
Spontaneous bilateral sagittal band ruptures can occur in non-rheumatoid arthritis individuals and can manifest with hand pain and swelling.
Dr. Fatema Husain Madan, Department of Orthopaedic and Trauma Surgery, Salmaniya Medical Complex, Al Salmaniya Area, Road No 2904, Manama, Bahrain. E-mail: Fatimadan@live.com
Abstract
Introduction: Extensor tendon subluxation or dislocation resulting from sagittal band rupture can be associated with snapping, catching, locking, pain, and swelling of the finger. Several etiologies were reported in the literature, with frequent mention of a traumatic rupture caused by a direct blow at the level of the metacarpophalangeal joint (MCPJ). The other causes of sagittal band injuries are degenerative disease, congenital infection, and rheumatoid arthritis. To our knowledge, we report the first case of spontaneous idiopathic bilateral sagittal band rupture.
Case Report: We, herein, present the case of a seronegative 29-year-old female who presented with pain and swelling in the dominant hand for 4 days.
Conclusion: Upon examination, she was found to have bilateral dislocation of the extensor tendons at the level of the (MCPJ) of the third and fourth digits. Any underlying cause was excluded, and the diagnosis was confirmed with a dynamic ultrasound study.
Keywords: Sagittal band, extensor tendon dislocation, spontaneous sagittal band rupture, metacarpophalangeal joint, hand pain.
The sagittal band functions as the primary stabilizer of the extensor tendon at the level of the metacarpophalangeal joint (MCPJ), preventing the tendon from subluxation laterally [1]. Rupture of the sagittal band can result in extensor tendon subluxation or dislocation, presenting with hand pain and swelling [2]. Several etiologies were reported in the literature, frequently mentioning a traumatic rupture caused by a direct blow to the MCPJ or low-energy trauma, a condition widely known as Boxer’s knuckle [3,4]. However, atraumatic ruptures can be due to congenital absence of the sagittal band [5], spontaneous rupture [4], degenerative disease [6], or inflammatory causes, commonly, rheumatoid arthritis leading to chronic MCP synovitis resulting in attenuation of the band [6]. Spontaneous sagittal band ruptures have been described to be caused by snapping, crossing a finger, or crumpling a piece of paper. However, spontaneous ruptures are uncommon among individuals who have not been diagnosed with an autoimmune arthropathy [4]. We report that a rare presentation, to our knowledge, is the first case of spontaneous idiopathic bilateral sagittal band rupture, where a 29-year-old healthy female presented with right-hand pain and swelling for 4 days. Clinical examination suggested extensor tendon dislocation in both hands. Any other etiologies were excluded, and a dynamic ultrasound study confirmed the diagnosis.
A 29-year-old right-handed female with no previous medical condition has presented with sudden onset right-hand pain, swelling, and stiffness at the MCPJ level for 4 days. She denied any history of trauma, fall, recent repetitive athletic activity, or a feeling of a sudden snap sensation involving her hand. She had a history of similar symptoms in 2012 at the level of the distal interphalangeal joint, where she was diagnosed with reactive arthritis and treated with oral penicillin. She claims to have had a similar presentation the following year and was treated with antibiotics. She has no family history of similar symptoms and no record of any inflammatory diseases in the family. However, she has a habit of continuously snapping her fingers.
In addition, she complained of diffuse bluish discoloration of the fingertips and joint pain when exposed to cold temperatures. She is a medical doctor, but her routine job involves typing on a computer. She also has a longstanding habit of cracking her knuckles.
Upon examination, she had moderate swelling and tenderness over the dorsal aspect of the right third and fourth digits, with maximum tenderness over the level of the metacarpal heads (Fig. 1). Furthermore, an active range of motion causes pain and discomfort more pronounced with active extension. Her left hand was not swollen and was non-tender. Flexion at the MCPJ produced pain and ulnar dislocation of the extensor tendon at that level of the third and fourth digits in both hands. Moreover, she had ulnar dislocation of the extensor tendon of the right fifth digit. In full extension, the extensor tendons were centralized. She was treated conservatively by strapping the third and fourth digits, and a wrist splint was applied; she improved within 5 days.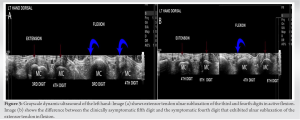
Investigations
Blood investigations were also done, including erythrocyte sedimentation rate, rheumatoid factor, and antinuclear antibodies, which were all negative. Plain X-rays at the time showed no fractures, dislocation, bony erosions, or arthritis.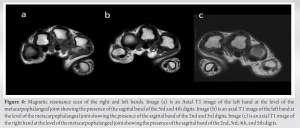
A specialist musculoskeletal radiologist performed a dynamic ultrasound. A 15-MHz linear transducer was used. Focal zone, imaging depth, and post-processing parameters were optimized for musculoskeletal imaging. The common extensor tendon dorsal to the MCPJ in the affected finger and the same tendon in the contralateral asymptomatic finger were either passively or actively flexed or extended. A pad made of a towel and a large amount of transmission gel were used (Fig. 2 and 3). The ultrasound images established the presence of the sagittal bands in all extensor tendons bilaterally. The diagnosis of bilateral sagittal band rupture was confirmed with the images showing ruptured bands in multiple digits of both hands. Radial sagittal band rupture was seen in both hands’ third and fourth digits, in addition to ulnar sagittal band rupture in the fifth digit of the right hand. The extensor tendons of the first and second digits were intact bilaterally. Moreover, the thickness of the sagittal bands was measured and confirmed to be within the normal range, which measured 1–2 mm, and preserved a normal morphological appearance. No signs of the inflammatory process could be appreciated to involve the tendons or the underlying joint. Bilateral hand magnetic resonance imaging was done and showed the presence of sagittal bands in all digits (Fig. 4).
Follow-up and outcome
At the 12-month follow-up, the examination revealed reduced swelling and a full range of motion of the hand joints. However, the extensor tendon dislocation at the level of MCPJs persists.
The dorsal hood covers the MCPJ, a reticular system made of three structures: The sagittal, the oblique, and the transverse bands. The sagittal band stabilizes the extensor tendon at the level of the MCPJ, whereas the oblique and transverse bands extend distally [7]. The sagittal band comprises two deep and superficial layers, forming a tunnel through which the extensor tendon passes [4,7]. Spontaneous ruptures are associated with rupture of only the superficial layer of the sagittal band at the insertion point on the extensor digitorum communis (EDC) radial aspect, detaching it from the radial and palmar connections to the deep sagittal band and causing ulnar dislocation of the extensor tendon. On the contrary, traumatic ruptures involve both the sagittal band’s superficial and deep layers [2,4]. In a ruptured sagittal band, the extensor tendon tends to dislocate to the ulnar direction following the direction of the MCP head slope [8]. As seen in the current patient, the sagittal band rupture typically occurs in the long finger [9]. It is believed to be due to the length of the digit and the relatively weak attachment to the dorsal hood [10]. Our patient presented with pain and swelling in the dominant hand, stating that this was the first time she had experienced this pain. Initially, we were suspicious of hypoplastic versus congenital absence of the sagittal bands, which was ruled out by dynamic ultrasound [11,12]. However, it is not feasible to know the exact time in which the sagittal band was ruptured. Spontaneous sagittal band rupture is rare in non-rheumatoid individuals and is unusual to be bilateral. Inoue et al. [11] reported 27 cases of sagittal band ruptures with extensor tendon dislocations. Seven of them had spontaneous dislocations in the long finger in the ulnar direction, whereas the little finger exhibited dislocation in the radial direction. However, none presented with bilateral extensor tendon dislocation of the hands. They also mentioned two cases with congenital dislocation of the EDC, where dislocation was noticed before the age of 10 years, and the radial sagittal band was either absent or thin. In contrast to our case, the ultrasound revealed an existing sagittal band with average thickness measurement [11]. Moreover, Ishizuki et al. [4] followed 16 patients with ulnar dislocation of the extensor tendon; 11 were classified as spontaneous, although they had a history of low-energy accidents such as snapping, crossing a finger, or crumpling paper [4]. Observing extensor tendon dislocation from their central position while the patient clenches their fist in dynamic ultrasound is diagnostic of sagittal band disruption [12]. The thickness of the sagittal band in our patient was within the average range compared to Kichouh et al. measurements of 21 volunteers, who underwent high-resolution ultrasound imaging of the fingers by two radiologists. The mean radial sagittal band thickness was 0.64 mm in the dominant middle finger and 0.55 mm in the dominant ring finger [13]. The mode of management of sagittal band ruptures is still controversial. It can be managed conservatively or with surgical intervention. Surgical intervention is indicated in chronic or when painful subluxation persists despite conservative management. Direct repair is possible in the acute setting [14].
Bilateral spontaneous sagittal band rupture can occur in individuals without underlying autoimmune arthropathy, resulting in hand pain and swelling. Management includes strapping and non-steroidal anti-inflammatory drugs. Surgical intervention with tendon stabilization might be indicated if no improvement is seen with conservative measures.
Sagittal band rupture can present as hand swelling and pain. Treatment is mainly conservative but surgical intervention is indicated in cases not improving with conservative measures.
References
- 1.Chinchalkar SJ, Barker CA, Owsley B. Relationship between juncturae tendinum and sagittal bands. J Hand Microsurg 2015;7:96-101. [Google Scholar | PubMed]
- 2.Mitsuzawa S, Ando M, Takeuchi H, Noguchi T, Ikeguchi R, Matsuda S. Functional anatomy of the sagittal bands and mechanisms of extensor tendon dislocation: A cadaveric study. J Hand Surg Eur Vol 2021;46:842-6. [Google Scholar | PubMed]
- 3.Capo JT, Shamian B, Rossy W, Hashem J. Closed sagittal band injury due to low energy trauma. Am J Orthop (Belle Mead NJ) 2012;41:374-7. [Google Scholar | PubMed]
- 4.Ishizuki M. Traumatic and spontaneous dislocation of extensor tendon of the long finger. J Hand Surg 1990;15:967-72. [Google Scholar | PubMed]
- 5.Çirpar M, Dağlar B, Oktaş B. Congenital extensor tendon dislocation causing pseudotriggering of the little finger. Acta Orthop Traumatol Turc 2017;51:429-31. [Google Scholar | PubMed]
- 6.Kozlow JH, Chung KC. Current concepts in the surgical management of rheumatoid and osteoarthritic hands and wrists. Hand Clin 2011;27:31-41. [Google Scholar | PubMed]
- 7.Kichouh M, Vanhoenacker F, Jager T, Van Roy P, Pouders C, Marcelis S, et al. Functional anatomy of the dorsal hood or the hand: Correlation of ultrasound and MR findings with cadaveric dissection. Eur Radiol 2009;19:1849-56. [Google Scholar | PubMed]
- 8.Hakstian RW, Tubiana R. Ulnar deviation of the fingers. The role of joint structure and function. J Bone Joint Surg Am 1967;49:299-316. [Google Scholar | PubMed]
- 9.Kang N, Smith P. Congenital absence of the juncturae tendini contributing to dislocation of the extensor tendons. J Hand Surg 2001;26:501-5. [Google Scholar | PubMed]
- 10.Kettelkamp DB, Flatt AE, Moulds R. Traumatic dislocation of the long-finger extensor tendon: A clinical, anatomical, and biomechanical study. J Bone Joint Surg Am 1971;53:229-40. [Google Scholar | PubMed]
- 11.Inoue G, Tamura Y. Dislocation of the extensor tendons over the metacarpophalangeal joints. J Hand Surg 1996;21:464-9. [Google Scholar | PubMed]
- 12.Willekens I, Kichouh M, Boulet C, De Maeseneer M, Clarys JP, De Mey J. Ultrasound follow-up of posttraumatic injuries of the sagittal band of the dorsal hood treated by a conservative approach. Eur J Radiol 2015;84:278-83. [Google Scholar | PubMed]
- 13.Kichouh M, De Maeseneer M, Jager T, Marcelis S, Van Hedent E, De Mey J. The thickness of the sagittal bands in volunteers: high resolution ultrasound of the fingers. Surg Radiol Anat 2011;33:65-70. [Google Scholar | PubMed]
- 14.Grandizio LC, Klena JC. Sagittal band, boutonniere, and pulley injuries in the athlete. Curr Rev Musculoskeletal Med 2017;10:17-22. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Eight-Year Neglected Pediatric Kaplan’s MCP Dislocation Following Childhood Trauma Managed by Volar Open Reduction: A Case Report
April 1, 2026 Eight-Year Neglected Pediatric Kaplan’s MCP Dislocation Following Childhood Trauma Managed by Volar Open Reduction: A Case Report June 1, 2025 Management of a Rare Case of Complex and Irreducible Dislocation of the Metacarpophalangeal Joint in the Little Finger – A Case Report
June 1, 2025 Management of a Rare Case of Complex and Irreducible Dislocation of the Metacarpophalangeal Joint in the Little Finger – A Case Report November 10, 2023 Metacarpal Joint Arthroplasty in the Acute Setting: A Case Report
November 10, 2023 Metacarpal Joint Arthroplasty in the Acute Setting: A Case Report December 10, 2022 Digital Arterial Occlusion at the Metacarpophalangeal Joint with Hypothenar Hammer Syndrome-like Symptoms: A Case Report
December 10, 2022 Digital Arterial Occlusion at the Metacarpophalangeal Joint with Hypothenar Hammer Syndrome-like Symptoms: A Case Report