
The ability to recognize Van Neck-Odelberg disease, a rare cause of pediatric hip pain, allows for effective treatment and avoidance of unnecessary procedures.
Mr. Liam McLoughlin, Medical Student (MS3), Florida State University College of Medicine, Tallahassee, FL, USA. E-mail: ltm20z@med.fsu.edu
Abstract
Introduction: Synchondrosis ischiopubic syndrome (SIS), also known as Van Neck-Odelberg disease, is a benign skeletal abnormality in children due to delayed closure in the ischiopubic synchondrosis (IPS). Patients may present with vague groin, hip, or buttock pain that can cause limitation of hip movement or limp. Few descriptions of this disorder exist, and it can easily be mistaken for other pathologies, including stress fracture, osteomyelitis, or tumor.
Case Report: We report the case of a 9-year-old female gymnast presenting with right hip pain who was diagnosed with SIS. She was managed conservatively by the pediatric orthopedist.
Conclusion: Van Neck-Odelberg disease is a rare cause of pediatric hip pain that can be mistaken for other more serious pathologies. The ability to recognize the disease early allows for effective treatment and the avoidance of unnecessary procedures.
Keywords: Hip pain, pediatric, synchondrosis ischiopubic syndrome, Van Neck-Odelberg disease.
The ischiopubic region of the pelvis is formed by two different ossification centers, the superomedial pubic center and inferolateral pubic center [1]. Between these two centers is a strip of cartilaginous tissue called the ischiopubic synchondrosis (IPS) [2]. Like all synchondroses, it is a temporary joint that is present during childhood, before fusion of the ischium and pubic bone. Usually, the ischium and pubic bone fuse without any clinical symptoms. Fusion is typically observed between the ages of 4 and 9 years in females and 7 and thirteen in males [3]. However, some children may experience pain and limitation of movement associated with enlargement of the IPS and delayed fusion of the ischium and pubis [4]. Drs. Odelberg (1923) and Van Neck (1924) described an enlargement of the IPS in radiographs taken in symptomatic children [5,6]. Thereafter, this clinical phenomenon became known as Van Neck-Odelberg disease or synchondrosis ischiopubic syndrome (SIS). Its non-specific symptomatology and radiological features that may mimic other pathologies create a challenge in diagnosis. The ability to diagnose SIS early on allows for effective treatment and avoidance of unnecessary procedures. We present the case of a 9-year-old female gymnast presenting with right hip pain who was later diagnosed with SIS.
A 9-year-old female presented to our clinic with a 4-month history of right hip pain. She was a competitive gymnast but had no history of injury. Pain was present on a daily basis, mostly in the afternoon. The patient and her mother noted an occasional limp, especially when she had to do a lot of walking. She had not been taking any medications for pain. There was tenderness on range of motion of her right hip. Range of motion of the hip was also limited with pain at the end range of passive hyperflexion and external rotation while at 90 degrees of flexion. While lying flat, her hip joint was semiflexed. She had moderate tenderness to palpation over the right pubic bone. No swelling, redness, or raised local temperature was noted in the hip or groin region. Other joints appeared normal and no significant gait abnormalities were noted. White blood cell, erythrocyte sedimentation rate, and C-reactive protein values were within normal limits.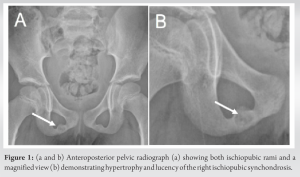
Anteroposterior radiographs of the pelvis revealed asymmetric hypertrophy and lucency of the right IPS relative to the left (Fig. 1a and b). Magnetic resonance imaging of the pelvis revealed mild-to-moderate intensity marrow edema and mild hypertrophic changes of the right IPS relative to the left, consistent with SIS (Fig. 2).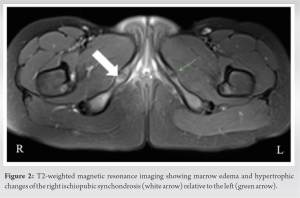
The patient was managed conservatively by a pediatric orthopedist. She was started on a course of non-steroidal anti-inflammatory therapy for 2–3 weeks and prescribed crutches to encourage non-weight-bearing to partial weight-bearing walking. The patient and her parent gave consent for the release of information including medical history, imaging, laboratory results, and follow-up visits related to this case for use in this case report.
Hip pain in the pediatric population can be difficult to diagnose due to a variety of pathologies that can present with non-specific symptoms and similar appearance in diagnostic imaging. Some of the most common causes of pain include stress fractures, transient synovitis, septic arthritis or osteomyelitis, slipped epiphysis, Perthes disease, and bone tumors [7]. Distinction among these causes is vital to ensure proper treatment early on and avoid unnecessary, potentially invasive interventions. The IPS is a temporary joint of childhood that occurs during the normal development of the skeleton. Through the process of ossification, the IPS begins to thin until it obliterates on fusion of the ischium and pubis before puberty [8]. This normal process of ossification is typically asymptomatic. However, delayed ossification may lead to pain in the hip area, restriction of hip movement, or limp [9]. Odelberg and Van Neck first described swelling and demineralization of the IPS in symptomatic patients in 1923 and 1924, respectively [5,6]. In young children, enlargement of the IPS is typically observed bilaterally. This suggests that the process of fusion between ischium and pubis begins symmetrically on each side of the pelvis. However, in older children, unilateral enlargement of the synchondrosis as seen in SIS is more commonly observed before complete ossification of the IPS [10]. The literature suggests that delayed ossification of the IPS is due to asymmetric mechanical stresses acting on it. Herneth et al. described an association between unilateral enlargement of the IPS and foot dominance in children, proposing that the non-dominant, weight-bearing leg experiences increased ground reaction forces applied to it relative to the non-dominant, swinging leg [10]. Wait et al. proposed that SIS could be caused by excessive pull of the hamstring tendon on the ischial tuberosity [11]. Similarly, Duben described the susceptibility of the IPS to mechanical forces, suggesting that thickening of the IPS is due to callus formation in response to mechanical strain [12]. To the best of our knowledge, this is the first report of SIS in a competitive child gymnast. SIS follows a benign course. Treatment typically involves rest, avoidance of exercise and 2–3 weeks of non-steroidal anti-inflammatory therapy. Once ossification is complete, no deformity is observed in the IPS [13].
SIS or Van Neck-Odelberg disease is a rare cause of pelvic or hip pain in the pediatric population. Although it is benign in nature, it can be mistaken for other more serious pathologies, leading to delayed treatment and unnecessary invasive intervention. Stress fracture, osteomyelitis, post-traumatic osteolysis, and tumor should be ruled out to make a diagnosis of SIS.
Van Neck-Odelberg is a rare cause of pediatric hip pain that can mimic serious pathologies, including stress fracture, osteomyelitis, or tumor. The condition is so rare that sparse information exists about treatment and management. The ability to recognize this disease early allows for effective treatment and avoidance of unnecessary procedures.
References
- 1.Oliveira F. Differential diagnosis in painful ischiopubic synchondrosis (IPS): A case report. Iowa Orthop J 2010;30:195-200. [Google Scholar | PubMed]
- 2.Sandomenico C, Tamburrini O. Bilateral accessory ossification center of the ischio-pubic synchondrosis in a female infant. Follow-up for over a three year period. Pediatr Radiol 1981;10:233-6. [Google Scholar | PubMed]
- 3.Gregory LS, Jones LV, Amorosi NM. Assessing the fusion of the ischiopubic synchondrosis using predictive modeling. Clin Anat 2019;32:851-9. [Google Scholar | PubMed]
- 4.Macarini L, Lallo T, Milillo P, Muscarella S, Vinci R, Stoppino LP. Case report: Multimodality imaging of van neck-odelberg disease. Indian J Radiol Imaging 2011;21:107-10. [Google Scholar | PubMed]
- 5.Van Neck M. Osteochondritis of the pubis. Arch Franco Belg Chir 1924;27:238-40 . [Google Scholar | PubMed]
- 6.Odelberg A. Some cases of destruction in the ischium of doubtful etiology. Acta Chir Scand 1923;56:273-84. [Google Scholar | PubMed]
- 7.Houghton KM. Review for the generalist: Evaluation of pediatric hip pain. Pediatr Rheumatol Online J 2009;7:10. [Google Scholar | PubMed]
- 8.Chaudhari AP, Shah G, Patil SS, Ghodke AB, Kelkar SB. Van neck-odelberg disease: A rare case report. J Orthop Case Rep 2017;7:24-7. [Google Scholar | PubMed]
- 9.Camacho DA, Bernal P, Cifuentes L, Rivero O. Van neck-odelberg disease: A rare cause of pain in pediatric pelvis. World J Nucl Med 2020;19:435-7. [Google Scholar | PubMed]
- 10.Herneth AM, Philipp MO, Pretterklieber ML, Balassy C, Winkelbauer FW, Beaulieu CF. Asymmetric closure of ischiopubic synchondrosis in pediatric patients: Correlation with foot dominance. Am J Roentgenol 2004;182:361-5. [Google Scholar | PubMed]
- 11.Wait A, Gaskill T, Sarwar Z, Busch M. Van neck disease: Osteochondrosis of the ischiopubic synchondrosis. J Pediatr Orthop 2011;31:520-4. [Google Scholar | PubMed]
- 12.Duben W. Transformation zones in the infantile ischiopubic epiphysis and its significance in differential diagnosis. Chirurg 1950;21:148-52. [Google Scholar | PubMed]
- 13.Sabir N, Çakmak P, Yılmaz N, Yüksel S. Osteochondrosis of ischiopubic synchondrosis: Van neck-odelberg disease. J Pediatr 2021;229:307-8. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2025 Primary Pyogenic Abscess in an Immunocompetent Child: An Indian Perspective
February 1, 2025 Primary Pyogenic Abscess in an Immunocompetent Child: An Indian Perspective August 1, 2026 Bisphosphonate-Related Pathological Femoral Fracture in a Child with ACTG2-Related Intestinal Failure and Metabolic Bone Disease: A Case Report
August 1, 2026 Bisphosphonate-Related Pathological Femoral Fracture in a Child with ACTG2-Related Intestinal Failure and Metabolic Bone Disease: A Case Report August 1, 2026 Spiked Washer–Augmented Screw Fixation for Bilateral Tibial Tuberosity Avulsion Fractures in an Adolescent: A Case Report
August 1, 2026 Spiked Washer–Augmented Screw Fixation for Bilateral Tibial Tuberosity Avulsion Fractures in an Adolescent: A Case Report July 1, 2026 Concurrent Occurrence of Dysplasia Epiphysealis Hemimelica involving Lateral Malleolus and Sinus Tarsi: Rare Case with Review of Literature
July 1, 2026 Concurrent Occurrence of Dysplasia Epiphysealis Hemimelica involving Lateral Malleolus and Sinus Tarsi: Rare Case with Review of Literature