
This article presents a new technique of treating subluxation of biceps femoris tendon around the knee joint by rerouting of the subluxating superior aspect of the tendon without further dissection and release as long as no anatomic variants are present.
Dr. Georgio Nahed, Department of Orthopaedic and Trauma Surgery, Aboujaoude Hospital, Jal El Dib, Beirut, Lebanon. E-mail: georgionahed6@gmail.com
Abstract
Introduction: Snapping biceps femoris tendon over the fibular head is an uncommon cause of snapping knee. We report a rare case of knee pain secondary to subluxation of the long head of the biceps femoris over the fibular head in an athlete with no history of trauma. This case was treated surgically by a modification of Kennedy procedure.
Case Report: A 21-year-old Lebanese athletic male presented for a nauseating feeling of something snapping over his lateral knee since the age of 12 when performing self-defense sports with no history of trauma. Snapping begins when the patient flexes above 80° during squatting, cycling, gym exercises, and climbing stairs.
Conclusion: A symptomatic snapping biceps femoris tendon is a rare phenomenon with limited reports in the literature. When conservative treatment fails, surgery may be the only successful treatment. A modification of the Kennedy procedure was used. Rerouting of the subluxating superior aspect of the tendon without further dissection and release appears to be an effective treatment that can result in symptom resolution as long as no anatomic variants are present.
Keywords: Snapping knee, biceps femoris subluxation, athlete.
Snapping of tendons around joints is well described in the literature. However, this is a rare phenomenon to occur around the knee joint [1]. Snapping biceps femoris tendon over the fibular head is an uncommon cause of snapping knee. This muscle has a distal insertion over the fibular head, proximal tibia, and the crural fascia [2]. Clinical reports of lateral knee pain caused by tendon subluxation have seldom been reported in the literature. Snapping knee due to the biceps femoris tendon can be caused by tendon injury, various anatomical pathologies, and fibular head deformity [3].
We report a rare case of knee pain secondary to subluxation of the long head of the biceps femoris over the fibular head in an athlete with no history of trauma.
A 21-year-old athletic male presented to our orthopedic clinic, 2 years before being operated, for a pain-free snapping left lateral knee. He reported a nauseating feeling of something snapping over his lateral knee since the age of 12 when performing self-defense sports with no history of trauma. This snapping begins when the patient flexes his knee above 80° during squatting, cycling, gym exercises, and climbing stairs.
On physical examination, the patient had full range of motion, no joint line tenderness, and a stable ligamentous examination. He has a visible, palpable, and audible subluxation of the biceps femoris tendon over the fibular head when flexing his knee above 80°. This subluxation was exacerbated by internal rotation of the tibia but not relieved by manual compression of the posterolateral thigh. No tenderness was noted over the fibular head. Subluxation was present with passive flexion of the knee above 80°. No fibular head difference was noted in comparison with the contralateral knee (See additional file 1: Video 1).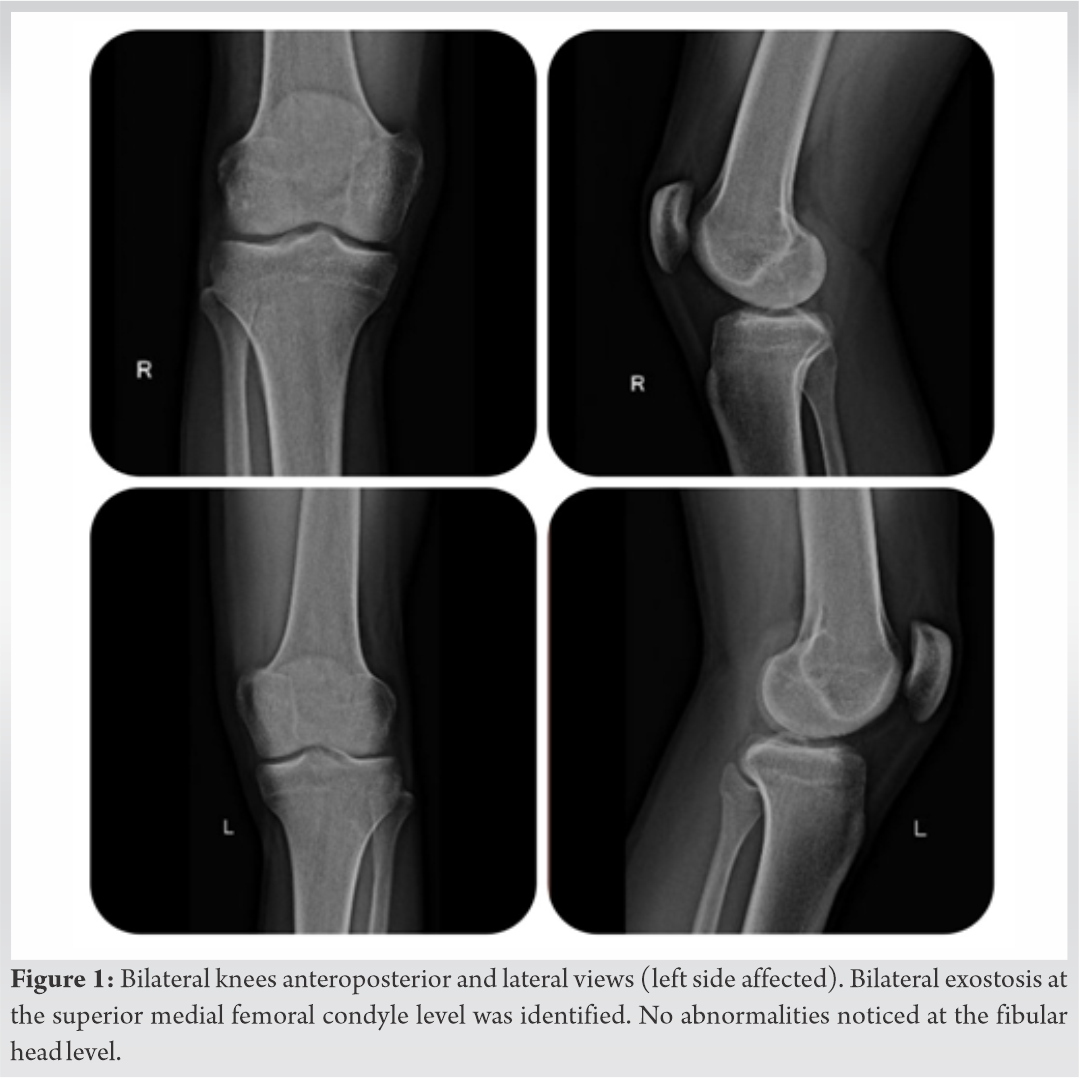
The patient was diagnosed with snapping biceps femoris syndrome. Conservative treatment with rest, anti-inflammatory medications, and hamstring stretching was unsuccessful.
The patient was seen again in our clinic. Recently, local pain was present after repetitive snapping.
Anteroposterior and lateral comparative radiographs of both knees showed no fibular head prominence (Fig. 1). Magnetic resonance imaging showed no anomaly of biceps femoris insertion.
Real-time sonography demonstrated superior fibers of the biceps femoris tendon slipping over the fibular head (See additional file 2: Video 2).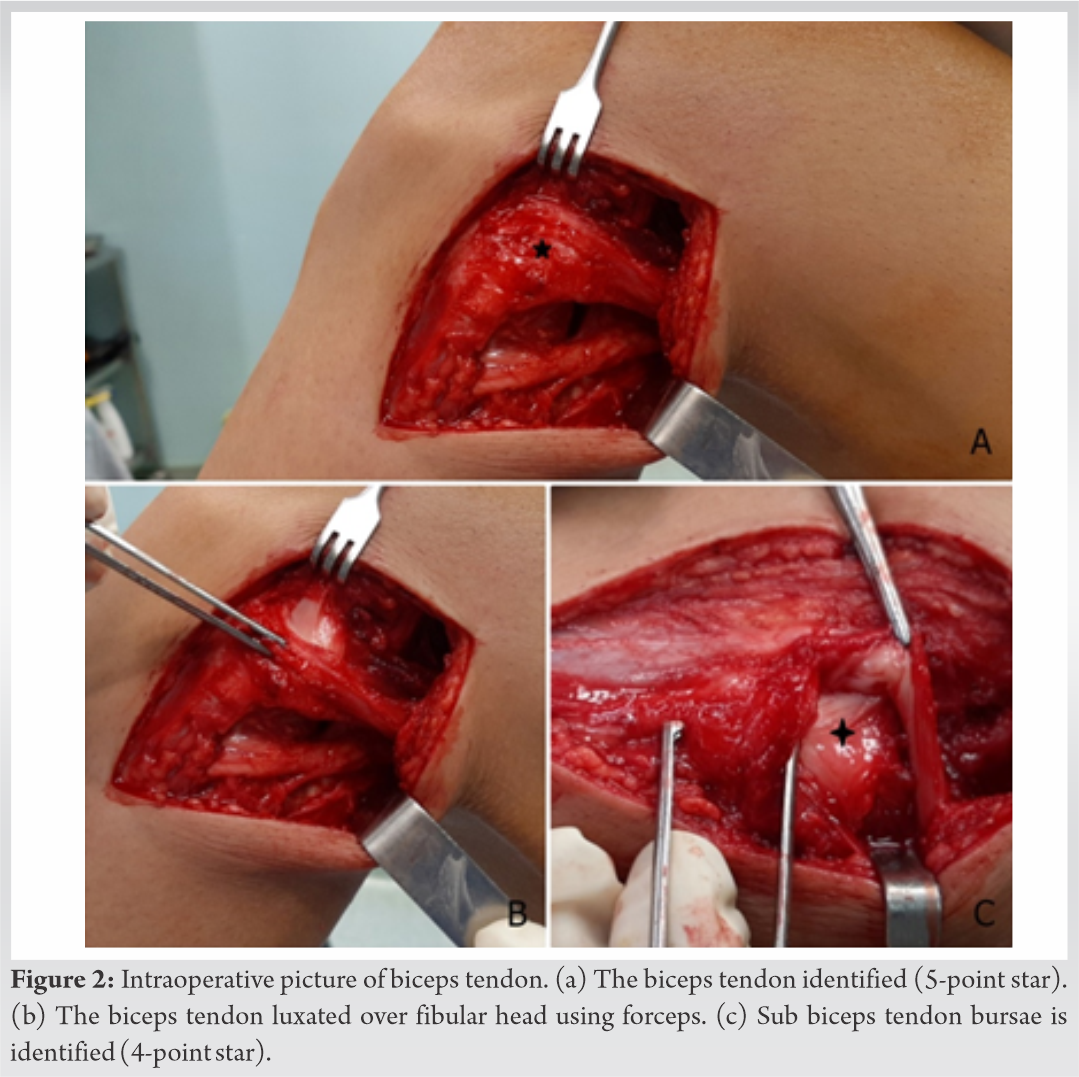
Our patient was then scheduled for operative exploration.
Patient positioning
The patient is positioned supine on the operating table. Examination under spinal anesthesia is performed to confirm the diagnosis. A well-padded tourniquet is placed on the upper thigh of the operative leg, which is then prepared and draped in a standard fashion. The tourniquet is not inflated.
Surgical approach
A lateral hockey-stick skin incision is made along the iliotibial band and extended distally, halfway between the fibular head and Gerdy tubercle. The subcutaneous tissue is dissected. Dissection between the biceps femoris and iliotibial band is done. The long and short heads of the biceps femoris are exposed (Fig. 2).
Common peroneal nerve (CPN) neurolysis is, then, performed. The nerve courses from the posterolateral side of the knee around the biceps femoris tendon and the fibular head to the anterolateral side of the lower leg. Distally, about 1 cm of peroneus longus fascia is incised over the CPN to prevent nerve irritation or a foot drop due to post-operative swelling.
Two arms of the biceps femoris are identified (tibial and fibular arms). Biceps femoris snapping is checked with passive flexion and internal rotation of the knee. The tibial arm was subluxating over the fibular head when flexing (See additional file 3: Video 3). A bursa at this location is seen and may be explained by the mechanism of subluxation of the biceps tendon over time (Fig. 2).
Excision of the bursa is done. The subcortical bone is exposed from the apex of the posterolateral fibular styloid down to the lateral aspect of the fibular head. One anchor (Smith and Nephew/Twinfix 3.5 mm) is inserted over the posterolateral fibular head 1cm below the tip of the styloid. The superior tibial arm is rerouted underneath the fibular head and tied through the anchor without release of its insertion on the anterolateral tibia. This is done in FULL EXTENSION (Fig. 3).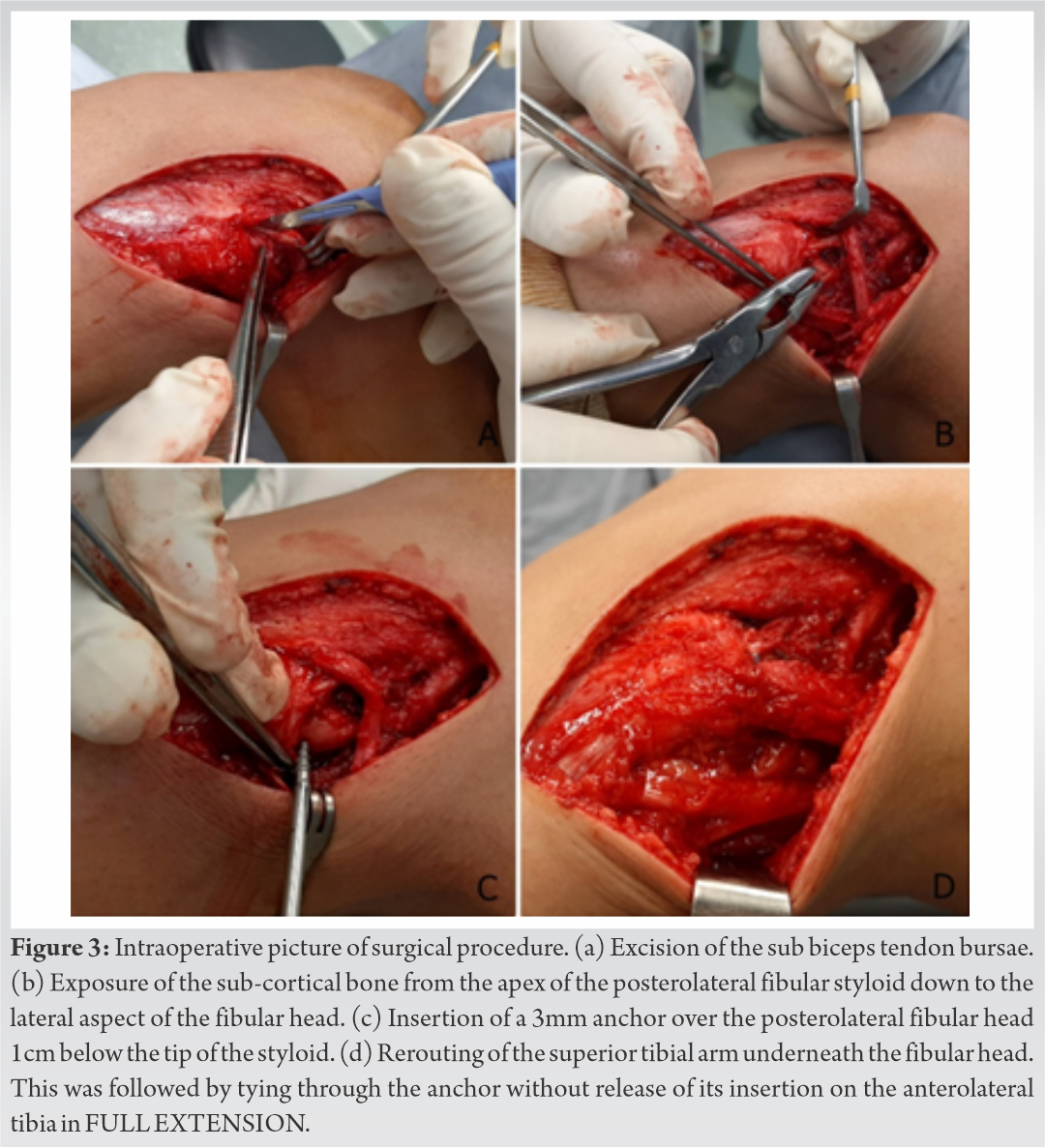
After rerouting, flexion and internal rotation of the knee is done with no evidence of biceps femoris snapping (Video 4).
After irrigation of the tissues, the superficial layers are closed in a regular fashion using interrupted subcutaneous skin sutures in the deep dermal layers. The skin is closed with nylon 3-0 interrupted horizontal matrix sutures. No drain is inserted. The patient was discharged the next day.
Rehabilitation protocol
No knee immobilizer is used. The patient is limited to weight bearing over 6 weeks with no active knee flexion. Two weeks post-operation, physical therapy is initiated with limitation to passive flexion (0–90°) and isometric contraction of the quadriceps at 15° of flexion. The patient returned to normal sport activity starting 6 months post-operation.
Follow-up
The patient was seen after 6 months in our clinics. Normal range of motion of the knee was noted. Knee flexion beyond 90° was performed pain free with no visible or audible biceps femoris subluxation. Return to normal physical activity was noted.
Snapping usually results from the sudden displacement of an anatomic or pathologic structure during the movement of a joint. Snapping knee has many intra and extra-articular etiologies. Extra-articular etiologies comprise snapping biceps femoris tendon, snapping Popliteus tendon, iliotibial band friction, patellar tendon–lateral femoral condyle friction, snapping pes anserinus, and snapping popliteal recess. Intra-articular causes include snapping meniscus, snapping plica, tumors, or intra-articular bodies. Snapping knee can also occur in total knee replacement patients [4].
Snapping biceps femoris tendon syndrome is an uncommon entity in snapping knee. Several previous case reports described this phenomenon. Biceps femoris tendon syndrome has been found to be due to anomalous insertion of the long head of the biceps femoris tendon [1,3,5,6,7,8,9,10,11,12,13,14], fibular head deformity [15,16,17,18], tendon injury [19,20], and normal anatomy without trauma [21,22].
Fritsch and Mhaskar and Hernandez et al. described an abnormal anterior insertion on proximal tibia, where the tendon was rerouted through a tunnel in the fibular head [5,6]. Lokiec et al. described an abnormal tendon insertion and a technique of releasing and repositioning only the irregular part of the tendon to its correct insertion [1]. Bagchi and Grelsamer and Kristen et al. described abnormal anterior insertion on proximal tibia treated by partial fibular head resection. [7,9] Date et al., Matar and Farrar, Kissenberth and Wilckens, Kennedy et al., and Reid and Mofidi described abnormal insertion of the biceps femoris treated by release and reinsertion of the tendon in the fibular head [3,8,11,13,14]. Ernat and Galvin described abnormal anterior insertion on proximal tibia and thickened anterolateral fibular insertion treated only with release of the abnormal tendon insertion [10]. Saltzman et al. described two cases of abnormal insertion onto proximal anterolateral tibia treated by reinsertion of anomalous tendon to fibular head with pie crust lengthening [12]. McNulty et al., Fung et al., Bach et al., and Hadeed et al. showed cases with normal tendon anatomy and prominent fibular head, where treatment consisted of partial fibular head excision [15,16,17,18]. Crow et al. and Vavalle and Capozzi described cases with normal biceps femoris attachment and fibular head anatomy. Crow et al. treated their case with the release of subluxating tendon; however, Vavalle and Capozzi treated it with resection of posterior fibular head [21,22]. Bansal et al. described a case of snapping of biceps femoris due to injury to the long head and was treated by tendon rerouting through a tunnel in fibular head [19].
There is no consensus regarding the most appropriate surgical technique. In most cases, surgical techniques used were dependent on intraoperative findings. In our case, as in the cases of Crow et al. and Vavalle and Capozzi, no abnormal anatomy in relation to tendon anatomy or fibular head was found, as evident in imaging studies and intraoperatively. Only the superior portion of the tendon was subluxating over the fibular head. Our surgical procedure was a modification of Kennedy’s technique [13]. It included no tendon release with rerouting of the superior portion to a position inferior to the fibular head using one anchor seated 1 cm inferior to the tip of the styloid and on the posterolateral portion of the fibula. The success of this procedure was confirmed intraoperatively.
In several previous reports of non-traumatic snapping biceps femoris tendons, the snapping was noted bilateral. Interestingly, in our case, it was present unilaterally.
Initially, our patient complained of pain-free snapping during sports, where knee flexion is necessary. Recently, repetitive snapping caused pain with annoyance during sports. As mentioned by Vavalle and Capozzi, this progression can be explained by progressive tendon stiffness with training.
A symptomatic snapping biceps femoris tendon is an unusual phenomenon with limited reports in the literature. When conservative treatment fails, surgery may be the only successful treatment. Using a modification of Kennedy’s procedure, where rerouting of the subluxating superior aspect of the tendon with no further dissection or release, appears to be an effective treatment that can result in symptom resolution as long as no anatomic variants are present.
This case report presents a modification of Kennedy’s procedure for treating biceps femoris subluxation over the fibula. It consists of rerouting of the subluxating superior aspect of the tendon without further dissection or release as long as no anatomic variants are present.
References
- 1.Lokiec F, Velkes S, Schindler A, Pritsch M. The snapping biceps femoris syndrome. Clin Orthop Relat Res 1992;(283):205-6. [Google Scholar | PubMed]
- 2.Guenoun D, Champsaur P, Coudreuse JM, Cucurulo T, Lagier A, Le Corroller T. A Symptomatic Anomalous Biceps Femoris Tendon Insertion. Netherland: Elsevier; 2016. p. 113-5. [Google Scholar | PubMed]
- 3.Date H, Hayakawa K, Nakagawa K, Yamada H. Snapping knee due to the biceps femoris tendon treated with repositioning of the anomalous tibial insertion. Knee Surg Sports Traumatol Arthrosc 2012;20:1581-3. [Google Scholar | PubMed]
- 4.Marchand AJ, Proisy M, Ropars M, Cohen M, Duvauferrier R, Guillin R. Snapping knee: Imaging findings with an emphasis on dynamic sonography. AJR Am J Roentgenol 2012;199:142-50. [Google Scholar | PubMed]
- 5.Fritsch BA, Mhaskar V. Anomalous biceps femoris tendon insertion leading to a snapping knee in a young male. Knee Surg Relat Res 2017;29:144-9. [Google Scholar | PubMed]
- 6.Hernandez JA, Rius M, Noonan KJ. Snapping knee from anomalous biceps femoris tendon insertion: A case report. Iowa Orthop J 1996;16:161. [Google Scholar | PubMed]
- 7.Kristensen G, Nielsen K, Blyme PJ. Snapping knee from biceps femoris tendon. A case report. Acta orthop Scand 1989;60:621. [Google Scholar | PubMed]
- 8.Matar HE, Farrar NG. Snapping biceps femoris: Clinical demonstration and operative technique. Ann R Coll Surg Engl 2018;100:59-61. [Google Scholar | PubMed]
- 9.Bagchi K, Grelsamer RP. Partial fibular head resection for bilateral snapping biceps femoris tendon. Orthopedics 2003;26:1147-9. [Google Scholar | PubMed]
- 10.Ernat JJ, Galvin JW. Snapping biceps femoris tendon. Am J Orthop 2018;47(7) [Google Scholar | PubMed]
- 11.Kissenberth MJ, Wilckens JH. The snapping biceps femoris tendon. Am J Knee Surg 2000;13:25-8. [Google Scholar | PubMed]
- 12.Saltzman BM, Collins MJ, Arns TA, Forsythe B. Unilateral snapping biceps femoris tendon with an anomalous insertion treated with anatomic repositioning and lengthening with a single suture anchor: A report of two cases. JBJS Case Connect 2018;8:13. [Google Scholar | PubMed]
- 13.Kennedy MI, DePhillipo NN, Chahla J, Armstrong C, Ziegler CG, Buckley PS, et al. Surgical repair of dynamic snapping biceps femoris tendon. Arthrosc Tech 2018;7:1129-33. [Google Scholar | PubMed]
- 14.Mofidi A, Mofidi A. Bilateral snapping biceps femoris tendon: A case report and review of the literature. Eur J Orthop Surg Traumatol 2019;29:1081-7. [Google Scholar | PubMed]
- 15.McNulty M, Carreau J, Hendrickson N, Bollier M. Case report: Snapping biceps femoris tendon due to abnormal fibular morphology. Iowa Orthop J 2017;37:81. [Google Scholar | PubMed]
- 16.Fung DA, Frey S, Markbreiter L. Bilateral symptomatic snapping biceps femoris tendon due to fibular exostosis. J Knee Surg 2008;21:55-7. [Google Scholar | PubMed]
- 17.Bach BR, Minihane K. Subluxating biceps femoris tendon: An unusual case of lateral knee pain in a soccer athlete. Am J Sports Med 2001;29:93-5. [Google Scholar | PubMed]
- 18.Hadeed MM, Post M, Werner BC. Partial fibular head resection technique for snapping biceps femoris. Arthrosc Tech 2018;7:859-62. [Google Scholar | PubMed]
- 19.Bansal R, Taylor C, Pimpalnerkar AL. Snapping knee: An unusual biceps femoris tendon injury. Knee 2005;12:458-60. [Google Scholar | PubMed]
- 20.Bernhardson AS, LaPrade RF. Snapping biceps femoris tendon treated with an anatomic repair. Knee Surg Sports Traumatol Arthrosc 2010;18:1110-2. [Google Scholar | PubMed]
- 21.Crow SA, Quach T, McAllister DR. Partial tendon release for treatment of a symptomatic snapping biceps femoris tendon: A case report. Sports Health 2009;1:435-7. [Google Scholar | PubMed]
- 22.Vavalle G, Capozzi M. Symptomatic snapping knee from biceps femoris tendon subluxation: An unusual case of lateral pain in a marathon runner. J Orthop Traumatol 2010;11:263-6. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 April 20, 2015 Arthroscopy Assisted Percutaneous Fixation of Ideberg Type Iii Glenoid Fractures
April 20, 2015 Arthroscopy Assisted Percutaneous Fixation of Ideberg Type Iii Glenoid Fractures October 10, 2021 Open Reduction and Internal Fixation of a Pediatric Talar Body Fracture using a Medial Malleolar Osteotomy – A Case Report
October 10, 2021 Open Reduction and Internal Fixation of a Pediatric Talar Body Fracture using a Medial Malleolar Osteotomy – A Case Report June 1, 2026 A Rare Neglected Ipsilateral Humeral Triad: Comminuted Proximal Humerus Nonunion with Avascular Necrosis, Mid-Shaft Fracture, and High Radial Nerve Palsy Managed with Staged Reconstruction
June 1, 2026 A Rare Neglected Ipsilateral Humeral Triad: Comminuted Proximal Humerus Nonunion with Avascular Necrosis, Mid-Shaft Fracture, and High Radial Nerve Palsy Managed with Staged Reconstruction February 1, 2026 Functional and Radiological Outcomes of Proximal Femoral Nailing in Unstable Peritrochanteric Fractures: A Prospective Observational Study
February 1, 2026 Functional and Radiological Outcomes of Proximal Femoral Nailing in Unstable Peritrochanteric Fractures: A Prospective Observational Study