
It highlights the necessity of responding to potentially fatal injuries quickly, implementing a surgical intervention plan that is phased following the patient’s overall health, and completing open reduction with internal fixation and ligament repair.
Dr. Naveen Sathiyaseelan, Department of Orthopaedics, Saveetha Institute of Medical and Technical Sciences, Chennai, Tamil Nadu, India. E-mail: spnaveen17@gmail.com
Abstract
Introduction: A difficult pattern of injuries is Hotchkiss’s terrible triad, which includes elbow dislocations with fracture of the coronoid and head of radius. It is uncommon to have a concurrent proximal humerus fracture, which makes clinical care even more difficult.
Case Report: An injured worker, 33 years old, claimed to have fallen from a height and received several injuries when he arrived at our emergency center. On physical examination, the patient showed signs of deformity and had an open injury over his left elbow. The radiographic evaluation showed that the patient had a posterior elbow dislocation along with a fracture of the left coronoid, head of radius, and proximal humerus. Following the reduction in a closed manner, computed tomography of the left elbow was carried out for additional assessment. The patient had both the proximal humerus and elbow fixed, and then the elbow was immobilized for 2 weeks.
Conclusion: Complex musculoskeletal injuries resulting from high-energy trauma require a thorough, multidisciplinary strategy to address since long-term results and any consequences will require ongoing monitoring and rehabilitation.
Keywords: Lateral collateral ligament, multidisciplinary approach, proximal humerus fracture, terrible triad.
The phrase “terrible triad” implies a devastating set of injuries that usually include fractures to the radial head, elbow dislocation, and coronoid fracture. When it comes to functional outcomes and management, this intricate damage pattern poses serious issues [1,2]. It is quite uncommon for there to be a simultaneous proximal humerus fracture added to this trio, which further complicates the clinical presentation and treatment choices. One of the more frequent traumatic injuries seen in orthopedic emergency rooms is elbow dislocations. First reported by Hotchkiss in 1996, the “terrible triad” injury is a severe dislocation of the elbow. The traditional symptoms include elbow dislocation, head of radius fracture, and fractured coronoid [3. 4]. To treat this complicated injury, surgical intervention is required to correct the fractures and instability that are a part of this injury pattern. An injury to an extended arm typically results in a valgus strain on the elbow, which dislocates the elbow posterolaterally [5-7]. Nonetheless, it is uncommon for a proximal humerus fracture to occur alongside the ipsilateral dreadful triad of the elbow, and managing such a condition presents special clinical and surgical difficulties. When one considers the awful triad of elbow injuries, such as this one, treatment considerations must take into account the possibility of complications and long-term disability, as well as the need to restore function in both the elbow and shoulder. This study is a case report of a polytrauma patient with an ipsilateral Hotchkiss triad of the elbow accompanied by a Neer’s Type 4 proximal humerus fracture. We discuss the patient’s clinical presentation, diagnostic workup, surgical intervention, and post-operative course.
A male patient, age 33, was brought into our emergency room. In addition, to allegedly having a history of falls from a height of roughly 20 feet, he also reportedly suffered injuries to his left elbow, left shoulder, left leg, head, abdomen, and spine. On inspection, the patient’s overall health was satisfactory. The patient was conscious and aware of time, place, and people. He had stable vitals at the presentation. The patient was bleeding profusely from an open wound covering his right cheek, left elbow, and left ankle. The physical examination revealed a distorted appearance in the left arm and elbow. There was noticeable moderate swelling in the left ankle and arm. The left ankle, bilateral hips, left elbow, and left shoulder all had limited range of motion. On vascular and neurological evaluation, the patient’s extremities were found to be unharmed.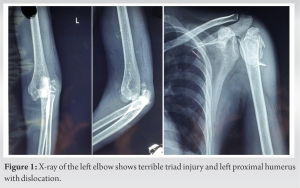
According to the radiographic evaluation, the patient suffered a left coronoid and head of radius fracture with posterior elbow dislocation (Fig. 1), a left superior and inferior pubic rami fracture, a fracture of the L2 to L5 transverse process, and a left proximal humerus fracture (Fig. 1). After a thorough cleansing of the wound, the patient was sewn up. Instability was found, closed reduction was attempted, and repeated elbow examinations were done. An above-elbow slab was placed on the patient. Following closed reduction, a computed tomography scan was carried out for additional assessments. There were found to be an ipsilateral coronoid, ipsilateral radial head, and ipsilateral humeral fractures (Figs. 2 and 3). The patient was ordered to remain under careful immobilization and observation in the intensive care unit due to splenic damage. Therefore, until the patient was fit, the decisive treatment was postponed. Treatment for pelvic and spinal injuries was conservative.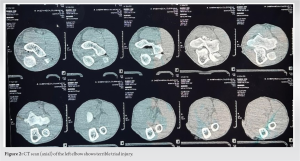
Surgical Procedure
Following a pre-operative assessment, the patient was scheduled for proximal humerus and elbow fixation after 17 days of observation, they were deemed fit for the surgery.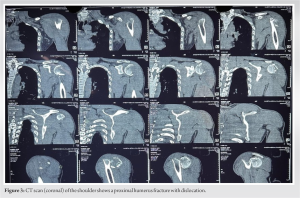 Regional anesthesia was used for the operation of the patient. The first to be operated on was the elbow. With the elbow completely pronated and bent to 90°, the patient was placed in a supine posture to protect the posterior interosseous nerve. By taking a lateral approach and applying Kaplan’s method (Fig. 4), the head of the radius was reached. The avulsed coronoid fragment with the capsule was sutured to the ulna using bone tunnels. The extracted radial head fragments were first secured in vitro using a Herbert screw (Fig. 5), and subsequently, the major component was secured using an additional Herbert screw. Over its original location, LCL was partially torn and remained intact. The LCL was repaired and the elbow was reduced. The deltopectoral technique was then used to operate on the proximal humerus (Fig. 4).
Regional anesthesia was used for the operation of the patient. The first to be operated on was the elbow. With the elbow completely pronated and bent to 90°, the patient was placed in a supine posture to protect the posterior interosseous nerve. By taking a lateral approach and applying Kaplan’s method (Fig. 4), the head of the radius was reached. The avulsed coronoid fragment with the capsule was sutured to the ulna using bone tunnels. The extracted radial head fragments were first secured in vitro using a Herbert screw (Fig. 5), and subsequently, the major component was secured using an additional Herbert screw. Over its original location, LCL was partially torn and remained intact. The LCL was repaired and the elbow was reduced. The deltopectoral technique was then used to operate on the proximal humerus (Fig. 4).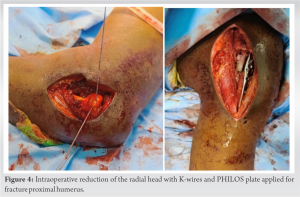 The reduction of fracture was first maintained using k-wires and then fixed with a PHILOS plate (Figs. 5 and 6). The elbow was immobilized in 90-degree flexion for 2 weeks using a posterior slab, followed by elbow and shoulder range of motion exercises. The patient was able to do elbow flexion 30–70°, shoulder flexion 0–100°, extension 0–20°, abduction 0–90°, internal rotation 0–20°, and external rotation 0–30°.
The reduction of fracture was first maintained using k-wires and then fixed with a PHILOS plate (Figs. 5 and 6). The elbow was immobilized in 90-degree flexion for 2 weeks using a posterior slab, followed by elbow and shoulder range of motion exercises. The patient was able to do elbow flexion 30–70°, shoulder flexion 0–100°, extension 0–20°, abduction 0–90°, internal rotation 0–20°, and external rotation 0–30°.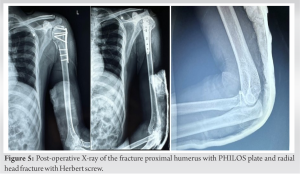
The elbow is limited by both dynamic (muscle) and static factors (bone, ligament, and capsular). The three primary stabilizers are the joint between the ulna and humerus and the lateral and medial collateral ligament. To withstand the different patterns of instability, primary and secondary constraints operate in tandem. When the radioulnar joint dislocates externally relative to the humerus, it causes a posterolateral subluxation of the forearm complex, which is known as posterolateral rotatory instability. An additional pattern is a posteromedial subluxation of the forearm complex accompanied by an internal rotatory dislocation of the radioulnar joint due to posteromedial rotatory instability. There are two types of elbow dislocations: simple and complex. A dislocation without bony injury is a simple elbow dislocation while a complex dislocation has accompanying fractures of bone. Due to their dismal prognosis following treatment, Hotchkiss dubbed complex dislocations of the elbow, with the head of radius and coronoid fractures, the “terrible triad.” They require surgical fixation to mobilize and give stability to the elbow. Surgical difficulties with associated proximal humerus fractures are additional. For improved results, meticulous surgical planning is also necessary. To prevent the proximal humerus implant from failing, the elbow was operated on before the latter.
A terrible triad injury was corrected in the order of the coronoid process head of radius LCL. After reduction, a posterior above the elbow slab was applied. Plate osteosynthesis was then used to repair the proximal humerus. Elbow stability and early mobilization must be balanced in the post-operative rehabilitation plan for this complicated condition. Due to the continuously poor results of immobilizing the elbow for longer than 4 weeks [8,9], our patient underwent 2 weeks of posterior splint at a 90° angle before beginning range-of-motion exercises with a hinged elbow brace. By 8 weeks following surgery, the patient was able to extend his elbow to its fullest. Adequate post-operative follow-up is crucial since it is difficult to treat the issues that arise after surgery. Redislocation, instability, stiffness, myositis ossificans, bursitis, malunion or non-union of fracture, post-traumatic arthritis, and nerve palsy are among the most common sequelae of dreadful triad injuries. The most difficult problem to manage is recurrent dislocation or subluxation [8-10].
The case highlighted how crucial it is to treat trauma systematically. Life-threatening wounds, including a Grade 2 splenic injury, were treated right away. Staged surgical intervention was undertaken immediately when the patient’s general condition improved. Surgical fixation of the head of the radius and coronoid and LCL repair were all accomplished effectively despite the difficult triad damage pattern. Then, in one session, a deltopectoral approach was used to treat the proximal humerus fracture.
Prospectively, further monitoring and rehabilitation will be necessary for the patient’s functional outcomes, potential problems, and quality of life. This case emphasizes the complexity of musculoskeletal injuries brought on by high-energy trauma and emphasizes the value of an all-encompassing, multidisciplinary approach to improving patient recovery and clinical outcomes. Additional investigation and case studies in analogous settings could enhance our comprehension of the handling of such intricate musculoskeletal ailments.
We propose that a detailed surgical strategy is necessary to address associated problems, emphasizing the particular order in which to treat the terrible triad components before reaching the proximal humerus. Furthermore, covered is the post-operative rehabilitation protocol, which emphasizes the need to strike a careful balance between early mobilization and elbow stability to prevent the negative effects of extended immobilization.
References
- 1.Cengiz T, Aydın Ş, Erdoğan F, Mraja HM, Coşkun HS. The terrible triad of the elbow accompanied by capitellum and humerus shaft fracture: A rare case report. Cureus 2022;14:e27658. [Google Scholar | PubMed]
- 2.Courtney PM, Shah RP, Mehta S, Donegan DJ. A terrible quartet injury of the elbow: A terrible triad variant with a capitellar shear fracture: A case report. JBJS Case Connect 2014;4:e88. [Google Scholar | PubMed]
- 3.O’Driscoll SW, Jupiter JB, King GJ, Hotchkiss RN, Morrey BF. The unstable elbow. Instr Course Lect 2001;50:89-102. [Google Scholar | PubMed]
- 4.Hotchkiss RN. Fractures and dislocations of the elbow. In: Rockwood CA Jr., Green DP, Bucholz RW, Heckman JD, editors. Rockwood and Green’s Fractures in Adults. 4th ed. Philadelphia: Lippincott Williams and Wilkins; 1996. p. 929-1024. [Google Scholar | PubMed]
- 5.Desai MM, Sonone SV, Badve SA. Terrible triad of the elbow: A case report of a new variant. J Postgrad Med 2006;52:43-4. [Google Scholar | PubMed]
- 6.Regan W, Morrey B. Fractures of the coronoid process of the ulna. J Bone Joint Surg Am 1989;71:1348-54. [Google Scholar | PubMed]
- 7.Beingessner DM, Dunning CE, Gordon KD, Johnson JA, King GJ. The effect of radial head excision and arthroplasty on elbow kinematics and stability. J Bone Joint Surg Am 2004;86:1730-9. [Google Scholar | PubMed]
- 8.Broberg MA, Morrey BF. Results of treatment of fracture-dislocations of the elbow. Clin Orthop Relat Res 1987;216:109-19. [Google Scholar | PubMed]
- 9.Dubberley JH, Faber KJ, Macdermid JC, Patterson SD, King GJ. Outcome after open reduction and internal fixation of capitellar and trochlear fractures. J Bone Joint Surg Am 2006;88:46-54. [Google Scholar | PubMed]
- 10.McKee MD, Jupiter JB, Bamberger HB. Coronal shear fractures of the distal end of the humerus. J Bone Joint Surg Am 1996;78:49-54. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 The “Terrible Tetrad” of the Elbow: A Case Series of Two Patients with a Rare Quadruple-Component Injury and a Proposed New Classification Term
August 1, 2026 The “Terrible Tetrad” of the Elbow: A Case Series of Two Patients with a Rare Quadruple-Component Injury and a Proposed New Classification Term June 1, 2026 A Rare Neglected Ipsilateral Humeral Triad: Comminuted Proximal Humerus Nonunion with Avascular Necrosis, Mid-Shaft Fracture, and High Radial Nerve Palsy Managed with Staged Reconstruction
June 1, 2026 A Rare Neglected Ipsilateral Humeral Triad: Comminuted Proximal Humerus Nonunion with Avascular Necrosis, Mid-Shaft Fracture, and High Radial Nerve Palsy Managed with Staged Reconstruction December 1, 2025 A Twist in the Shoulder Tale: Proximal Humerus Fracture Following Trapezius Transfer – A Case Report
December 1, 2025 A Twist in the Shoulder Tale: Proximal Humerus Fracture Following Trapezius Transfer – A Case Report November 1, 2025 In Trauma Expect the Unexpected – A Case Report on Post-Traumatic Pancreatitis associated with Superior Mesenteric Artery Pseudoaneurysm in Spinopelvic fracture
November 1, 2025 In Trauma Expect the Unexpected – A Case Report on Post-Traumatic Pancreatitis associated with Superior Mesenteric Artery Pseudoaneurysm in Spinopelvic fracture