
Damage Control Orthopedics (DCO) is indispensable when managing unstable trauma patients, wherein early definitive fixation (EDF) can lead to significantly better outcomes in hemodynamically stable patients. The success of EDF is contingent on robust ICU support anchored in a collaborative, multidisciplinary approach to patient care. As India continues to grapple with the ever-increasing incidence of RTAs, an adherence to ATLS protocols coupled with appropriate use of EDF in applicable patients will prove critical in improving trauma outcomes.
Dr. Rohan Jayaram, Department of Orthopaedics, Dr. D.Y. Patil School of Medicine and Hospital, Navi Mumbai, Maharashtra, India. E-mail: drrohanjayaram@gmail.com
Introduction: Road traffic accidents (RTA) account for a sizable portion of morbidity and mortality globally, with a particularly high incidence among young and active individuals. Patients presenting with polytrauma require a multidisciplinary approach guided by protocols for advanced trauma life support.
Case Report: We report the case of a 31-year-old female, transferred-in to our center following primary care after an RTA on June 17th, 2023. Initial assessment at the other hospital found multiple fractures accompanying her internal injuries – a right haemothorax and pulmonary contusion, with Grade 3 injuries to the liver, spleen, and kidneys. The patient, who was also found to be pregnant, presented to our facility with hypotension and breathlessness. Stabilization efforts spanned to include ventilatory support following resuscitation in the intensive care unit. Upon achieving hemodynamic stabilization, early definitive fixation was meticulously planned and implemented, leading to intramedullary nailing of the femur, open reduction and internal fixation in the left wrist, and percutaneous fixation of the right acetabulum. Despite landing in post-operative complications such as pleural effusion and subcutaneous emphysema, the patient showed remarkable recovery and was successfully extubated on June 27th, 2023. She was discharged vitally stable, and continued recovery at her residence. The patient managed to regain full range of motion in all joints, with good union of fractures at the end of her 1-year post-operative follow-up period.
Conclusion: This case highlights the importance of tailoring an approach which was unique to the polytrauma presentation. While damage control orthopaedics is often recommended in unstable patients, early definitive orthopedic care must be considered where patients are successfully resuscitated and stabilized, invariably improving trauma outcomes.
Keywords: Road traffic accident, polytrauma, advanced trauma life support, early definitive orthopedic care, bilateral femoral fractures, pneumothorax.
India has seen a significant increase concerning road traffic accidents (RTAs) over past years, with an estimated 4.5 lakh accidents being reported annually – leading to approximately 1.5 lakh fatalities. This alarming rising trend is attributed to the increasing number of vehicles on the road, inadequate traffic management, and poor driving habits. Such accidents are often observed resulting in polytrauma injuries, thus requiring urgent and efficient medical intervention [1]. The implementation of advanced trauma life support (ATLS) protocols has vastly improved management modalities among trauma patients. The ATLS approach guarantees identification of critical life-threatening conditions whilst providing the proper sequential management, in efforts to ensure that patient receives prompt treatment with improved chances of survival[2]. The focus is on damage control orthopaedics (DCO) for those presenting in hemodynamically unstable conditions. This approach prioritizes life and advocates temporary stabilization of fractures to prevent further physiological deterioration made possible by avoiding a second insult. DCO may involve external or temporary internal fracture fixation, allowing the patient to stabilize before taking up for the definitive surgical intervention [3]. However, early definitive fixation (EDF) of fractures is mostly seen to be preferred in hemodynamically stable patients. EDF has shown to prove reduced complications with shorter hospital stays, whilst also improving functional outcome. It involves immediate surgical fixation of fractures, followed by early mobilization in order to avoid risks associated with prolonged immobilization, via-à-vis deep vein thrombosis, and pneumonia, amongst other fatal cardiopulmonary events. Studies have demonstrated to show that EDF, when performed in a stable patient, leads to better outcomes than delayed fixation [4]. A well-equipped intensive care unit (ICU) and multi-disciplinary team are essential in managing the patient’s perioperative needs, including vigilant monitoring of vitals, fluid balance, and organ function [5, 6]. We present a case in which we performed EDF for early mobilization in a polytrauma patient at a tertiary healthcare hospital in Navi Mumbai.
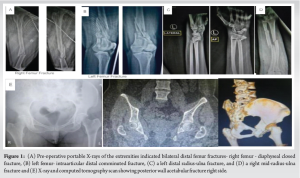
A 31-year-old female, transferred-in from another center following a high velocity trauma due to a RTA (2-wheeler vs. 4-wheeler) on June 17th, 2023, around 06:15 PM near Uran Panvel Highway. She presented with multiple fractures and internal injuries. Following the accident, patient was provided primary care at a different tertiary care center, where primary examination and first aid was performed and multiple injuries were identified. Chest X-ray and high-resolution computed tomography (CT) of thorax revealed a right haemothorax and pulmonary contusion, necessitating the insertion of an intercostal drainage (ICD) tube. Further imaging showed a Grade 3 liver injury, Grade 3 splenic injury, Grade 3 renal injury, undisplaced fracture of posterior wall of left acetabulam (Fig. 1e), and haemoperitoneum. Radiographs of extremities revealed bilateral distal femur fractures – closed diaphyseal right femur (Fig. 1a) with comminuted intra-articular left femur (Fig. 1b), left distal radius-ulna fracture (Fig. 1c), and right mid-shaft radius-ulna fracture (Fig. 1d). She also tested positive pregnancy evidenced by urine pregnancy test and a beta human chorionic gonadotropin level of 101.4.
Course at our hospital
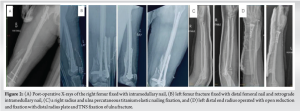
Upon arrival at our center, the patient was found hypotensive (90/60 mmg) and tachypnoeic (Respiratory rate – 31/min). She was stabilized in the emergency room and transferred to the Intensive Care Unit (ICU), where additional ventilatory support with bilevel-positive airway pressure (BiPAP) was provided in accordance to sustained hypotension and increasing oxygen requirements. Comprehensive evaluations, ranging across echocardiography to CT scans, revealed mild global left ventricular hypokinesia and multiple rib fractures, amongst add vcdsitional findings. As the patient was able to achieve hemodynamic stability after 2 days in the ICU following resuscitation, orthopaedic interventions were provided based on principles of EDF. This included intramedullary nailing of the right femur, and distal femoral nailing alongside plating by lateral condylar locking plate over the left femur. Open reduction with internal fixation of the left wrist was performed through distal radius plating and titanium elastic nail (TENS) fixation of the ulna, and percutaneous TENS fixation contralaterally of the left radius and ulna(Fig. 2). Fixation of the right acetabulum was undertaken by a percutaneous antegrade posterior column screw, on June 20th and 23rd of 2023. Subsequently, complications of pleural effusion and subcutaneous emphysema set in, which were managed by re-insertion of ICD tube along with appropriate medical care.
Outcome
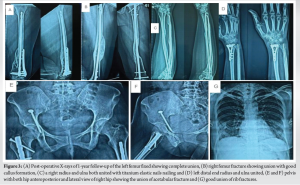
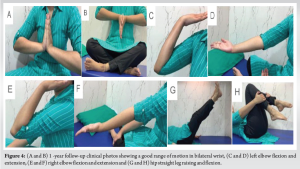
The patient’s condition gradually improved with continuous supportive care, including blood transfusions, antibiotics, and physiotherapy. She was successfully extubated on June 27, 2023, and transitioned to oral medications. After stabilizing hemodynamically, she was discharged with the central line and silicon catheter in situ, showing significant recovery from her injuries. Immediate post-operative X-rays show a satisfactory reduction. On 1-year follow-up patient is mobilizing independently with the ability to perform all activities of daily living. The fractures show good union at all fracture sites (Fig. 3). The patient has a full range of motion in bilateral hips, knees, elbows, and wrists (Fig. 4).
Polytrauma patients, especially those with serious injuries and physiological derangements, have typically been managed using DCO. The primary purpose of DCO is to stabilize the patient using temporary fixation procedures, reducing the surgical load until the patient is hemodynamically stable and can withstand definitive surgery. However, new research has emphasized the potential benefits of EDF in selected polytrauma patients, demonstrating that it can improve outcomes under specific settings.
Benefits of EDF for hemodynamically stable patients
Several studies have shown that in hemodynamically stable polytrauma patients, EDF can lead to better results than DCO. Pape et al. (2007) discovered that patients who received EDF had a shorter ICU stay and total hospital stay. This was related to early mobilization and decreased consequences such as infection and multi-organ failure [7]. Similarly, several studies have found that EDF reduces the need for subsequent operations, which is helpful in terms of lowering the risks associated with recurrent anesthesia and surgical procedures. For example, Vallier et al. (2013) found that patients who got EDF had less issues with pulmonary function and infection than those who underwent stepwise treatments characteristic of DCO [8].
Criteria for choosing EDF over DCO
The choice between EDF and DCO should be based on the patient’s initial physiological condition and damage severity. Giannoudis et al. (2016) found that patients with mild injury severity ratings (injury severity score ISS <25) and stable physiological indicators are most suited for EDF. The study discovered that EDF lowered the overall treatment duration in this subgroup and resulted in speedier recovery [9]. Scalea et al. (2000) found that patients with severe injuries and symptoms of physiological compromise, such as acidosis, hyper-coagulopathy, and hypothermia, benefit the most from DCO. This emphasizes the significance of a personalized approach in which the choice between EDF and DCO is driven by real-time clinical evaluation [10].
Impact on long-term results
Long-term results, such as regain of function and return to work, have been favorable in patients with EDF. Oochit et al. (2024) found that EDF improves long-term function, especially for lower extremity fractures. The authors speculated that this advantage is related to avoiding the additional insult related to temporary fixation systems and the early start of recovery [11]. In contrast, DCO frequently demands a second final operation, which might postpone rehabilitation and lengthen overall recovery time. This delay may lead to problems such as joint stiffness and muscular atrophy, which are less prevalent in EDF patients [12].
Comparison of outcomes
When comparing the results of EDF with DCO, it is evident that while DCO saves lives in unstable patients, EDF provides considerable advantages in stable patients. According to Pfeifer et al.’s (2017) meta-analysis, EDF patients had a lower risk of complications, such as acute respiratory distress syndrome and systemic inflammatory response syndrome, than those treated with DCO [13]. Furthermore, EDF is related to improved pain management because permanent fixation stabilizes fractures more efficiently than interim treatments [8]. This was underlined in the study of Castillo et al. (2017), who said that pain management is an essential component of early recovery and that EDF leads to improved pain outcomes and patient satisfaction [14].
This case underscores the importance of a multidisciplinary approach to timely assessment and intervention in managing polytrauma patients. While DCO is typically favoured in unstable patients, our report demonstrates that early definitive orthopedic care can be safely undertaken in stable patients, leading to better functional outcomes. The contribution of each discipline and adherence to ATLS protocols were pivotal in successfully managing the patient, making each team member integral to the patient’s care.
Early definitive orthopedic care can be considered in polytrauma patients who are hemodynamically stable following resuscitation. This approach may improve outcomes significantly, reducing the need for multiple surgeries and prolonged hospital stays. It is imperative the medical fraternity consider this approach more frequently, as it can inspire positive change in trauma care outcomes.
References
- 1.Available from: https://morth.nic.in/sites/default/files/ra_2021_compressed.pdf [Last accessed on 2024 Aug 17]. [Google Scholar | PubMed]
- 2.Kaczynski J. Resuscitation beyond advanced trauma life support: Damage control. Br J Hosp Med (Lond) 2013;74:144-8. [Google Scholar | PubMed]
- 3.Pfeifer R, Kalbas Y, Coimbra R, Leenen L, Komadina R, Hildebrand F, et al. Indications and interventions of damage control orthopedic surgeries: An expert opinion survey. Eur J Trauma Emerg Surg 2021;47:2081-92. [Google Scholar | PubMed]
- 4.Vallier HA, Moore TA, Como JJ, Wilczewski PA, Steinmetz MP, Wagner KG, et al. Complications are reduced with a protocol to standardize timing of fixation based on response to resuscitation. J Orthop Surg Res 2015;10:155. [Google Scholar | PubMed]
- 5.Dogjani A, Bendo H, Blloshmi A. Polytrauma - Definition and management aspects and trauma score? Albanian J Trauma Emerg Surg 2017;1:9-10. [Google Scholar | PubMed]
- 6.National Academies of Sciences, Engineering, and Medicine, Health and Medicine Division, Board on the Health of Select Populations, Board on Health Sciences Policy, Committee on Military Trauma Care’s Learning Health System and Its Translation to the Civilian Sector. A National Trauma Care System: Integrating Military and Civilian Trauma Systems to Achieve Zero Preventable Deaths After Injury. United States: National Academies Press; 2016. p. Available from: https://books.google.com/books/about/a_national_trauma_care_system.html?hl=&id=oz0udqaaqbaj [Google Scholar | PubMed]
- 7.Pape HC, Giannoudis P, Krettek C. The timing of fracture treatment in polytrauma patients: Relevance of damage control orthopedic surgery. Am J Surg 2002;183:622-9. [Google Scholar | PubMed]
- 8.Vallier HA, Cureton BA, Ekstein C, Oldenburg FP, Wilber JH. Early definitive stabilization of unstable pelvis and acetabulum fractures reduces morbidity. J Trauma 2010;69:677-84. [Google Scholar | PubMed]
- 9.Giannoudis PV, Tzioupis CC, Pape HC. Pelvic fractures in polytrauma patients. In: Damage Control Management in the Polytrauma Patient. New York: Springer New York; 2010. p. 299-314. Available from: https://link.springer.com/10.1007/978-0-387-89508-6_17 [Google Scholar | PubMed | CrossRef]
- 10.Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN. External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-21; discussion 621-3. [Google Scholar | PubMed]
- 11.Oochit K, Imran A, Marsh A. 9 early vs late definitive fixation of pelvic ring fractures in polytraumatized patients. A systematic review and meta-analysis. Br J Surg 2024;111:znae163.185. [Google Scholar | PubMed]
- 12.Volpin G, Pfeifer R, Saveski J, Hasani I, Cohen M, Pape HC. Damage control orthopaedics in polytraumatized patients- current concepts. J Clin Orthop Trauma 2021;12:7-82. [Google Scholar | PubMed]
- 13.Pfeifer R, Heussen N, Michalewicz E, Hilgers RD, Pape HC. Incidence of adult respiratory distress syndrome in trauma patients: A systematic review and meta-analysis over a period of three decades. J Trauma Acute Care Surg 2017;83:496-506. [Google Scholar | PubMed]
- 14.Castillo RC, Raja SN, Frey KP, Vallier HA, Tornetta P 3rd, Jaeblon T, et al. Improving pain management and long-term outcomes following high-energy orthopaedic trauma (pain study). J Orthop Trauma 2017;31:S71-7. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 In Trauma Expect the Unexpected – A Case Report on Post-Traumatic Pancreatitis associated with Superior Mesenteric Artery Pseudoaneurysm in Spinopelvic fracture
November 1, 2025 In Trauma Expect the Unexpected – A Case Report on Post-Traumatic Pancreatitis associated with Superior Mesenteric Artery Pseudoaneurysm in Spinopelvic fracture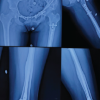 October 1, 2025 Girl with Multiple Fractures: A Unique Case of Polytrauma
October 1, 2025 Girl with Multiple Fractures: A Unique Case of Polytrauma October 1, 2025 A Unique Case of Bilateral Elbow Terrible Triad in a Polytrauma Patient: Associated Challenges in Management
October 1, 2025 A Unique Case of Bilateral Elbow Terrible Triad in a Polytrauma Patient: Associated Challenges in Management September 1, 2025 Triple-Segmental Shaft Femur Fracture: A Case Report
September 1, 2025 Triple-Segmental Shaft Femur Fracture: A Case Report