroscopic analysis of lateral meniscal variants and a comparison with MRI findings. Knee surgery, sports traumatology, arthroscopy . Knee Surg Sports Traumatol Arthrosc 2006;14:20-6. [Google Scholar | PubMed]
- 3.Ota M, Takagi H, Kato S, Kawashima F, Kanzaki K. Surgical treatment of double-layered lateral meniscus. Case Rep Orthop 2021;2021:9978889. [Google Scholar | PubMed]
- 4.Bailey WH, Tge B. An unusual abnormality affecting both knee joints in a child. J Bone Jt Surg Am 1974;56:814-6. [Google Scholar | PubMed]
- 5.Suzuki S, Mita F, Ogishima H. Double-layered lateral meniscus: A newly found anomaly. Arthrosc J Arthrosc Relat Surg 1991;7:267-71. [Google Scholar | PubMed]
- 6.Okahashi K, Sugimoto K, Iwai M, Oshima M, Fujisawa Y, Takakura Y. Double-layered lateral meniscus. J Orthop Sci 2005;10:661-4. [Google Scholar | PubMed]
- 7.Saavedra M, Sepúlveda M, Tuca MJ, Birrer E. Discoid meniscus: Current concepts. EFORT Open Rev 2020;5:371-9. [Google Scholar | PubMed]
- 8.Ahn TY, Kim HT, Park YG. Double-layered lateral meniscus including a ring-shaped accessory meniscus: A case report. JBJS Case Connect 2018;8:e104. [Google Scholar | PubMed]
- 9.Fukuda A, Nishimura A, Nakazora S, Kato K, Sudo A. Double-layered lateral meniscus accompanied by meniscocapsular separation. Case Rep Orthop 2015;2015:357463. [Google Scholar | PubMed]
- 10.Saygi B, Yildirim Y, Senturk S, Sezgin Ramadan S, Gundes H. Accessory lateral discoid meniscus. Knee Surg Sport Traumatol Arthrosc 2006;14:1278-80. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 All-Inside Versus Inside-Out Meniscal Repair: A Comparative Study of Healing Rates And Functional Outcomes
July 1, 2026 All-Inside Versus Inside-Out Meniscal Repair: A Comparative Study of Healing Rates And Functional Outcomes June 1, 2026 Creatine Supplementation in Pediatric Orthopedic Rehabilitation: A Translational Review and Proposed Clinical Trial Framework
June 1, 2026 Creatine Supplementation in Pediatric Orthopedic Rehabilitation: A Translational Review and Proposed Clinical Trial Framework May 1, 2026 Optimizing Post-operative Pain Management in Knee Arthroscopy: A Double-Blinded Randomized Controlled Trial of Regional Anesthesia with and without Local Infiltration
May 1, 2026 Optimizing Post-operative Pain Management in Knee Arthroscopy: A Double-Blinded Randomized Controlled Trial of Regional Anesthesia with and without Local Infiltration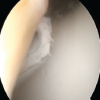 February 1, 2026 Knee Arthroscopy in Morbidly Obese Patients: Perioperative Challenges and Technical Considerations to Optimize Outcomes
February 1, 2026 Knee Arthroscopy in Morbidly Obese Patients: Perioperative Challenges and Technical Considerations to Optimize Outcomes