
The case emphasizes the need for orthopedic surgeons to adopt a tailored approach for epileptic patients with hip fractures, factoring in seizure history, bone quality, and the potential complications from standard fixation methods.
Dr. Mansoor Malnas, Postgraduate Student, Department of Orthopaedics, Bombay Hospital, Mumbai, Maharashtra, India. E-mail: malnasmansoor@gmail.com
Introduction: The occurrence of non-traumatic bilateral femoral neck fractures is exceedingly rare, and their manifestation subsequent to an epileptic attack is an uncommon entity with very few cases reported globally.
Case Report: We present the positive outcome of a 68-year-old man who underwent staged bilateral constrained total hip arthroplasty following a fracture resulting from a generalized seizure. This unconventional decision was justified based on several factors, including fracture pattern, bone quality, seizure history, and advanced tribology.
Conclusion: Epileptic patients pose a potential high risk for hip dislocation or fracture neck of femur. In such cases, we advocate for primary constrained arthroplasties as a viable and durable option, considering the specific circumstances and challenges associated with these patients.
Keywords: Constrained acetabular liners, bilateral femoral neck fractures, atraumatic fractures, epilepsy and fractures, rare.
It is exceedingly rare for a patient to sustain non-traumatic fractures of bilateral femoral neck. While hip fractures are commonplace injuries treated by orthopedic surgeons, they characteristically occur unilaterally in elderly individuals with osteoporosis resulting from trival trauma such as a fall or a high-energy trauma in young individual. Bilateral femoral neck fractures, on the other hand, represent an infrequent clinical presentation often linked to contributing factors such as metabolic diseases or chronic renal disease that compromise bone integrity, the physiologic stress following electroconvulsive therapy procedures, or violent muscle contractions during a seizure episode as documented across the medical literature [1,2]. Of particular singularity are cases where these highly uncommon bilateral fractures arise in the acute aftermath of an epileptic seizure – only a very limited number of such instances have been reported worldwide to date. Fig. 1.
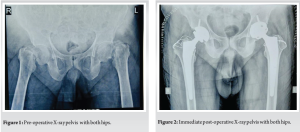
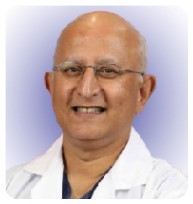
We present a case of a 68-year-old gentleman, a known epileptic for the past 15 years. Following a significant epileptic episode, he encountered abrupt and intense pain in both hip joints while in bed during the night. Subsequent to the episode, he found himself unable to mobilize or elevate his legs. A subsequent examination by his family physician the following morning prompted a portable X-ray, which suggested bilateral femoral neck fractures. The patient, under consistent anti-epileptic therapy (Tab Eptoin-Phenytoin and Tab Levera-Levetiracetam) for the past 15 years, had been seizure-free for the preceding 12 years. Approximately 3 months before the incident, a neuro-physician, assessing his condition, conducted an EEG with normal results, recommending a discontinuation of medication. On general examination, evidence of a tongue bite indicated a seizure during sleep. Although his MRI brain exhibited age-related atrophy without significant pathology, he was referred to our orthopedic department for further management. At the time of presentation, the patient was conscious, cooperative, and well orientation, with both limbs in adduction and external rotation. He experienced tenderness in the groin and significant pain on movement of both the hips, with no neurological or vascular deficits. Pelvic AP radiographs revealed Garden type IV transcervical neck of femur fractures with comminuted greater trochanter fractures in both hips. Despite having no previous hip pain and an active lifestyle, maintaining full functionality with weight-bearing. The severe displacement of hip fractures, delayed presentation, combined with his age and quality of bone, led us to anticipate a failure of osteosynthesis. Consequently, we planned bilateral total hip replacement surgery. Following thorough counseling with the patient and his family, staged bilateral hip replacement surgeries were proposed. Femur canal was Dorr B type, and pre-operative templating and planning led to the selection of uncemented prostheses (although cemented implants were kept backup) with a Ceramic on Poly bearing [3]. Comminuted fractures of the greater trochanter on both sides were addressed using two Tension band wires and non-absorbable supplementary Ethibond no. 5 sutures. The surgical procedure involved an anterolateral approach, utilizing a 32mm diameter head for the Pinnacle Poly constrained acetabular liner with a 50 mm outer shell diameter (DePuy, Warsaw, IN, USA) and a size 15 Corail cementless stem in the left hip. Subsequently, after a 5-day interval, the right hip underwent a similar procedure with similar implants. Both intraoperative and post-operative periods transpired without complications. Fig 2.
The patient was mobilized on day 3 after the second surgery around the bed with the aid of a walking device. By post-operative day 5, the patient was able to sit in a chair and was able to walk 100 m. Follow-up examinations at 3 months indicated the patient’s ability to walk independently with the support of a stick, and by 6 months, the patient demonstrated independent walking without any external assistance. At latest follow-up of 5 years, there is complete free mobility and is able to do all activities of daily routine independently with an excellent Harris Hip Score of 98.
In adults with normal bone structure, the occurrence of bilateral femoral neck fractures is an infrequent phenomenon, typically necessitating substantial external force such as a motor vehicle accident or a fall from a considerable height [1]. While violent muscle contractions during seizures are recognized to cause fractures or dislocations, with an incidence of 1.1% following a convulsion [2], the musculoskeletal consequences of seizures extend beyond the conventional posterior shoulder dislocation. However, there are notably scarce documented cases of bilateral hip fractures occurring during seizures [4,5]. Literature underscores that individuals with epilepsy face an elevated fracture risk, with an increased likelihood of two- to six-fold [6]. Notably, certain anti-epileptic drugs, particularly Phenytoin, are known to alter calcium metabolism, potentially inducing osteomalacia or reducing bone density during prolonged treatment. This elevates the susceptibility to pathological fractures, emphasizing the importance of monitoring bone mineral density in patients using anti-epileptic drugs [7]. Our patient, under long-term anti-epileptic therapy, had been receiving Vitamin D and calcium supplements, with initial values on admission indicating a Vitamin D level of 26.6 and a calcium level of 8.9. Histopathological examination of the femoral head specimen revealed normal bone histology. Recommendations by Pack et al advocate for Vitamin D and calcium supplementation, alongside vigilant monitoring of bone mineral density, especially in individuals undergoing prolonged antiepileptic treatment, particularly if they present with concurrent bone pathologies [8]. For patients under the age of 60, internal fixation of femoral neck fractures represents the standard of care, while arthroplasty procedures tend to be reserved for the elderly population or specific clinical scenarios [9,10]. In cases where inadequate reduction is achieved following femoral neck fractures, the risk of osteosynthesis failure becomes particularly concerning. However, the current evidence base has not established a definitive correlation between the timing of fixation and the subsequent development of osteonecrosis of the femoral head [11]. Duckworth et al. have identified a direct association between comorbidities compromising bone quality and fixation failure in displaced femoral neck fractures among the young adult demographic. Their findings suggest individuals over 40 years exhibiting compromised that bone integrity may warrant consideration for primary total hip arthroplasty given the heightened predisposition to fixation failure [12]. For this particular patient, the decision to undertake staged uncemented bilateral constrained total hip arthroplasties using anterolateral approach was predicated on several key considerations: The patient’s chronological age, the presence of an epileptic disorder, the prospective risk of developing post-operative aseptic osteonecrosis of the femoral heads, and the anticipated necessity for future revision procedures. It warrants highlighting that the rates of instability and dislocation following total hip arthroplasty undertaken for femoral neck fractures notably surpass those encountered in arthroplasty procedures performed for the treatment of degenerative osteoarthritis [15]. This risk is further compounded in patients with recurrent seizure disorders. Primary total hip arthroplasty in the setting of cognitive deficits or neuromuscular diseases has been associated with notable post-operative dislocation rates; hence, constrained liner or dual mobility hip arthroplasty is recommended in such cases [16,17]. In our surgical approach, we employed anterolateral exposures to circumvent violation of the posterior capsule and musculature, thereby mitigating dislocation risk [18-20]. Moreover, the utilization of constrained acetabular liners aimed to confer stability is a pivotal consideration in patients with a history of recurrent dislocations. Constrained acetabular components, renowned for their efficacy in preventing instability without substantially compromising implant longevity, were judiciously selected to optimize the durability of the arthroplasty constructs [21,22]. (Fig 3 & 4).

The case of the 68-year-old man highlights the unique challenges faced by orthopedic surgeons when treating epileptic patients with hip fractures. The need for a tailored approach is underscored, taking into account the patient’s seizure history, bone quality, and potential complications arising from standard fixation methods. The successful implementation of staged bilateral constrained total hip arthroplasty using anterolateral approach in this patient not only mitigated the risk of complications but also showcased a viable surgical option for such case. As the incidence of bilateral femoral neck fractures related to seizures remains exceedingly rare, this case serves as a crucial reminder for surgeons to prioritize individualized treatment strategies that address the complexities of each patient’s condition. By adopting such an approach, orthopedic surgeons can enhance outcomes for patients with epilepsy, ensuring both functional recovery and long-term stability in their hip joint health.
Non-traumatic bilateral femoral neck fractures, especially resulting from an epileptic seizure, are extremely rare. Only a few such cases have been reported globally. Epileptic patients are at a higher risk of fractures due to factors such as seizures and the long-term use of anti-epileptic drugs (like Phenytoin), which can impair calcium metabolism and bone quality. Opting for primary constrained arthroplasties stands as a viable and durable solution for addressing the unique challenges posed by hip pathology in these patients.
References
- 1.Sathyanarayana V, Patel MT, Raghavan S, Naresh D. Simultaneous bilateral femur neck fracture in a young adult with chronic renal failure- a case report and review of literature. J Orthop Case Rep 2015;5:24-6. [Google Scholar | PubMed]
- 2.Grimaldi M, Vouaillat H, Tonetti J, Merloz P. Simultaneous bilateral femoral neck fractures secondary to epileptic seizures: Treatment by bilateral total hip arthroplasty. Orthop Traumatol Surg Res 2009;95:555-7. [Google Scholar | PubMed]
- 3.Dorr LD, Wolf AW, Chandler R, Conaty JP. Classification and treatment of dislocations of total hip arthroplasty. Clin Orthop Relat Res 1983;173:151-8. [Google Scholar | PubMed]
- 4.Maimin DG, Meneses-Turino L. Seizures causing simultaneous bilateral neck of femur fractures. Case Rep Orthop 2019;2019:4570578. [Google Scholar | PubMed]
- 5.Cagırmaz T, Yapici C, Orak MM, Guler O. Bilateral femoral neck fractures after an epileptic attack: A case report. Int J Surg Case Rep 2015;6:107-10. [Google Scholar | PubMed]
- 6.Mattson RH, Gidal BE. Fractures, epilepsy, and antiepileptic drugs. Epilepsy Behav 2004;5:36-40. [Google Scholar | PubMed]
- 7.Bell RD, Pak CY, Zerwekh J, Barilla DE, Vasko M. Effect of phenytoin on bone and vitamin D metabolism. Ann Neurol 1979;5:374-8. [Google Scholar | PubMed]
- 8.Pack A. Bone health in people with epilepsy: Is it impaired and what are the risk factors? Seizure 2008;17:181-6. [Google Scholar | PubMed]
- 9.Araujo TP, Guimaraes TM, Andrade-Silva FB, Kojima KE, Silva JS. Influence of time to surgery on the incidence of complications in femoral neck fracture treated with cannulated screws. Injury 2014;45 Suppl 5:S36-9. [Google Scholar | PubMed]
- 10.Bhandari M, Devereaux PJ, Swiontkowski MF, Tornetta P 3rd, Obremskey W, Koval KJ, et al. Internal fixation compared with arthroplasty for displaced fractures of the femoral neck. A meta-analysis. J Bone Joint Surg Am 2003;85-A:1673-81. [Google Scholar | PubMed]
- 11.Duckworth AD, Bennet SJ, Aderinto J, Keating JF. Fixation of intracapsular fractures of the femoral neck in young patients: Risk factors for failure. J Bone Joint Surg Br 2011;93:811-6. [Google Scholar | PubMed]
- 12.Leighton RK, Schmidt AH, Collier P, Trask K. Advances in the treatment of intracapsular hip fractures in the elderly. Injury 2007;38:S24-34. [Google Scholar | PubMed]
- 13.Tidermark J, Ponzer S, Svensson O, Söderqvist A, Törnkvist H. Internal fixation compared with total hip replacement for displaced femoral neck fractures in the elderly. A randomised, controlled trial. J Bone Joint Surg Br 2003;85:380-8. [Google Scholar | PubMed]
- 14.Berry DJ, Von Knoch M, Schleck CD, Harmsen WS. The cumulative long-term risk of dislocation after primary charnley total hip arthroplasty. J Bone Joint Surg Am 2004;86:9-14. [Google Scholar | PubMed]
- 15.Marsh JP, Leiter JR, MacDonald P. Bilateral femoral neck fractures resulting from a grand mal seizure in an elderly man with Down syndrome. Orthop Rev (Pavia) 2010;2:e10. [Google Scholar | PubMed]
- 16.Cabanela ME, Weber M. Instructional course lecture: Total hip arthroplasty in patients with neuromuscular disease. J Bone Joint Surg Am 2000;82:426-32. [Google Scholar | PubMed]
- 17.Jolles BM, Bogoch ER. Posterior versus lateral surgical approach for total hip arthroplasty in adults with osteoarthritis. Cochrane Database Syst Rev 2006;3:CD003828. [Google Scholar | PubMed]
- 18.Aggarwal VK, Iorio R, Zuckerman JD, Long WJ. Surgical approaches for primary total hip arthroplasty from Charnley to now: The quest for the best approach. JBJS Rev 2020;8:e0058. [Google Scholar | PubMed]
- 19.Hernigou P, Filippini P, Flouzat-Lachaniette CH, Batista SU, Poignard A. Constrained liner in neurologic or cognitively impaired patients undergoing primary THA. Clin Orthop Relat Res 2010;468:3255-62. [Google Scholar | PubMed]
- 20.Song JH, Kwon WH, Oh SB, Moon KH. Use of a constrained acetabular liner to prevent and treat recurrent dislocation after total hip replacement arthroplasty. Orthop Surg 2020;12:2004-2012. [Google Scholar | PubMed]
- 21.Callaghan JJ, O’Rourke MR, Goetz DD, Lewallen DG, Johnston RC, Capello WN. Use of a constrained tripolar acetabular liner to treat intraoperative instability and postoperative dislocation after total hip arthroplasty: A review of our experience. Clin Orthop Relat Res 2004;429:117-23. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2025 Melorheostosis: A Rare Case Report with Pelvic and Lumbar Involvement
August 1, 2025 Melorheostosis: A Rare Case Report with Pelvic and Lumbar Involvement June 1, 2025 Successful Management of Atypical Bilateral Galeazzi Fractures with Unique Dorsal Displacement: A Case Report
June 1, 2025 Successful Management of Atypical Bilateral Galeazzi Fractures with Unique Dorsal Displacement: A Case Report April 1, 2025 Unveiling the Uncommon: Ewing Sarcoma Cranium – A Rare Clinical Vignette
April 1, 2025 Unveiling the Uncommon: Ewing Sarcoma Cranium – A Rare Clinical Vignette May 10, 2023 A Rare Case of Melorheostosis Presenting with Extra-osseous Lesions Around the Knee: Case Report
May 10, 2023 A Rare Case of Melorheostosis Presenting with Extra-osseous Lesions Around the Knee: Case Report