
In PCL avulsion, the size, geometry of the fragment, and associated rim injury dictate the method of fixation and we presented a case wherein PCL avulsion with rim fracture was fixed using sutures and knotless anchors.
Dr. M L V Sai Krishna, Department of Orthopaedics, All India Institute of Medical Sciences, New Delhi, India. E-mail: krishna.mlv.sai@gmail.com
Introduction: Posterior cruciate ligament (PCL) avulsion fractures are the most common type of isolated PCL injuries. Avulsion from the tibia is more common than femoral attachment. They can present as isolated tibial avulsion or as a component of posterior tibial rim fractures. The size, geometry of the fragment, and associated ligamentous injury dictate the method of fixation.
Case Report: A 32-year-old patient presented with posterior rim tibial plateau fracture with PCL avulsion after a motor vehicle accident. We used Burke and Schaffer approach and fixed the ligamentous avulsion and rim fracture using high tensile sutures and knotless swivel lock anchors.
Conclusion: PCL avulsions can present either as an isolated injury or as a part of a complex injury involving the anterior or posterior tibial rim. These complex injuries occur due to the hyperextension mechanism which results in either anterior tibial plateau compression fracture or posterior rim avulsion injuries. The treatment of such injuries requires addressing both ligamentous and bony components. The size, geometry of the fragment, and associated ligamentous injury dictate the method of fixation. We described the fixation of both ligamentous and rim avulsion using sutures and knotless anchors.
Keywords: Posterior cruciate ligament avulsion, tibial rim fractures, sutures, anchors.
Posterior cruciate ligament (PCL) avulsion fractures are the most common type of isolated PCL injuries. Avulsion from the tibia is more common than femoral attachment. They can present as isolated tibial avulsion or as a component of posterior tibial rim fractures. The isolated PCL avulsion injuries are more commonly seen in motorcycle accidents and dashboard injuries whereas the injuries of the posterior rim occur due to the hyperextension mechanism [1,2,3,4]. Operative treatment for PCL avulsions by reduction and fixation either by open or arthroscopy yields better results than conservative treatment. Posterior rim fractures with or without associated ligamentous injury are treated as intraarticular fractures. The size, geometry of the fragment, and associated ligamentous injury dictate the method of fixation [5,6,7,8,9,10,11]. In this case report, we have described a patient with posterior tibial rim fracture with PCL avulsion and its fixation through an open procedure using high tensile sutures and knotless anchors.
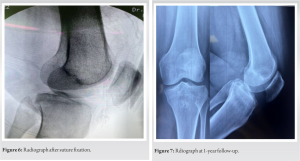
A 32-year-old female had a fall from a two-wheeler and sustained an injury to the left knee. She presented to us with knee pain and an inability to bear weight. She had diffuse pain over the knee with a contusion on the anterior knee. She had posterior tibial sag and the posterior drawer test was positive. The varus and valgus stress tests were comparable with the opposite knee. The range of movement was from 0° to 90° with further movement painful. The dial test was negative at 30° and 90°. The radiograph and the computed tomography scan were suggestive of posterior tibial rim fracture along with PCL avulsion fracture from the tibial insertion (Fig. 1). The patient was planned for open reduction and fixation. The patient was operated on under regional anesthesia in a prone position with a tourniquet over the proximal thigh. A lazy S-shaped skin incision was placed over the popliteal fossa with a horizontal limb over the fossa and vertical limbs over the lateral distal femur and proximal medial tibia (Fig. 2). The dissection was between the medial gastrocnemius and semimembranosus (Fig. 3) as suggested by Burke and Schaffer. Deep into this plane, the popliteus muscle was seen and elevated from the proximal tibia. The posterior capsule of the knee joint was identified along with the avulsed tibial fragment. The fragment was initially stabilized with a K wire (Fig. 4). Then, four high tensile sutures (Fiber wire No. 2, Arthrex, Naples, Florida) were passed through the posterior capsule and PCL at their tibial insertion on the avulsed fragment (Fig. 5).
The patient was planned for open reduction and fixation. The patient was operated on under regional anesthesia in a prone position with a tourniquet over the proximal thigh. A lazy S-shaped skin incision was placed over the popliteal fossa with a horizontal limb over the fossa and vertical limbs over the lateral distal femur and proximal medial tibia (Fig. 2). The dissection was between the medial gastrocnemius and semimembranosus (Fig. 3) as suggested by Burke and Schaffer. Deep into this plane, the popliteus muscle was seen and elevated from the proximal tibia. The posterior capsule of the knee joint was identified along with the avulsed tibial fragment. The fragment was initially stabilized with a K wire (Fig. 4). Then, four high tensile sutures (Fiber wire No. 2, Arthrex, Naples, Florida) were passed through the posterior capsule and PCL at their tibial insertion on the avulsed fragment (Fig. 5). A knotless fixation was planned with two swivel lock PEEK anchors (4.9 mm, Arthrex, Naples, Florida). Two drill holes were made and the drill holes were tapped for the passage of anchors. The sutures that were passed through the capsule and PCL were then passed through the anchors, with two sets of sutures through each anchor. The anchor along with the sutures was threaded through the posterior tibial cortex with sutures in tension and the K wire was removed (Fig. 5). The reduction was checked under the image (Fig. 6) and the tourniquet deflated. The wound was washed and closed in layers. A posterior knee plaster was applied with a proximal tibial posterior padding to prevent posterior sagging. The patient was started on isometric quadriceps exercises from day 1 and non-weight-bearing crutch walking was also started. At 2 weeks, the plaster was removed and sutures were also removed.
A knotless fixation was planned with two swivel lock PEEK anchors (4.9 mm, Arthrex, Naples, Florida). Two drill holes were made and the drill holes were tapped for the passage of anchors. The sutures that were passed through the capsule and PCL were then passed through the anchors, with two sets of sutures through each anchor. The anchor along with the sutures was threaded through the posterior tibial cortex with sutures in tension and the K wire was removed (Fig. 5). The reduction was checked under the image (Fig. 6) and the tourniquet deflated. The wound was washed and closed in layers. A posterior knee plaster was applied with a proximal tibial posterior padding to prevent posterior sagging. The patient was started on isometric quadriceps exercises from day 1 and non-weight-bearing crutch walking was also started. At 2 weeks, the plaster was removed and sutures were also removed. 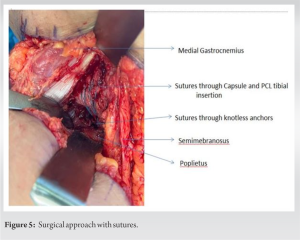
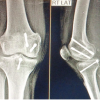
 A brace was applied with proximal leg PCL support and non-weight bearing was allowed along with isometric quadriceps and ankle range of movement exercises. At 4 weeks, partial weight bearing was allowed progressing to full weight bearing by 8 weeks. The patient was started on an open chain range of movement exercises of the knee and active straight leg rising. Night-time bracing was continued for 2 months. At 6-month and 1-year follow-up, the patient had no complaints and she achieved her full range of movement (Fig. 7). There was no posterior tibial sag.
A brace was applied with proximal leg PCL support and non-weight bearing was allowed along with isometric quadriceps and ankle range of movement exercises. At 4 weeks, partial weight bearing was allowed progressing to full weight bearing by 8 weeks. The patient was started on an open chain range of movement exercises of the knee and active straight leg rising. Night-time bracing was continued for 2 months. At 6-month and 1-year follow-up, the patient had no complaints and she achieved her full range of movement (Fig. 7). There was no posterior tibial sag.
Approximately 10% of all tibial plateau fractures cannot be classified based on Schatzker’s classification. These include fractures associated with dislocations and having a concomitant ligamentous injury. One such fracture subtype is rim fractures of the posterior tibial plateau with or without ligamentous injury. The mechanism of injury for such fractures involves a hyperextension mechanism, with varus or valgus components and a rotational force. These injuries result in either an anteromedial or anterolateral fracture and an associated posterior tension band injury. This has been described as a diagonal lesion [1,2,3,4]. The posterior tension band injury can include either a ligamentous injury or a bony injury. The ligamentous injury can involve PCL or the posterolateral corner. The bony injury includes the failure of the posterior tibial rim either medial or lateral. They can also present without any associated anterior tibial plateau fracture of the diagonal lesion. The posterior tension band injury can be treated by either addressing the ligamentous injury or fixing the bony avulsions [2,3,4]. Isolated PCL avulsion fixation can be done either by arthroscopy or open method. Based on the size of the avulsed fragment, Kim et al. [5] proposed the fixation of comminuted fragments or fragments <10 mm with sutures, fragments >10 mm with K wires, and fragments >20 mm with screws. Various plates [6] and suture anchors [7,8] have also been used for the fixation of avulsed fragments depending on the size and comminution. Song et al. [9] published the results of a systematic review comparing clinical outcomes of arthroscopic suture fixation versus the open posterior approach for PCL avulsion fractures. They showed comparable clinical outcomes, radiological healing, and stability of the knee in both techniques. Very few reports have been described for rim fractures with PCL avulsions [1,9,10,11]. These fractures have been fixed by an open approach with plates and screws. Burk and Schaffer’s [2] approach has been used for posteromedial rim component and for fixation of the posterolateral fracture Brosch’s [1] approach and its modifications including the trans-fibular approach [9] have been described. Posterolateral approaches have been described and the fixation involves plates and screws with various modifications [10,11]. Our technique involves open fixation of posterior rim fracture with PCL avulsion using Burke and Schaffer’s posteromedial approach. High tensile sutures were passed through the posterior capsular tissue and PCL tibial insertion which are then fixed to the bone using knotless anchors. We have used a swivel lock anchor as an implant of choice for fixation. The advantages of our technique include all the advantages of an open procedure like adequate visualization of the avulsed fragment. Since we have used sutures, this technique can be used even when the avulsed fragment is small and comminuted, where plates and screws risk further comminution. The benefit of a swivel lock anchor is that it comes with a drill, tap, and thread technique. Simple drilling and push-in technique risks anchor breakage or deformation due to strong posterior tibial cortical bone that can be avoided with a thread in anchor.
PCL avulsions can present either as an isolated injury or as a part of a complex injury involving the anterior or posterior tibial rim. These complex injuries occur due to the hyperextension mechanism which results in either anterior tibial plateau compression fracture or posterior rim avulsion injuries. The treatment of such injuries requires addressing both ligamentous and bony components. The size, geometry of the fragment, and associated ligamentous injury dictate the method of fixation. We described the fixation of both ligamentous and rim avulsion using sutures and knotless anchors.
The size of the fragment dictates the fixation of the PCL avulsion with or without involving the tibial rim. In our technique, we used sutures and knotless anchors as a method of fixation in a patient with PCL avulsion along with tibial rim fracture.
References
- 1.Chang SM, Zheng HP, Li HF, Jia YW, Huang YG, Wang X, et al. Treatment of isolated posterior coronal fracture of the lateral tibial plateau through posterolateral approach for direct exposure and buttress plate fixation. Arch Orthop Trauma Surg 2009;129:955-62. [Google Scholar | PubMed]
- 2.Li X, Song G, Li Y, Liu X, Zhang H, Feng H. The “diagonal” lesion: A new type of combined injury pattern involving the impingement fracture of anteromedial tibial plateau and the injury of posterior cruciate ligament and posterolateral corner. J Knee Surg 2020;33:616-22. [Google Scholar | PubMed]
- 3.Zhang X, Tian X, Wang S, Hu Y, Pan S, Peng A. Different patterns of tibial plateau fractures associated with hyperextension injuries of the knee with or without varus/valgus component. Medicine (Baltimore) 2021;100:e28337. [Google Scholar | PubMed]
- 4.Firoozabadi R, Schneidkraut J, Beingessner D, Dunbar R, Barei D. Hyperextension varus bicondylar tibial plateau fracture pattern: diagnosis and treatment strategies. J Orthop Trauma 2016;30:e152-7. [Google Scholar | PubMed]
- 5.Kim SJ, Shin SJ, Choi NH, Cho SK. Arthroscopically assisted treatment of avulsion fractures of the posterior cruciate ligament from the tibia. J Bone Joint Surg Am 2001;83:698-708. [Google Scholar | PubMed]
- 6.Khatri K, Sharma V, Lakhotia D, Bhalla R, Farooque K. Posterior crucial tibial avulsion treated with open reduction and internal fixation through Burks and Schaffer approach. Malays Ortop J 2015;9:2-8. [Google Scholar | PubMed]
- 7.Hooper PO 3rd, Silko C, Malcolm TL, Farrow LD. Management of posterior cruciate ligament tibial avulsion injuries: A systematic review. Am J Sports Med 2018;46:734-42. [Google Scholar | PubMed]
- 8.Sun K, Fan M. Study of double button plate and cannulated screw fixation for posterior cruciate ligament avulsion fracture. Ann Clin Case Rep 2022;7:2306. [Google Scholar | PubMed]
- 9.Song JG, Nha KW, Lee SW. Open posterior approach versus arthroscopic suture fixation for displaced posterior cruciate ligament avulsion fractures: Systematic review. Knee Surg Relat Res 2018;30:275-83. [Google Scholar | PubMed]
- 10.Kim Y, Yoon YC, Cho JW, Cho WT, Jeon NH, Oh CW, et al. Rim plate augmentation of the posterolateral bare area of the tibial plateau using a 3.5-mm precontoured locking compression plate: A cadaveric study. J Orthop Trauma 2018;32:e157-60. [Google Scholar | PubMed]
- 11.Solomon LB, Stevenson AW, Baird RP, Pohl AP. Posterolateral transfibular approach to tibial plateau fractures: Technique, results, and rationale. J Orthop Trauma 2010;24:505-14. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 Posterior Approach for Single-stage Fixation of Medial Hoffa with Posterior Cruciate Ligament Avulsion: A Rare Case Report
November 1, 2025 Posterior Approach for Single-stage Fixation of Medial Hoffa with Posterior Cruciate Ligament Avulsion: A Rare Case Report January 1, 2025 A Rare Case Report: Managing PCL Avulsion Fracture with a Fracture of the Proximal Tibial Shaft
January 1, 2025 A Rare Case Report: Managing PCL Avulsion Fracture with a Fracture of the Proximal Tibial Shaft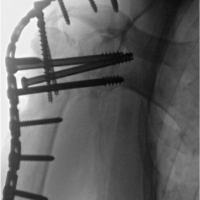 July 10, 2022 Glenohumeral Arthrodesis for Treatment of Unique Instability with Axillary Nerve Injury: A Case Report
July 10, 2022 Glenohumeral Arthrodesis for Treatment of Unique Instability with Axillary Nerve Injury: A Case Report July 10, 2020 Total Elbow Arthroplasty as Treatment of Non-union with Bone Loss of Distal Humerus – A Case Report
July 10, 2020 Total Elbow Arthroplasty as Treatment of Non-union with Bone Loss of Distal Humerus – A Case Report