
The Allyane technic has been been decisive, used as a reprogramming method, to treat Chronic Ankle Instability (CAI) in this case report. Decreasing ankle muscle inhibition, stability, pliometry and ankle confidence improve.
PT. Jean-Baptiste Colombié, Department of Orthopaedic, Gare du Midi, Biarritz, France. E-mail: jbc.kine@gmail.com
Abstract
Introduction: The treatment of chronic ankle instability (CAI) is quite long and problematic. In dance, about 53% of dancers have CAI. CAI is a major cause of musculoskeletal disorders such as sprains, posterior ankle impingement, and shin splints. Moreover, CAI leads to a loss of confidence and becomes a key factor for reducing or stopping dance. This case report assesses the effectiveness of the Allyane technique on CAI. Furthermore, it provides a better understanding of this pathology. The Allyane process is a neuromuscular reprogramming method based on the scientific background of neuroscience. Its aim is to strongly activate the afferent pathways of the reticular formation, responsible for voluntary motor learning. It uses mental skill imagery, afferent kinaesthetic sensations, and specific sequences of low-frequency sounds coming from a patented medical device.
Case Report: A. Is a 15-year-old female dancer who practices ballet 8 h per week. She has suffered from CAI for 3 years, with repeated sprains as well as a loss in confidence, with a direct implication on her career. Despite physiotherapy rehabilitation, her CAI tests were still deficient and she still felt strongly apprehensive while dancing.
Conclusion: After 2 h of the Allyane technique, we notice a 195% gain of strength of the peroneus, 266% for the posterior tibialis, and 141% for the anterior tibialis muscles. Side hop test and the functional test (Cumberland Ankle Instability tool) normalized. 6 week later, the control assessment confirms this screening and gibes an idea of the durability of the technic. This neuroreprogramming method could not only open the door to interesting perspectives in the treatment of CAI, but it can also help in the understanding of this pathology in case of central muscle inhibitions.
Keywords: Chronic ankle instability, dance, neuromuscular reprogramming method, Allyane.
In dance, the ability to perform esthetic movement requires optimal reflex stability. Chronic ankle instability (CAI) is common in dance: About 53% of pre professional dancers have CAI [1,2]. This is due to multifactorial causes, as well as depending on reflex motricity and motor inhibition [3]. For dancers, CAI is a major cause of pathologies like foot or ankle sprains, posterior ankle impingement, and shin splints. Moreover, instability increases lack of confidence and becomes a key factor for reducing or stopping dance [4]. The discovery of muscular inhibitions has been a major step in the understanding of CAI. A lot of neuromuscular reprogramming methods (NMRm) have been developed over the last 20 years. They are based on multi afference motor learning (visual, proprioceptive, mental visualization, and kinetic, goals) and are described with different protocols [5,6,7,8,9]. Their first point in common is their long integration time (between 4 and 15 months) which is quite an important inefficiency factor. For a dancer, a 20-min-long protocol per day, along with having to constantly maintain voluntary control while dancing for a period of 6 months is quite difficult. The second point in common is the use of mental motor imagery, whose results are known both in dance and sports [10,11]. At the Malandain Ballet Biarritz, we discovered that the Allyane method thanks to dancers, who were treated for different chronic pathologies related to joint instability. An only one session of this method seemed to be necessary to modify the reflex motor pattern (RMP), that is why we have been interested first in this treatment. Moreover, dancer population can smartly understand and analyze its movements and ready to use new methods to improve faster its technique. Interested, but sceptical about the lack of scientific studies, we decided to evaluate this technique for CAI. This case report is the pilot protocol of a larger and cohort study. The Allyane process is a NMRm based on the scientific background of neuroscience [12]. Its principle is to strongly activate the afferent pathway of the reticulated formation, responsible for voluntary motor learning [13,14,15]. Developed 13 years ago by athletic trainers for tennis players, this method has been used by health professionals for 3 years. The process is composed of three phases: Screening, erasing, and reprogramming. It uses mental skill imagery, afferent proprioceptive information (sensations, kinesthetics, intentions, and feelings), and low-frequency sounds (LFS).
A. is a 15-year-old female dancer. She has practiced ballet since the age of 4 and is currently in a pre-professional program. In 2016, she began to suffer from repeated ankle sprains on her two feet and was treated with four standard physiotherapy treatments of 10 sessions. She practiced protocols for muscle strengthening and followed an advanced proprioception program. We also tried to change her motor patterns using traditional methods: By trying to understand and perceive her movements with an evolutive protocol of exercises ranging from analytic to global and finally to dancing movements. She also benefited from five osteopathy sessions and a 3-month reconditioning program. She was in therapeutic failure, and the surgeon to whom she was addressed refused to operate because she had no mechanical instability. We decided to analyze very precisely its dancing movements.It became clear that she was in trouble with instability when she was no longer focusing on her ankle, certainly preferring to think of her choreography. We conclude, we had to change the reflex stability of her ankle. We choose the Allyane technique because of its speed but also because the other methods seemed to be too similar of the techniques, we use the last months. When we decided to treat A with the Allyane technique, we first performed an orthopedic screening.
She was still dancing but with a lot of difficulty and stress, feeling unbalanced,
-
- Pain and joints: Her ankle was painless, without a limited range of motion. She had no mechanical instability, clinically diagnosed with a negative anterior talar tilt test
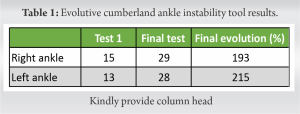
- Functional impairment: Evaluated with the cumberland ankle instability tool (CAIT) for its specificity on CAI. The diagnostic score was 24.5 [15] Her CAIT was 13/30 for the left ankle and 15/30 for the right one (cf. Table 1)
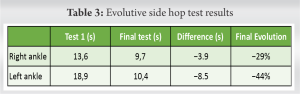
- Dynamic balance was evaluated with the Side hop test and the modified star excursion balance test (SEBTm) [16]. To perform 10 side hop jumps, A. needed 13.6s on her left leg and 18.9s on her right, while the limiting standard is to perform below 12.4s [17]
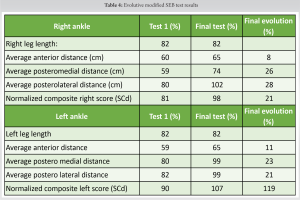
- At the modified SEBTm, as the two ankles were involved, we did not consider the reach difference between the right and left sides. However, we considered the normalized composite reach distance (SCd). In theory, we consider that the pathogenic level is below 94% [16]. We found a 91% high score on the right leg and a 90% for the left leg.
Performing the modified SEBTm, as the two ankles were involved, we did not consider the reach difference between the right and left sides. However, we considered the normalized composite reach distance (SCd). In theory, we consider that the pathogenic limit is below 94% [16]. We found a 91% score on the right leg and a 90% for the left leg.
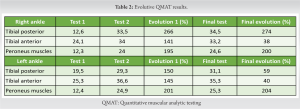
- Muscular screening: To measure muscle inhibitions analytically, quantitative analytical muscle testing was performed with a microfet2. We use a classical method: One guided passive movement to understand the aim, one active movement without strength to check the proper understanding of the exercise, and a last try with a maximal concentric, 3s isometric and eccentric contraction. Only the maximum force measurement, the peak force was noted.
- There was a difference of 12 kg between the maximum peroneus (P) and tibial anterior (TA) strength. This is a difference ratio of 2 while scientific literature matches a Tibial Posterior muscle/Peroneus muscles (TP/P) ratio of 1,1.
Allyane technique strategy
The aim of the treatment was to reactivate the Peroneus muscles, then to coordinate ankle balance using peroneus muscles, tibialis anterior and posterior muscles with a good plantar tonus. Those patterns going into the one-foot position, the jump impulse, and the jump reception.
Allyane technique description
The Allyane technique begins with the precise analysis of the pathogenic RMP and the new one. We worked to feel the effect of the P, the TA, and TP muscles on the ankle. What external and internal stabilization it allowed, how the ankle seemed to be attracted at the top, forward, and in turn out. We worked in one-foot balance position, in parallel then in turn out. In a second time, we worked to analyze the jump impulse and the jump landing. Each RMP we described, A. was asked to build mental imagery of the posture, motion. Listening the LFS. The second step included an erasing phase of the pathogenic RMP. It allowed a new pattern to be built without conflict with the pathogenic one. We asked A. to visualize her whole body, including her pathogenic RMP, then to mentally erase her feet up to her hips. We triggered the associated sound at her signal. In a 3rd time, still using mental imagery accompanied by low frequencies sounds, we asked A. to remember her mental imagering of the corrected RMP described earlier, starting with the analytic correction of global movement and feeling. In each key point, we triggered the associated sound at her signal. At the end of this reprogramming phase, A. physically checked her reflex correction. We asked her if she felled a difference, performing the three postures. If this difference was spontaneous, reflex, or voluntary. A. answered that she felled a changing, being more balanced. The last phase served to strengthen the new RMP: During 15 min, we asked A. to visualize everyday motions with her new RMP feeling. This serves to activate it in a larger motion range. After the 2 h of the Allyane technique, A. had to physically activate her new RMP: Dancing without thinking about his new RMP.
Second evaluation
At the end of the 2-h long Allyane process, we implemented a second screening.
-
- The Quantitative muscular analytic testing (QMAT) showed an average increase of 183% of the muscles’ strengths. The peroneus muscles strength increased by 198%, the right TP by 266%
- The Tibialis anterior /Peroneus muscle strength ratio became more balanced: from 2 to 1 (cf. Table 2).
This QMAT quantified how much the muscular inhibition has been improved. After the Allyane process, A. returned back to her normal life as a dancer, without the need for physiotherapy, strengthening, or proprioceptive program.
Final evaluation
6 weeks later, we performed the same screening:
-
- The new ankle stability of A. permitted her to progress in her technique and gain confidence. She can now train normally without feelings of instability
- The final CAIT score was 28 for the left ankle and 29 for the right one. An average gain of 204% (cf. Table 1)
- The side hop test increased by +160% (cf, Table 3). A. realized 10 jumps under 12.4s
-
- The QMAT average gain was +186%, the muscles’ strengths increased by 3% after the allyane process. (cf. Table 2)
- At the SEBTm we found a 107% high SCd. Hence, an average increase of 118%. The SCd score was higher than the 94% pathogenic level (cf. Table 4).
This case report is the first to show the effectiveness of the Allyane technique. Further studies including more patients in a prospective design are necessary to present a stronger level of evidence. It is important to recall that his technique cannot be used alone. A first work of physiotherapy and ostheopathy is necessary before considering the reflects motor pattern. Nevertheless, compared to other neuromotor or programming methods, the speed and simplicity of the Allyane technique seem to be decisive.
After the use of the Allyane method, we observed a significant modification of the ankles’ stability. The QMAT evolution showed a positive effect on muscular inhibition. The side hop test and the CAIT revealed that the ankles were functionally stable. After 6 weeks, the results had not changed. From this, we can conclude the sustainability of the results. The CAIT objectified a functional gain in dancing. A. was dancing normally, increasing her technique with confidence. She no longer needed care, strengthening, or proprioceptive protocols anymore. For this particular case of dancer’s CAI, using the Allyane process has been effective. We have to submit it on a larger cohort study to know if the benefits can be extended to a larger population.
Allyane method seems to be helpful in the treatment of CAI, working on muscular inhibitions and changing the RMP.
References
- 1.Simon J, Hall E, Docherty C. Prevalence of chronic ankle instability and associated symptoms in university dance majors: An exploratory study. J Dance Med Sci 2014;18:178-84. [Google Scholar | PubMed]
- 2.Gribble PA, Bleakley CM, Caulfield BM, Docherty CL, Fourchet F, Fong DT. 2016 consensus statement of the International Ankle Consortium: Prevalence, impact and long-term consequences of lateral ankle sprains. Br J Sports Med 2016;50:1493-5. [Google Scholar | PubMed]
- 3.Hertel J, Corbett RO. An updated model of chronic ankle instability. J Athletic Train 2019;54:572-88. [Google Scholar | PubMed]
- 4.O’Loughlin PF, Hodgkins CW, Kennedy JG. Ankle sprains and instability in dancers. Clin Sports Med 2008;27:247-62. [Google Scholar | PubMed]
- 5.Porrill J, Dean P. Cerebellar motor learning: When is cortical plasticity not enough? PLoS Comput Biol 2007;3:1935-50. [Google Scholar | PubMed]
- 6.Kermarrec G. Stratégies D’apprentissage et Autorégulation. Revue de Question dans le Domaine des Habiletés Sportives. Movement Sport Sciences; 2004. Available from: https://www.academia.edu. [Google Scholar | PubMed]
- 7.Hignet R. Sensorimotor reprogramming concepts and principles. Kinésithérapie, la revue 2012;12:23-8. [Google Scholar | PubMed]
- 8.Smarandache CR, Daur N, Hedrich UB, Stein W. Regulation of motor pattern frequency by reversals in proprioceptive feedback. Eur J Neurosci 2008;28:460-74. [Google Scholar | PubMed]
- 9.Lucca LF. Virtual reality and motor rehabilitation of the upper limb after stroke: A generation of progress? J Rehabil Med 2009;41:1003-6. [Google Scholar | PubMed]
- 10.Coker E, McIsaac TL, Nilsen D. Motor imagery modality in expert dancers: An investigation of hip and pelvis kinematics in demi-plié and sauté. J Dance Med Sci 2015;19:63-9. [Google Scholar | PubMed]
- 11.Oishi K, Maeshima T. Autonomic nervous system activities during motor imagery in elite athletes. J Clin Neurophysiol 2004;21:170-9. [Google Scholar | PubMed]
- 12.Friggeri A, Le Blay G. Reprogrammation Neuro-Cognitive reprogrammation in orthopedic mecanic pathologies with the allyane method.. Cahiers de la SOFMMOO; 2018. [Google Scholar | PubMed]
- 13.Apps R, Lee S. Central regulation of cerebellar climbing fibre input during motor learning. J Physiol 2002;541:301-17. [Google Scholar | PubMed]
- 14.Weicker H, Kinsherf R, Diserens K, Deigner HP, Struder H. Physiology and pathophysiology of basalganglia: Impact on motor system function. Eur J Sport Sci 2001;1:1-46. [Google Scholar | PubMed]
- 15.Geerinck A, Beaudart C, Salvan Q, Van Beveren J, D’Hooghe P, Bruyère O, et al. French translation and validation of the Cumberland Ankle Instability Tool, an instrument for measuring functional ankle instability. Foot Ankle Surg 2020;26:391-7. [Google Scholar | PubMed]
- 16.Rosen AB, Needle AR, Ko J. Ability of functional performance tests to identify individuals with chronic ankle instability: A systematic review with meta-analysis. Clin J Sport Med 2019;29:509-22. [Google Scholar | PubMed]
- 17.Hall EA, Chomistek AK, Kingma JJ, Docherty CL. Balance-and strength-training protocols to improve chronic ankle instability deficits, Part I: Assessing clinical outcome measures. J Athl Train 2018;53:568-77. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Functional Outcomes of All-Inside Arthroscopic Repair for Chronic Ankle Instability in Adolescents: A Case Series
June 1, 2026 Functional Outcomes of All-Inside Arthroscopic Repair for Chronic Ankle Instability in Adolescents: A Case Series January 1, 2026 A Prospective Comparative Study of the Outcome of Diaphyseal Humeral Shaft Fractures with Anterior BridgePlating versus Open Reduction Internal Fixation by Dynamic Compression Plating
January 1, 2026 A Prospective Comparative Study of the Outcome of Diaphyseal Humeral Shaft Fractures with Anterior BridgePlating versus Open Reduction Internal Fixation by Dynamic Compression Plating December 1, 2024 Metacarpophalangeal Joint Dislocations Two Cases, Two Stories
December 1, 2024 Metacarpophalangeal Joint Dislocations Two Cases, Two Stories May 1, 2026 Combined Post-operative Denosumab and Oral Bisphosphonate Therapy Following Resection of Spinal Giant Cell Tumor: A Case Report
May 1, 2026 Combined Post-operative Denosumab and Oral Bisphosphonate Therapy Following Resection of Spinal Giant Cell Tumor: A Case Report