
Endoscopic repair of the hip abductor tendon is a safe and minimally invasive surgical technique indicated for treating chronic full-thickness abductor tendon recalcitrant to conservative management.
Dr. Gabriella Bucci, LSU Health Family Medicine Residency Program, Shreveport, LA, USA. E-mail: gabriellabuccimd@outlook.com
Abstract
Introduction: Greater trochanteric pain syndrome is a common incapacitating hip condition characterized by chronic lateral hip pain. This condition includes a range of pathologies ranging from trochanteric bursitis, hip abductor pathology involving the gluteus medius and minimum, external coxa saltans (snapping hip syndrome), or combinations of these. Hip abductor tendon tears have gained recognition as a main contributor to this condition. This pathology is often misdiagnosed and left untreated because of the frequency of partial-thickness undersurface tears. Once this challenging diagnosis is confirmed, non-operative treatments are considered the first therapeutic approach. Despite the availability and effectiveness of multiple non-operative therapies, a considerable percentage of patients will present with chronic disabling pain and refractory symptoms. Many health-care providers are unaware of accessible advanced surgical techniques that benefit patients unresponsive to conservative management.
Case Report: We present the case of a 51-year-old female patient with chronic lateral hip pain refractory to conservative treatment for more than two years, treated successfully with endoscopic abductor tendon repair. The patient returned to the desired activities six months following surgery without any reported complications. Patient’s pre-operative reported outcomes utilizing the MHOT-14 and Vail hip scores improved from 27 to 79 points (on a scale of 0-100) and from 30 to 56 points (on a scale of 0-–100), respectively, at eight months follow-up.
Conclusion: This case report is illustrative of endoscopic surgical repair of the hip abductor tendons in the setting of a chronic full-thickness abductor tendon tear in a female patient after failure of conservative management. The multiple advantages of the technique include performance in an ambulatory day surgery center, soft-tissue preservation, and fewer complications compared to other open techniques. Knowledge of this pathology and its state-of-the-art available treatments is relevant for orthopedic surgeons and a wide range of health providers who encounter patients with chronic lateral hip pain.
Keywords: Greater trochanteric pain syndrome, lateral hip pain, gluteus medius tendon, gluteus minimus tendon, hip abductor tendon tear, endoscopic repair.
Greater trochanteric pain syndrome (GTPS) which is defined as chronic pain in the lateral area of the hip has an estimated frequency of 1.8–5.6/1000 patients [1]. Previously this lateral hip pain has been attributed to trochanteric bursitis, external coxa saltans (snapping hip syndrome), or combinations of these, however, recent studies propose the etiology is more closely tied to gluteus medius and minimus tendon tears [2-4]. These injuries generally result from a chronic, degenerative process that may be classified as either spontaneous or traumatic[[5]. Because of the frequency of partial-thickness undersurface tears, this pathology is often misdiagnosed and left untreated. Abductor tendon tears occur 4 times more frequently in women than in men, with incidence peaking between the fifth and seventh decades [4]. This prevalence has been attributed to increased abductor tendon forces required to stabilize the female pelvis, differences in hormones, and activity patterns [6]. Diagnosis is made by a thorough history and physical examination, and confirmed with diagnostic imaging, including X-ray and MRI [1,4,7]. Once this challenging diagnosis is confirmed, non-operative treatments are considered the first therapeutic approach and have shown to be highly effective, with curative rates of more than 90% [8,9]. Conservative measures include activity modification, weight loss, heat/cold therapy, physical therapy (PT), and pharmacologic treatment, including, non-steroidal anti-inflammatory medications (NSAIDs), simple non-opioid analgesics, such as paracetamol, which may be preferred in this age group of patients avoiding NSAIDs, dermal anesthetic patches and adjuvant medication such as antidepressants, injections with corticosteroid and local anesthetics, shockwave therapy and injections with platelet-rich-plasma (PRP) [8,9,10]. These treatments can be used in an individual or multimodal phase, depending on the severity of the patient’s symptoms, availability, and patient-physician preferences [8,10]. However, conservative measures may require lengthy periods of treatments, and multiple cycles of therapy, and patients may experience only partial relief or recurring symptoms [8,10]. For recalcitrant cases, surgical treatment is indicated and either open or endoscopic repair techniques have demonstrated significant clinical benefits exceeding the minimal clinically important difference (MCID) at more than 2 years of follow-up. This manuscript describes a severe refractory case of GTPS in a female patient treated with endoscopic abductor tendon repair, reporting the patient’s outcomes utilizing MHOT-14 and Vail Hip scores after a short-term follow-up, without any reported complications.
A 51-year-old female with a past medical history of seronegative rheumatoid arthritis and on-demand treatment with NSAIDs was evaluated for lateral hip pain irradiated to the posterior hip for more than two years, which limited her recreational sports and activities for daily living. The pain was refractory to conservative treatment, including one year of physical therapy, three trochanteric bursa steroid injections, and one bone marrow aspiration injection by previous physicians. All injections were separated by three months and performed under fluoroscopy guidance. Physical examination was positive for Trendelenburg gait, tenderness over the greater trochanter, FABER maneuver, and abductor complex weakness with resisted hip abduction. Radiological images demonstrate moderate degenerative changes of the right hip joint with Tönnis grade 2 and greater trochanter enthesopathy (Fig. 1). 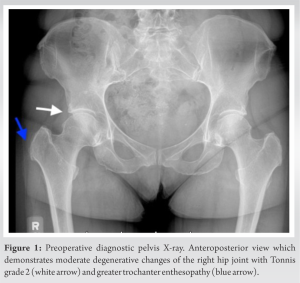 MRI demonstrated a complete, chronic full-thickness gluteus medius tendon tear with mild retraction, chronic enthesopathy with osteophyte formation at the abductor insertion with associated bursitis (Fig. 2a and b). Given the failure of conservative management and duration of hip pain, indication of surgical treatment with endoscopic gluteus medius repair was indicated.
MRI demonstrated a complete, chronic full-thickness gluteus medius tendon tear with mild retraction, chronic enthesopathy with osteophyte formation at the abductor insertion with associated bursitis (Fig. 2a and b). Given the failure of conservative management and duration of hip pain, indication of surgical treatment with endoscopic gluteus medius repair was indicated.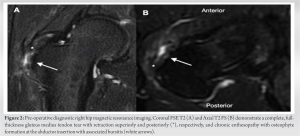
The surgery was performed by the senior author. After adequate induction of general anesthesia, the patient was placed in a supine position on a hip arthroscopy minimal-post table after properly protecting the pressure areas. drape, and pre-operative IV antibiotics were given. No hip distraction was applied, and the hip was placed in 15 degrees of abduction to relieve gluteal tension (Fig. 3). Under fluoroscopic guidance, a spinal needle was used to localize the peritrochanteric anterolateral portal, and a 70 degrees lens was established deep to the iliotibial band (ITB), and adjacent to the insertion of the abductor tendon which was confirmed by rotation of the limb. Next an incision overlying the most anterior aspect of the insertion was made and correspondent instruments were guided into the deep peritrochanteric space. Next, the posterolateral (PL) portal was placed under direct visualization followed by placement of the distal anterior lateral accessory (DALA) portal.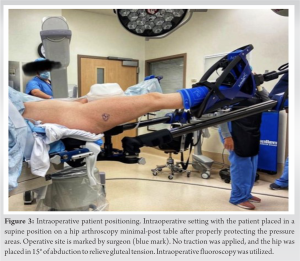 The ITB was not released during the procedure. Within the medial peritrochanteric space the bursal side of the abductor tendon insertion on the greater trochanter was visualized, demonstrating significant amount of scarring and hyperemia within the abductor tendon complex itself. A thickened hypertrophic bursa was visualized and treated with bursectomy utilizing radiofrequency and shaver (Fig. 4a). Complete bursectomy was performed until an adequate visualization of the gluteus maximus insertion was identified distally, its undersurface proximally, the longitudinal fibers of the vastus lateralis medially, and the ITB laterally. The abductor tendon insertion site on the femur was visualized arthroscopically and confirmed under fluoroscopic guidance. A pathologic osteophyte formation distal to the chronically hyperemic degenerative and torn abductor tendon insertion was identified. A probe was used to palpate the surface of the abductor’s tendon to detect areas of occult fiber disruption, identifying a full-thickness tear of the gluteus medius. The degenerative tissue around the tear was debrided using a shaver. No signs of intratendinous steroid injections were observed. Then, the insertional footprint itself was prepared with a shaver in burr mode to create a bleeding surface to improve tendon-bone healing (Fig. 4b).
The ITB was not released during the procedure. Within the medial peritrochanteric space the bursal side of the abductor tendon insertion on the greater trochanter was visualized, demonstrating significant amount of scarring and hyperemia within the abductor tendon complex itself. A thickened hypertrophic bursa was visualized and treated with bursectomy utilizing radiofrequency and shaver (Fig. 4a). Complete bursectomy was performed until an adequate visualization of the gluteus maximus insertion was identified distally, its undersurface proximally, the longitudinal fibers of the vastus lateralis medially, and the ITB laterally. The abductor tendon insertion site on the femur was visualized arthroscopically and confirmed under fluoroscopic guidance. A pathologic osteophyte formation distal to the chronically hyperemic degenerative and torn abductor tendon insertion was identified. A probe was used to palpate the surface of the abductor’s tendon to detect areas of occult fiber disruption, identifying a full-thickness tear of the gluteus medius. The degenerative tissue around the tear was debrided using a shaver. No signs of intratendinous steroid injections were observed. Then, the insertional footprint itself was prepared with a shaver in burr mode to create a bleeding surface to improve tendon-bone healing (Fig. 4b).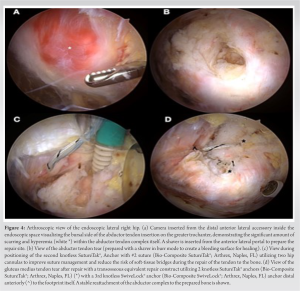 Next a transosseous equivalent repair construct utilizing 2 knotless SutureTak® Anchor with #2 suture (Bio-Composite SutureTak®; Arthrex, Naples, FL) was created for repair of the tendon to bone with a 3rd knotless SwiveLock® anchor (Bio-Composite SwiveLock®; Arthrex, Naples, FL) distal anteriorly to the footprint itself (Fig. 4c). A stable reattachment of the abductor complex to the prepared bone was visualized during rotatory examination (Fig. 4d). Local anesthetic (2cc Marcaine 0.5%) was placed within the wound at the repair site, the skin was closed sterilely, and a sterile dressing was applied.
Next a transosseous equivalent repair construct utilizing 2 knotless SutureTak® Anchor with #2 suture (Bio-Composite SutureTak®; Arthrex, Naples, FL) was created for repair of the tendon to bone with a 3rd knotless SwiveLock® anchor (Bio-Composite SwiveLock®; Arthrex, Naples, FL) distal anteriorly to the footprint itself (Fig. 4c). A stable reattachment of the abductor complex to the prepared bone was visualized during rotatory examination (Fig. 4d). Local anesthetic (2cc Marcaine 0.5%) was placed within the wound at the repair site, the skin was closed sterilely, and a sterile dressing was applied.
Post-operative evaluation
Patients are evaluated by the treating orthopedic surgeon at 1-day, 2-weeks, 6-weeks, 3- months’ post-operative, and as needed until clearance for a return to desired activities. Patient’s pre-operative reported outcomes utilizing the MHOT-14 and Vail Hip scores improved from 27 to 79 points (on a scale of 0–100) and from 30 to 56 points (on a scale of 0–100), respectively, at eight months follow-up. The patient returned to the desired activities six months following surgery without any reported complications. Follow-up images are not part of the routine post-operative care at the clinic, unless the patient complains of pain or a traumatic injury occurs.
Rehabilitation protocol
The patient followed a three phases rehabilitation protocol focused on patients with baseline dysfunctions documented pre-operatively as degenerative tendinopathy or tears in older, more sedentary patients.
Phase 1: Protected Mobility (post-operative day 0–week 6 post-operative).
Goal: Maintain mobility to reduce medical comorbidity and preserve hip/spine function without stressing tendon-to-bone repair during the early healing phase.
- The patient was instructed to use a walker with partial flat-foot-weight-bearing and fitted for the T scope post-operative hip abduction brace (©2019 Breg, Inc.) limiting adduction and flexion to 90 degrees Brace at all times with 0-90 degrees.
- Daily position changes (no sit/ stand/ walk longer than 30 continuous minutes).
- Foot/calf activations; glut max isometric; abdominal isometric.
Phase 2: Unassisted activities of daily living (ADL) (post-operative week 6–8).
Goal: Engage isometric function of abductor/ITB; Increase stance-phase independence of operative limb and restore normal gait.
- Week 6–7: discontinue walker and use a brace with a cane in the opposite hand.
- Week 7–8: discontinue brace and use a cane in the opposite hand.
Phase 3: Endurance (post-operative week 8–3 months).
Goal: Increase gait and ADL-related repair site endurance and reduce myofascial pain.
- Aqua walking; Manual myofascial techniques avoiding extremes of passive ADDUCTION/IR/ER.
- Supine, foot on the ground core; Gentle isokinetic abductor.
Standing core/balance isometrics.
GTPS is a term used to characterize multiple disorders about the proximal, lateral hip area. [1,10] Often these disorders involve problems within the peritrochanteric anatomic area of the proximal femur. The most frequently seen disorders are trochanteric bursitis, hip abductor pathology involving the gluteus medius, external coxa saltans (snapping hip syndrome), or combinations of these [1,4,7]. Pain is a common complaint. Proper diagnosis requires the following: An awareness of the potential causes of pain, performing an appropriate history and physical examination, appreciating findings on radiographs and MRI [1,10]. Despite the availability and effectiveness of multiple non-operative therapies, a considerable percentage of patients will present with chronic disabling pain and refractory symptoms [8,9]. Many health-care providers are unaware of accessible advanced surgical techniques that have proven to benefit patients unresponsive to conservative management [3,11,12]. Endoscopic abductor tendon repair is a recently developed minimally invasive technique that has been shown to provide significant improvement in patients reported outcomes (PROs) and substantial clinical benefits (SCB) [6,11,12]. Multiple investigators have demonstrated results equivalent to open repair techniques that exceed minimal clinically important difference (MCID) and patient-acceptable symptomatic state (PASS) [6,11,12]. Advancements in arthroscopic techniques and reliable repair constructs have made this surgical technique a viable treatment option for patients with symptomatic abductor tendon tears who fail conservative management. The advantages of performing an endoscopic approach for these injuries include (1) a decreased risk of altering patient’s gait, (2) less post-operative pain by preserving the ITB and gluteus maximus, (3) less cost associated with performance in the outpatient surgical setting and (4) decreased risk of complications when compared to open repairs. Two recent reports in the literature emphasize the benefits of the arthroscopic surgical technique to the repair of gluteus medius tears in the short-term [6,11,12]. Nazal et al. conducted a prospective study of 15 hips with full-thickness gluteus medius and minimus tears that underwent arthroscopic repair with transosseous equivalent repair and a double-row technique using suture anchors. At 24 months follow-up, 100% reported satisfaction and would undergo the same procedure again. The mean of differences between pre-operative and 24-month post-operative follow-up PROs, was statistically significant for every score measured and most patients exceeded the MCID thresholds for the modified Harris Hip score: 86.67% (P<0.001), hip outcome scored ADL: 86.67% (P=0.0047), hip outcome scored SSS: 66.67% (P=0.01), Non-arthritic Hip Scale: 93.33% (P<0.001), and International Hip Outcome Tool-33: 80% (P<0.001). No complications were noted [11]. Similarly, Kirby et al. conducted a study of 20 hips divided into two groups of patients with either partial or full-thickness gluteus medius tears, treated with endoscopic knotless repair in an inverted horizontal mattress configuration. At an average follow-up of 28 months, both groups presented statistically significant improvements in PROs without differences between tear types. The average pre-operative NAHS and mHHS scores improved 35.3 and 38.1 points, respectively, at 2 years postoperatively (P <001) [12]. This study has similar favorable results as other endoscopic repair studies [11,12,13]. The MCID is defined as the minimal change in outcome that the patient is able to appreciate, in contrast the SCB is considered the improvement in outcome that the patient considers a substantial amelioration. The current case report demonstrates improvement in both, MHOT-14 and Vail Hip score, exceeding the values associated with previously established MCID and SCB [13]. This manuscript adds to the growing body of literature that endoscopic abductor tendon repair is a safe procedure with good patient-reported outcomes and low risk of complication.
This case report is illustrative of endoscopic surgical repair of the hip abductor tendons in the setting of a chronic full-thickness abductor tendon tear in a female patient after failure of conservative management, reporting improvement in PROs without short-term complications. The multiple advantages of the technique include, performance in an ambulatory day surgery center, soft-tissue preservation, and fewer complications when compared to other open techniques. Knowledge of this pathology and its state-of-the-art available treatments is relevant for orthopedic surgeons and a wide range of health-care providers who encounter patients with chronic lateral hip pain.
Abductor tendon tears represent a challenging diagnosis for all health-care providers when treating patients with lateral hip pain. Although representing the gold standard first-line approach, conservative measures may require long periods of treatments, multiple cycles of therapy, and patients may experience only partial relief or recurring symptoms. For recalcitrant cases, surgical treatment is indicated. This article describes a safe and minimally invasive endoscopic repair technique indicated for treating a chronic full-thickness abductor tendon in a female patient after failure of conservative management, without reported complications at short-term follow-up.
References
- 1.Williams BS, Cohen SP. Greater trochanteric pain syndrome: A review of anatomy, diagnosis and treatment. Anesth Analg 2009;108:1662-70. [Google Scholar | PubMed]
- 2.Domb BG, Nasser RM, Botser IB. Partial-thickness tears of the gluteus medius: Rationale and technique for trans-tendinous endoscopic repair. Arthroscopy 2010;26:1697-705. [Google Scholar | PubMed]
- 3.Chandrasekaran S, Lodhia P, Gui C, Vemula SP, Martin TJ, Domb BG. Outcomes of open versus endoscopic repair of abductor muscle tears of the hip: A systematic review. Arthroscopy 2015;31:2057- 67.e2. [Google Scholar | PubMed]
- 4.Silva F, Adams T, Feinstein J, Arroyo RA. Trochanteric bursitis: Refuting the myth of inflammation. J Clin Rheumatol 2008;14:82-6. [Google Scholar | PubMed]
- 5.Gordon EJ. Trochanteric bursitis and tendinitis. Clin Orthop 1961;20:193-202. [Google Scholar | PubMed]
- 6.Hartigan DE, Perets I, Ho SW, Walsh JP, Yuen LC, Domb BG. Endoscopic repair of partial-thickness undersurface tears of the abductor tendon: Clinical outcomes with minimum 2-year follow-up. Arthroscopy 2018;34:1193-9. [Google Scholar | PubMed]
- 7.Lequesne M. From “periarthritis” to hip “rotator cuff” tears. Trochanteric tendinobursitis. Joint Bone Spine 2006;73:344-8. [Google Scholar | PubMed]
- 8.Barratt PA, Brookes N, Newson A. Conservative treatments for greater trochanteric pain syndrome: A systematic review. Br J Sports Med 2017;51:97-104. [Google Scholar | PubMed]
- 9.Lustenberger DP, Ng VY, Best TM, Ellis TJ. Efficacy of treatment of trochanteric bursitis: A systematic review. Clin J Sport Med 2011;21:447-53. [Google Scholar | PubMed]
- 10.Torres A, Fernández-Fairen M, Sueiro-Fernández J. Greater trochanteric pain syndrome and gluteus medius and minimus tendinosis: Nonsurgical treatment. Pain Manag 2018;8:45-55. [Google Scholar | PubMed]
- 11.Nazal MR, Abraham PF, Conaway WK, Quinlan NJ, Gillinov SM, Gibbs JS, et al. Endoscopic repair of full-thickness gluteus medius and minimus tears-prospective study with a minimum 2-year follow-up. Arthroscopy 2020;36:2160-9. [Google Scholar | PubMed]
- 12.Kirby D, Fried JW, Bloom DA, Buchalter D, Youm T. Clinical outcomes after endoscopic repair of gluteus medius tendon tear using a knotless technique with a 2-year minimum follow-up. Arthroscopy 2020;36:2849-55. [Google Scholar | PubMed]
- 13.Martin RL, Kivlan BR, Christoforetti JJ, Wolff AB, Nho SJ, Salvo JP Jr., et al. Minimal clinically important difference and substantial clinical benefit values for the 12-item international hip outcome tool. Arthroscopy 2019;35:411-6. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 December 10, 2021 Anterior Column and Anterior Dome Marginal Impaction Acetabular Fracture Treated with a Modified Smith-Petersen Approach along with Anterior Superior Iliac Spine Osteotomy using the Two-level Reconstruction Technique
December 10, 2021 Anterior Column and Anterior Dome Marginal Impaction Acetabular Fracture Treated with a Modified Smith-Petersen Approach along with Anterior Superior Iliac Spine Osteotomy using the Two-level Reconstruction Technique June 10, 2024 Multiple Vertebral Compression Fractures Secondary to Pregnancy-induced Osteoporosis: A Case Report
June 10, 2024 Multiple Vertebral Compression Fractures Secondary to Pregnancy-induced Osteoporosis: A Case Report October 1, 2025 Burden, Treatment Patterns, and Functional Recovery of Hand Injuries in a Tertiary Hospital of Eastern India
October 1, 2025 Burden, Treatment Patterns, and Functional Recovery of Hand Injuries in a Tertiary Hospital of Eastern India October 10, 2015 Eckert and Davis Grade 3 Superior Peroneal Retinaculum Injury: Treated by Endoscopic Peroneal Retinaculum Reconstruction and Complicated by Malposition of the Suture Anchors
October 10, 2015 Eckert and Davis Grade 3 Superior Peroneal Retinaculum Injury: Treated by Endoscopic Peroneal Retinaculum Reconstruction and Complicated by Malposition of the Suture Anchors