
This case highlights that a strong clinical suspicion should be raised, supported by blood and radiological investigations to diagnose very unusual sites of TB like that of navicular bone. It is a rare condition and can be treated conservatively with near-complete function and recovery if diagnosed early. ATT can be stopped at 11–12 months if postcontrast-enhanced MRI reveals no intra/extra osseous enhancement or collection.
Dr. Amartya Gain, Department of Orthopaedics, University College of Medical Sciences and GTB Hospital, Tahirpur Rd, GTB Enclave, Dilshad Garden, New Delhi-110 095, India. E-mail: amartyagain@gmail.com
Abstract
Introduction: Tuberculosis (TB) is a global public health problem, endemic to India. Osteoarticular TB uncommonly presents in the foot, navicular osteomyelitis is an extremely rare entity.
Case Report: We report a rare case of navicular osteomyelitis caused by TB in a 37-year-old man who presented to OPD with swelling and dull aching pain over the dorsum of his left foot. A radiograph of the foot showed a lytic lesion in the navicular bone. Further investigations in the form of aspiration cytology, cartridge-based nucleic acid amplification test, and acid-fast bacilli culture confirmed TB. Category-1 anti-tubercular therapy was started immediately and the patient was treated conservatively. Four drugs (HRZE) were given for 2 months and 3 drugs (HRE) for 9 months, after which the patient stopped his medications on his own. Radiographs and CEMRI at 14-month follow-up showed a healed lesion.
Conclusion: This case illustrates an exceptional location of osteoarticular TB and shows that Navicular TB can be treated conservatively with near-complete function and recovery if diagnosed early.
Keywords: Navicular TB, ATT, foot and ankle TB.
Foot and ankle TB comprises <1% of all instances of bone tuberculosis (TB) [1]. Osteoarticular TB of the navicular bone is extremely rare. The knowledge of rare sites of tubercular infections and unusual presentation makes clinicians more susceptible and pick signs of TB early.
A 37-year-old male presented to the orthopedics outpatient department with chief complaints of pain and swelling over left foot for the last 1.5 months. The swelling increased slowly in the 1.5-month duration. There was no history of such swelling anywhere else in the body. The pain was dull aching and increased on weight bearing and walking. The pain was relieved by taking analgesics and giving rest to the foot. There was no history of trauma, fever, malaise, loss of appetite, or weight loss. The patient had neither history of contact with TB nor history of TB. Local examination revealed an erythematous, tender swelling of about 3 × 3 cm on the anteromedial aspect of the dorsum of the left mid-foot with slightly raised local temperature. Fluctuation could not be appreciated. There was no discharging sinus, ulcer, or healed scar in the area. The patient had a normal range of motion around the ankle and foot. A radiograph of the foot showed a lytic lesion in the navicular bone with the fuzziness of margins specifically toward the distal part (Fig. 1). His Chest X-ray was within normal limits. MRI foot (Fig. 2) revealed hypo intensity in the navicular bone on T1-weighted and hyperintensity on T2-weighted films which was suggestive of inflammation of the navicular bone with intraosseous abscess.
Laboratory investigation revealed a raised erythrocyte sedimentation rate (ESR) (50) and C-reactive protein (CRP) (79) with a normal TLC count (6000). A clinical diagnosis of Pyogenic/Tubercular/ Fungal Osteomyelitis was made. Thick bore needle aspiration was done and about 5 mL pus was aspirated (Fig. 3). Samples were sent for: Pus cs and gram stain, acid-fast bacilli (AFB) smear, liquid culture, and sensitivity to 13 anti-tubercular drugs (Isoniazid, Rifampicin, Kanamycin, Amikacin, Capreomycin, Levofloxacin, Moxifloxacin, Ethionamide, Para aminosalicylic acid, Linezolid, Bedaquiline, Delamanid, and Clofazimine), cytopathology, cartridge-based nucleic acid amplification test (CBNAAT) and line probe assay (LPA). CBNAAT detected M. TB and was rifampicin sensitive. The patient was started on cat-1 anti-tubercular therapy (ATT) based on clinico-imaging and CBNAAT findings. LPA also detected MTB and was sensitive to both 1st line (INH and RIF) and 2nd line drugs (FQs and SLIDs). The stain for AFB was negative. Culture detected MTB and liquid drug sensitivity testing revealed sensitivity to all 13 anti-tubercular drugs.
In follow-up, the radiographs and blood tests in the form of CBC, ESR, CRP, and LFT were performed at 2 months, 4 months, and 7 months of ATT intake (Fig. 4, 5, and 6). The foot was protected in a below-knee slab for 8 weeks. Partial weight bearing was allowed at 8 weeks followed by full weight bearing at 16 weeks.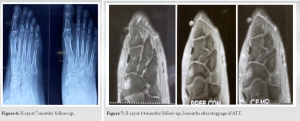
The patient took cat-1 ATT 4 drugs: Rifampicin 450 mg, INH 300 mg, ETB 1200 mg, pyrazinamide 1500 mg fixed-dose combination for the first 2 months in the intensive phase and then rifampicin 450 mg, INH 300 mg, and ETB 1200 mg in continuation phase for 9 months and then stopped on his own and presented to us 3 months post stoppage of ATT. Complete resolution of pain and swelling was there without any recurrence. Blood investigation revealed normal ESR (5) and slightly raised CRP (11) with normal TLC count (4540). Radiographs and CEMRI were done which showed signs of healed lesion. X-ray showed sclerosis around the residual lytic cavity (Fig. 7). CEMRI showed focal residual marrow edema without any post-contrast ring enhancement (Fig. 8).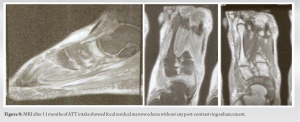
Foot TB accounts for 5–10% of OATB with calcaneum, talus, first metatarsal, cuboid, medial, and intermediate cuneiforms being the most involved bones[1]. Osteoarticular TB either presents as osteomyelitis or as arthritis. The former often involves one single bone but can be multifocal. Very few cases have been reported of isolated navicular bone TB (Table 1).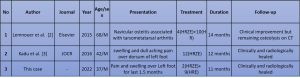
Foot TB symptoms are often chronic and insidious. The most common symptom is pain. Our patient was complained about pain and swelling over the midfoot region. The diagnosis was suspected by X-ray and further supported by raised ESR and CRP. The radiological appearances of rheumatoid arthritis particularly when monoarticular, osteoarthritis, gout, neuropathic joints, sarcoidosis and neoplasms may be similar, but can be differentiated from those of osteoarticular TB [1]. MRI is the gold standard imaging modality to diagnose TB in early stages when X-ray and CT scan can be normal [4]. However, MRI images of osteolysis can suggest other diagnoses such as chronic osteomyelitis, brucellosis, tumors such as osteoid osteoma or chondroma, and metabolic diseases such as hyperparathyroidism and Paget’s disease. The prognosis for OATB is improved by early diagnosis and intervention [5]. There is a mean delay of 6–8 months before the diagnosis is ascertained particularly in endemic countries due to difficulty in procuring sample from deep seated lesion, difficulty in demonstrating AFB on smear, culture and histology due to the paucibacillary nature of disease and difficulty in detecting early lesions on plain radiographs as at least 30–40% mineral density should be lost before changes appear on radiographs which usually takes 3–6 months [6,7]. Genotypic DST can reduce this delay and preventthe development of complications, thus improving prognosis [7,8]. No single modality can ascertain the diagnosis in all cases of OATB [9]. Hence, we had sent the sample aspirated from midfoot swelling for molecular tests, histopathology culture and DST [10].
Anti-tubercular therapy is the mainstay of treatment modality. 2(HRZE)/10–16(HRE) with rest to the joint in a functional position (in plaster/ ankle-foot orthoses) for 4–6 weeks followed by gentle non-weight-bearing mobilization as tolerated. Surgery is rarely required, but is indicated for impending bone collapse, large abscess, or correction of deformity in healed patients.
ATT can be stopped at 11–12 months if post contrast enhanced MRI reveals no intra/extra osseous enhancement or collection in cases of osteoarticular TB.
References
- 1.Tuli SM. Tuberculosis of the Skeletal System: Bones, Joints, Spine and Bursal Sheaths. New Delhi: Jaypee Brothers Medical Publishers Pvt. Limited; 2010. [Google Scholar | PubMed]
- 2.Lemnouer A, Frikh M, Belfquih B, Jaafar A, Bouya A, Jidal M, et al. Navicular tuberculosis: A rare localization of bone tuberculosis. IDCases 2015;2:80-2. [Google Scholar | PubMed]
- 3.Kadu VV, Saindane KA, Godghate N, Godghate N. Tuberculosis of navicular bone-a rare presentation. J Orthop Case Rep 2016;6:76-8. [Google Scholar | PubMed]
- 4.Sharma A, Chhabra HS, Mahajan R, Chabra T, Batra S. Magnetic resonance imaging and genexpert: A rapid and accurate diagnostic tool for the management of tuberculosis of the spine. Asian Spine J 2016;10:850-6. [Google Scholar | PubMed]
- 5.Gain A, Jain AK, Bhalla M, Aggarwal AN, Dhammi IK, Arora VK. Drug resistance in osteoarticular tuberculosis: A study from an endemic zone. Cureus 2023;15:e44173. [Google Scholar | PubMed]
- 6.Jain AK, Jena SK, Singh MP, Dhammi IK, Ramachadran VG, Dev G. Evaluation of clinico-radiological, bacteriological, serological, molecular and histological diagnosis of osteoarticular tuberculosis. Indian J Orthop 2008;42:173-7. [Google Scholar | PubMed]
- 7.Wang G, Dong W, Lan T, Fan J, Tang K, Li Y, et al. Diagnostic accuracy evaluation of the conventional and molecular tests for spinal tuberculosis in a cohort, head-to-head study. Emerg Microbes Infect 2018;7:109. [Google Scholar | PubMed]
- 8.Upadhyay M, Patel J, Kundnani V, Ruparel S, Patel A. Drug sensitivity patterns in Xpert-positive spinal tuberculosis: An observational study of 252 patients. Eur Spine J 2020;29:1476-82. [Google Scholar | PubMed]
- 9.Abhimanyu S, Jain AK, Myneedu VP, Arora VK, Chadha M, Sarin R. The role of cartridge-based nucleic acid amplification test (CBNAAT), line probe assay (LPA), liquid culture, acid-fast bacilli (AFB) smear and histopathology in the diagnosis of osteoarticular tuberculosis. Indian J Orthop 2021;55:157-66. [Google Scholar | PubMed]
- 10.Convenors I. Initiative of Central TB Division Ministry of Health and Family Welfare, Government of India INDEX-TB GUIDELINES-Guidelines on Extra-pulmonary Tuberculosis for India; 2016. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 March 10, 2024 Unifocal Tubercular Osteomyelitis of Ulna Diaphysis in a Child: A Case Report
March 10, 2024 Unifocal Tubercular Osteomyelitis of Ulna Diaphysis in a Child: A Case Report October 1, 2024 Sclerotherapy as a Primary or Salvage Procedure for Aneurysmal Bone Cyst: A Case Report
October 1, 2024 Sclerotherapy as a Primary or Salvage Procedure for Aneurysmal Bone Cyst: A Case Report October 14, 2014 The Acute and Chronic Presentation of Gluteus Medius Calcific Tendinitis- A Case Report of Two
October 14, 2014 The Acute and Chronic Presentation of Gluteus Medius Calcific Tendinitis- A Case Report of Two July 10, 2022 Reviewers Acknowledgement & Photo Gallery July 2022
July 10, 2022 Reviewers Acknowledgement & Photo Gallery July 2022