
When highly active individuals such as military personnel present with non-traumatic common peroneal palsy, patients should be evaluated for chronic exertional compartment syndrome. Such patients require a combined surgical treatment with nerve decompression and compartment release for successful outcome instead of nerve decompression alone.
Dr. Prashant Meshram, Orthocure Medical Center, Mirdif Avenue Mall, Mirdif, Dubai, United Arab Emirates. E-mail: drmeshramortho@gmail.com
Introduction: The common peroneal nerve (CPN) palsy in military personnel due to chronic exertional compartment syndrome (CECS) is uncommon. There are no previous reports of treatment of this condition with simultaneous CPN and superficial peroneal nerve (SPN) neurolysis and compartment release.
Case Report: An 18-year-old military recruit presented with complete CPN palsy after sitting cross-legged for 2 h in training. After 3 months of failed non-operative treatment, a clinical diagnosis of CECS with CPN palsy was made and the patient was treated with simultaneous CPN and SPN neurolysis and release of the anterior and lateral leg compartments. The patient had full recovery at 6 months post-operative period and returned to sports at 1 year follow-up.
Conclusion: This case report of a young military recruit with CPN palsy after prolonged cross-legged sitting in the setting of CECS demonstrates successful treatment with simultaneous CPN and SPN neurolysis and anterior and lateral compartment release. Future studies should explore the efficacy of this treatment option and prevention strategies of CPN palsy in military personnel.
Keywords: Penoreal, palsy, compartment syndrome, chronic exertional compartment syndrome, military, surgery.
The common peroneal nerve (CPN) is the most common peripheral nerve injury of the lower extremity and injury is most susceptible when the nerve crosses the fibular head [1,2]. While CPN palsy most occurs after traumatic injuries, non-traumatic compressive etiologies are not uncommon and include tight casts, sitting cross-legged, prolonged squatting, limb position during surgery causing nerve compression, bariatric surgery, and chronic compartment syndrome. Few studies have reported CPN palsy after prolonged squatting as a part of occupational requirements and treated successfully either with non-operative or operative treatment [3,4]. However, there are few reports of CPN palsy with chronic exertional compartment syndrome (CECS) presenting after prolonged sitting in cross-legged position as a part of military training. More research on CPN palsy in military personnel is needed to understand the injury patterns and treatment strategies to give recommendations on the prevention and treatment of this injury. The aim of this study is to report a case of a young patient who had CPN palsy after military training in the United Arab Emirates and the due clinical course of recovery.
A previously healthy 18-year-old man presented with a 2-month history of spontaneous right foot drop. The symptoms of tingling numbness started after the patient sat in cross-legged position for 2 h as a part of military training. When the patient got up from the cross-legged position, he was not able to dorsiflex his foot and had numbness in the foot. Physical examination showed numbness of the lateral leg and dorsum of the foot and 0 out of 5 grade of the Medical Research Grading Scale in ankle and great toe dorsiflexion and ankle eversion. The knee and leg radiographs and magnetic resonance imaging did not show any space-occupying lesions. The patient was treated with an ankle foot orthosis, physiotherapy, and oral 5-day course methylprednisolone therapy. The symptoms of foot drop and sensory loss did not improve with non-operative treatment over 3 months. Nerve conduction studies showed increased latency and decreased amplitude of the right peroneal nerve at the knee, whereas electromyography showed denervation of the tibialis anterior and extensor digitorum brevis. A clinical diagnosis was made of CPN palsy due to CECS not responsive to non-operative treatment. The patient underwent a surgery for CPN and superficial peroneal nerve (SPN) neurolysis and anterior and lateral leg compartment releasewith two separate incisions. Proximally, a 5 cm incision centered on the head of the fibula was used to release the fascia over CPN (A). The nerve was traced proximally and showed no compression. Distally, the anterior compartment of the leg was decompressed by incising the anterior septum between the tibialis anterior and extensor hallucis longus (Fig 1B). The lateral compartment was released by incising the posterolateral septum between the extensor hallucis longus and peroneal muscles and also the septum posterior to the peroneal muscles. A second incision measuring 12 cm centered 11 cm proximal to the tip of the distal fibula and 2 cm lateral to the anterior border of the tibia was used to decompress the SPN. The nerve was identified as it emerged from the deep lateral compartment and the fascia around it was released. The subcutaneous lateral compartment fasciotomy was performed all the way to the proximal tibia followed by a distal release down to the peroneal tunnel. After 12 days postoperatively, the patient had improvement in active ankle dorsiflexion up to neutral but no sensory improvement. At 3 months postoperatively, the patient had improvement in dorsiflexion and eversion of grade 3 out of 5 and 50% sensory improvement in the lateral part of the leg and dorsum of the foot. At 6 months postoperatively, the patient had full recovery of muscle power in ankle dorsiflexion and eversion and sensation in the lateral part of the leg and dorsum of the foot. At the last follow-up of 1 year after surgery, the patient returned to daily and recreational activities of playing football and paddle tennis without limitations.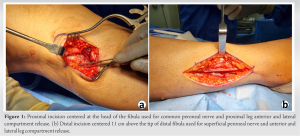
The CPN palsy after military training is uncommon. The case report presented here was a rare case of CPN palsy due to CECS presenting acutely after prolonged sitting cross-legged in a military exercise required surgical decompression of CPN and SPN nerves and leg compartment release. This report highlights the importance of surgical treatment of patients of CPN palsy with CECS by performing neurolysis of both CPN and SPN along with anterior and lateral compartment release. The report also emphasizes on timely surgical intervention at 3 months after failed non-operative treatment to improve chances of recovery. There have been few reports of CPN palsy in the setting of exertional compartment syndrome [5,6,7]. Solmaz et al. reported a case series of 28 patients with foot drop in military professionals attributed to either strenuous military routine or prolonged crouching or idiopathic [5]. The patients were treated operatively at a mean of 5 months since the injury with CPN decompression of the nerve with one incision at the fibular head. The motor recovery was incomplete in 3 (17%) patients and 1 (3%) patient had no improvement after surgery. Another report by Jimenez et al. of a lacrosse player with spontaneous CPN palsy due to acute exertional compartment syndrome treated with anterolateral fasciotomy alone failed to resolve the symptoms and the patient required a second procedure for CPM neurolysis [8]. Van Zantvoort et al. in a case series of 5 patients with CECS with CPN entrapment when patients slept on the affected side and successfully treated with CPN neurolysis [9]. This variability in treatment options and success of results in patients with CPN palsy and CECS raises an argument whether CPN neurolysis or fasciotomy as separate procedures are enough treatment for this patient population. We believe that the surgical treatment for CPN palsy due to CECS should include decompression of both CPN and SPN with two separate incisions along with anterior and lateral compartment release. This case report also highlights the importance of timely surgical intervention at 3 months in case of CPN palsy due to CECS where there is no evidence of recovery on clinical or nerve conduction studies. The previous reports on the influence of delay between the onset of symptoms of CPN palsy and surgical treatment are controversial [5]. Vastamäki. in a series of 24 patients with CPN palsy recommended operative treatment in case of no clinical recovery at 2 months after injury [10]. This study has limitations of being a case report and no objective evidence of CECS with compartment pressure measurement. In our practice, the diagnosis of CECS is based on clinical findings.
This case report of a young military recruit with CPN palsy after prolonged cross-legged sitting in the setting of CECS demonstrates successful treatment with a combined CPN and SPN neurolysis and anterior and lateral compartment release. Future studies should explore the efficacy of this treatment option and prevention strategies of CPN palsy in military personnel.
This case report illustrates the severity of CPN that can be resulted due to CECS with high levels of activity like military personnel. This report also demonstrates that in patients with CPN palsy in the setting of CECS, a combined surgical treatment with nerve decompression and compartment release provides a successful outcome instead of CPN decompression alone.
References
- 1.Lezak B, Massel DH, Varacallo M. Peroneal nerve injury. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK549859 [Last assessed on 2022 Oct 02]. [Google Scholar | PubMed]
- 2.Keny SM, Dabral L, Meshram P, Ansari N, Gokhale N, Nawale S, et al. Acute onset common peroneal nerve palsy in a child due to fibular head osteochondroma: A case report. Int J Res Orthop 2022;8:268-74. [Google Scholar | PubMed]
- 3.Toğrol E. Bilateral peroneal nerve palsy induced by prolonged squatting. Mil Med. 2000 Mar;165(3):240-2. [Google Scholar | PubMed]
- 4.Kodaira M, Sekijima Y, Ohashi N, Takahashi Y, Ueno K, Miyazaki D, et al. Squatting-induced bilateral peroneal nerve palsy in a sewer pipe worker. Occup Med (Lond) 2017;67:75-7. [Google Scholar | PubMed]
- 5.Solmaz I, Cetinalp EN, Göçmez C, Albayrak BS, Kural C, Kaya HS, et al. Management outcome of peroneal nerve injury at knee level: Experience of a single military institution. Neurol Neurochir Pol 2011;45:461-6. [Google Scholar | PubMed]
- 6.Streckmann F, Balke M, Cavaletti G, Toscanelli A, Bloch W, Décard BF, et al. Exercise and neuropathy: Systematic review with meta-analysis. Sports Med 2022;52:1043-65. [Google Scholar | PubMed]
- 7.Kollrack YM, Möllenhoff G. Exertional compartment syndrome of the lower leg and common peroneal nerve palsy as combined injury after weight lifting. Sportverletz Sportschaden 2009;23:165-8. [Google Scholar | PubMed]
- 8.Jimenez A, Branam BR, Hasselfeld KA, Hasselfeld KA. A case report of acute exertional compartment syndrome with peroneal nerve palsy in an adolescent athlete. J Orthop Case Rep 2019;10:1-3. [Google Scholar | PubMed]
- 9.Van Zantvoort AP, Setz MJ, Hoogeveen AR, Scheltinga MR. Common peroneal nerve entrapment in the differential diagnosis of chronic exertional compartment syndrome of the lateral lower leg: A report of 5 cases. Orthop J Sports Med 2018;6:2325967118787761. [Google Scholar | PubMed]
- 10.Vastamäki M. Decompression for peroneal nerve entrapment. Acta Orthop Scand 1986;57:551-4. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2025 A Case of Volkmann’s Ischemic Contracture – A Case Report
September 1, 2025 A Case of Volkmann’s Ischemic Contracture – A Case Report January 1, 2025 Femoral Nerve injury from slip and fall: A novel presentation of debilitating injury
January 1, 2025 Femoral Nerve injury from slip and fall: A novel presentation of debilitating injury October 1, 2024 Beyond Tradition: “Figure of 8” Casting for Gartland Type 1 and Type 2A Pediatric Supracondylar Fractures of Humerus: Video Technique
October 1, 2024 Beyond Tradition: “Figure of 8” Casting for Gartland Type 1 and Type 2A Pediatric Supracondylar Fractures of Humerus: Video Technique September 1, 2024 Compartment Syndrome Following Intramedullary Nailing of the Tibia: A Case Report
September 1, 2024 Compartment Syndrome Following Intramedullary Nailing of the Tibia: A Case Report