
Posterior dislocation of the hip requires emergent intervention and it can be complicated by ipsilateral shaft femur fracture; knowledge of the appropriate reduction maneuvers is of paramount importance.
Dr. Amit Kumar Salaria, Department of Orthopaedic Surgery, All India Institute of Medical Sciences, Bilaspur, Himachal Pradesh, India. E-mail: meetamit20salaria@gmail.com
Abstract
Introduction: The incidence of ipsilateral fracture of the shaft of the femur and dislocation of the hip are extremely rare injuries. However, the incidence of complex fractures is increasing day by day due to an increasing variety of traumatic mechanisms. This type of injury constitutes various diagnostic and treatment difficulties for the surgeon. Such injuries should be managed on an urgent basis for better functional outcomes.
Case Report: We hereby describe two such cases: First case hip was reduced using external fixator pins, stabilization of the shaft femur fracture was done with an external fixator and the second case hip was reduced with bone holding clamps and the shaft femur fracture was fixed with interlocking nail.
Conclusion: Fixator-assisted closed reductions are the first line of treatment in the management of posterior dislocation hip complicated with ipsilateral femoral shaft fractures. If closed reduction fails, fracture site can be opened and direct forces can be applied to the proximal femur to aid hip reduction with minimum complications.
Keywords: Ipsilateral, posterior hip dislocation, shaft femur fracture, close reduction.
The complexity of fractures has significantly increased due to the increasing variety of traumatic mechanisms such as high-speed collisions, falls from heights, and construction-related high-energy injuries. These fractures tend to drift from the standard classification systems and their treatment is usually controversial because of varying outcomes. One such example is hip dislocations associated with head, neck, intertrochanteric, shaft, distal femur fractures, or knee dislocation [1]. In this report, we study the two cases who sustained a posterior hip dislocation with concomitant ipsilateral femur shaft fractures. Only a few such cases reported in the literature [2]. In our first case, hip was reduced using external fixator pins and stabilization of the shaft femur fracture was done with an external fixator, and in the second case, the hip was reduced with bone-holding clamps, the shaft femur fracture was fixed with an interlocking nail.
An 11-year-old female patient reported to our emergency department (ED) following a road traffic accident with severe pain in the right hip and right thigh. The patient had a deformity of the right hip and thigh and was unable to walk. On clinical examination, we found that she had flexion-adduction deformity of the right hip. Her leg and foot showed external rotation and abduction. There was tenderness and abnormal mobility at the right thigh. In addition, there was tenderness at the right hip joint and the femoral head was palpable in the gluteal region. The range of movements at the right hip was grossly restricted and painful. There was no distal neurovascular deficit noted. After providing the advanced trauma life support in causality, the patient was sent for radiography. X-rays of the pelvis with both hips and of the right thigh with hip and knee were taken (Fig. 1).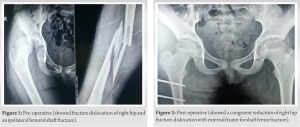
From the radiograph, we confirmed that there was a comminuted fracture in the shaft of the femur and a posterior dislocation in the hip. The patient was taken to an emergency OT and subjected to closed manipulation of the hip joint. As there was a fracture in the shaft of the femur, the force was not transmitted to the hip joint and we are unable to reduce the hip dislocation. We placed a temporary external fixator pin in the femur under anesthesia, and the external fixator rod was used as a handle to perform closed manipulation and reduction of dislocation of the hip using the Allis method. Femur shaft fracture was fixed with a closed reduction and stabilization with an external fixator, two pins each in the proximal and distal femoral part. Finally, fracture alignment is checked under fluoroscopy (Fig. 2). In the second case, a 44-year-old man presented to the emergency trauma room following a motor vehicle accident, and the patient was standing roadside and hit by vehicle. In the emergency ward, orthopedic and general surgeon assessed the patient initially and implemented the advanced trauma life support protocol [3]; he was deemed to be hemodynamically stable with no other systemic injuries. The patient was, however, complaining of left hip and thigh pain as well as pain in the right lower limb. On examination, he was noted to have abducted, shortened, and internally rotated his left lower limb. Active and passive movements of the left thigh were not possible due to pain with no neurovascular deficits detected distally. There were swelling, tenderness, and bony creeps in the mid-shaft of the right tibia. X-rays of the pelvis and left femur revealed a posterior fracture dislocation of the left femoral head with an ipsilateral femoral mid-shaft fracture. A right lower limb X-ray also revealed both bone leg fractures at mid-shaft level (Fig. 3). An attempt of left hip closed reduction was made while the patient was still in the ED and it was however unsuccessful.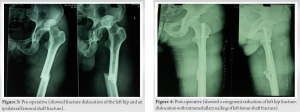
After being cleared by the trauma team, the patient was admitted to the orthopedic ward with a working diagnosis of left posterior hip dislocation with an ipsilateral femoral shaft fracture and both bone leg fractures right side. The patient was taken to the operating theater for closed versus open reduction and intramedullary (IM) nailing of the left femur. A close reduction trial was unsuccessful. The patient was positioned laterally and fracture site was opened and the proximal femoral part was held with bone holding clamp and hip dislocation was reduced using the Allis method. Shaft femoral fracture stabilized with IM nail (Fig. 4). As the patient was stable intraoperatively, the right tibia fracture was also stabilized with close reduction and ILN. After completion of the procedure, the left hip was examined and found to be stable. The patient was discharged after 5 days with a clean, dry wound.
The primary challenge in these cases was achieving closed reduction of the hip dislocation, and this was particularly difficult due to the inability to transmit the force needed for reduction through to the hip and the difficulty controlling the thigh [4]. Both of these problems were caused by the concomitant fracture in the femoral shaft [5]. This necessitated the use of other indirect/direct methods of reduction such as the temporary external fixator or holding the proximal femoral part with bone holding clamp [6]. These challenges were also faced by other treating surgeons in similar cases and each team was able to achieve the reduction by closed manipulation or manual traction maneuvers, indirect reduction with the aid of external tools such as Schanz pins and open reduction [7]. Early reduction of the dislocation is important to prevent significant complications associated with late reduction such as osteonecrosis and subsequent hip arthritis [8]. In our first case, using an external fixator helped in the indirect reduction of hip dislocation and precluded open reduction-related complications. In our second case after a failed close reduction trial, we planned to open the fracture site and reduce hip dislocation by applying direct forces to the proximal femur part and then retrograde open IM nailing for femoral shaft fracture. At 6-week follow-up fracture was united with a healthy surgical site gave satisfactory results without any complications [9,10].
Ipsilateral fractures of the femur shaft and hip dislocation are rare injuries and are always difficult to be diagnosed and treated. These injuries are always considered an orthopedic emergency. In such conditions, fixator-assisted reduction of hip dislocation followed by closed reduction and external fixator stabilization for femoral shaft fracture in children and open reduction and fracture fixation with retrograde ILN in adults give satisfactory results with minimal complications.
Posterior dislocation of the hip associated with femoral shaft fracture is a complicated scenario. For appropriate reduction and leverage external fixator with Schanz screws and bone-holding forceps can be a valuable tool .
References
- 1.Stannard JP, Harris HW, Volgas DA, Alonso JE. Functional outcome of patients with femoral head fractures associated with hip dislocations. Clin Orthop Relat Res 2000;377:44-56. [Google Scholar | PubMed]
- 2.Dummer RE, Sanzana ES. Hip dislocations associated with ipsilateral femoral neck fracture. Int Orthop 1999;23:353-4. [Google Scholar | PubMed]
- 3.Radvinsky DS, Yoon RS, Schmitt PJ, Prestigiacomo CJ, Swan KG, Liporace FA. Evolution and development of the advanced trauma life support (ATLS) protocol: A historical perspective. Orthopedics 2012;35:305-11. [Google Scholar | PubMed]
- 4.Jamshidi MH, Mirkazemi M, Birjandinejad A. Posterior hip fracture-dislocation associated with ipsilateral intertrochantric fracture; A rare case report. Arch Bone Jt Surg 2014;2:75-8. [Google Scholar | PubMed]
- 5.Verdonk R, de Smet L. Hip dislocation combined with femoral shaft fracture. Two cases treated with the Lardennois hoop. Acta Orthop Scand 1984;55:185-6. [Google Scholar | PubMed]
- 6.Zhen P. Traumatic posterior hip dislocation with an ipsilateral comminuted femoral intertrochanteric fracture: A case report. Orthop Surg 2013;5:219-21. [Google Scholar | PubMed]
- 7.DuBois B, Montgomery WH Jr., Dunbar RP, Chapman J. Simultaneous ipsilateral posterior knee and hip dislocations: Case report, including a technique for closed reduction of the hip. J Orthop Trauma 2006;20:216-9. [Google Scholar | PubMed]
- 8.Pipkin G. Treatment of grade IV fracture-dislocation of the hip. J Bone Joint Surg Am 1957;39-A:1027-42 passim. [Google Scholar | PubMed]
- 9.Alho A. Concurrent ipsilateral fractures of the hip and femoral shaft: A meta-analysis of 659 cases. Acta Orthop Scand 1996;67:19-28. [Google Scholar | PubMed]
- 10.Sanders S, Tejwani N, Egol KA. Traumatic hip dislocation--a review. Bull NYU Hosp Jt Dis 2010;68:91-6. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Arthroscopic-Assisted Removal of Incarcerated Fragment following Manual Reduction of Posterior Hip Dislocation in Acute Polytrauma Patient: A Case Report
February 1, 2026 Arthroscopic-Assisted Removal of Incarcerated Fragment following Manual Reduction of Posterior Hip Dislocation in Acute Polytrauma Patient: A Case Report September 1, 2025 Total Hip Arthroplasty with Cage Application for Complex Posterior Hip Dislocation and Acetabular Fracture in a Patient with Prior Patellectomy: A Case Report
September 1, 2025 Total Hip Arthroplasty with Cage Application for Complex Posterior Hip Dislocation and Acetabular Fracture in a Patient with Prior Patellectomy: A Case Report September 1, 2025 Triple-Segmental Shaft Femur Fracture: A Case Report
September 1, 2025 Triple-Segmental Shaft Femur Fracture: A Case Report December 10, 2023 Uncommon Yet Noteworthy: A Clear and Comprehensive Case Report on Pediatric Hip Dislocation
December 10, 2023 Uncommon Yet Noteworthy: A Clear and Comprehensive Case Report on Pediatric Hip Dislocation