
Head-stem dissociation is a previously undocumented complication of the Exeter V40 stem and this case report provides clinicians an insight into the successful management of this rare complication.
Dr. Sahil Shet, Registrar in Trauma and Orthopaedics, MbBChBAO MRCS MCh, Cork University Hospital, Cork, Ireland. E-mail: sahilshet@rcsi.ie
Introduction: In this article, we report a unique case of head-stem dissociation in a metal-on-metal total hip replacement which utilized an Exeter stem. Although metallosis and pseudotumor formation are well recognized complications of metal-on-metal hip replacements, head-stem dissociations are rare with few being reported in literature. To the best of our knowledge, this case report is the first to report this occurrence in an Exeter stem.
Case Report: A 76-year-old male presented to the emergency department with pain and discomfort in his left hip triggered by a twisting movement while getting into bed. The patient described a “pop” in his hip upon turning and reported mild ongoing discomfort in his left hip for the past 4 weeks before this acute presentation. X-rays and Metal artifact reduction sequence magnetic resonance image (MARS) revealed head-stem dissociation along with pseudotumor formation. The patient successfully underwent a two stage revision with no perioperative complications.
Conclusion: This case report, to the best of our knowledge, is the first to report catastrophic failure of a metal-on-metal hip caused by trunnionosis and subsequent head-stem dissociation. We report successful management of this unique case and hope to highlight the complexities and challenges associated with metal-on-metal THR. This case report is aimed at raising clinical awareness of this rare complication which requires expert management for a successful outcome.
Keywords: Trunnionosis, Metallosis, pseudotumor.
Primary total hip arthroplasties (THA) are one of the most common elective procedures being performed by orthopedic surgeons worldwide with over 200,000 being performed yearly in the United States of America alone [1,2]. High success rates and an aging global population have made this one of the fastest growing procedures in the USA with a projected increase of up to 70% from 2014–2030 [3]. The goal THA is to restore the normal hip joint anatomy and ultimately, alleviate patient’s symptoms. Despite the success rates, failure can occur due to various reasons including hip instability, prosthetic joint infection, implant loosening, and implant failure or wear. Recently, modular THA systems have fallen into favor due to their ability to allow the surgeon to make fine adjustments in order restore the natural biomechanics of the hip joint as closely as possible [4]. Over the years, the design of the THA has undergone significant changes with different materials trialled to reduce the risk of implant wear and instability. Materials including stainless steel, titanium alloys, zirconia, cobalt chrome alloys, ultra high molecular weight polyethylene have been utilized with configurations such a metal-on-metal (MoM), metal-on-polyethylene (MoP), ceramic-on-polyethylene (CoPE), ceramic-on-ceramic (CoC) ceramic-on-metal (CoM) being possible [5]. The MoM configuration had high hopes of resolving some of the issues associated with THA including polythene wear while providing greater joint range of motion and stability with large diameter heads [6]. Unfortunately, significant serious complications were noted with these configurations including metallosis, trunnionosis, metal ion toxicity and pseudotumor formation. Some studies reported failure rates of up to 30% at 7 years [7]. The MITCH TRH modular system was a popular system for THA and was utilized worldwide between 2006 and 2011. Unfortunately, there were early reports of failure and thus the system was recalled discontinued in 2012. Trunnion failure, head-neck dissociation, and fretting were seen, especially in the Accolade I TMZF uncemented stems when used in combination with the MITCH TRH modular head [8]. From our review of the literature, there has not yet been a reported failure of the popular Exeter V40 cemented femoral stem in this fashion. While stem fractures have been reported [9], fretting and corrosion of the trunnion with associated head-stem dissociation in a MoM hip has yet to be reported until now.
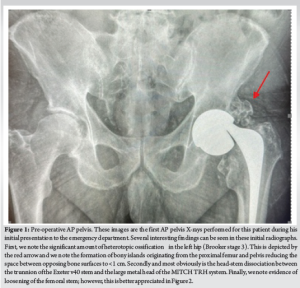
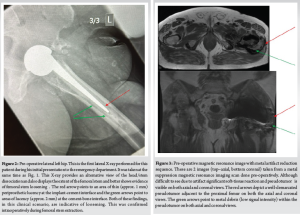
A 76 year old with a BMI of 36 kg/m2 male presented to the Emergency Department with left-sided hip pain and discomfort after performing a “twisting” motion of his hip while getting into bed. He described a “popping” sensation in his left hip upon doing this movement and immediately experienced a sharp pain and was unable to weight bear on that side. The patient described a discomfort in that left hip for the last 4 weeks before this acute presentation, which was not triggered by any trauma/injury. This patient had a MoM THA that was performed 16 years ago for osteoarthritis. He had had a successful outcome until now and denied any post-operative complications after the procedure. The MITCH TRH Modular head with an Exeter V40 cemented stem was used and the operation performed by an experienced consultant orthopedic surgeon. The patient’s medical history includes atrial fibrillation, coronary stenting, high BMI (36 kg/m2) hypertension, hypercholesterolemia, and bilateral total knee replacements. The patient is a non-smoker with occasional alcohol intake and mobilizes independently without walking aids at baseline. Clinical examination at the presentation revealed a shortened limb on the left side held in the neutral position. The patient was unable to straight leg raise due to pain and had a normal neurological and vascular examination. No visible signs of injury or trauma were present, and a systems examination was normal. The patient was admitted under the care of the orthopedic team, and investigations, including X-rays, MARS scan, laboratory tests (Full blood count, renal profile, C-reactive protein, coagulation profile, metal ion levels), and electrocardiogram, were ordered. X-rays (Figs. 1 and 2) revealed head-stem dissociation in a MoM hip configuration. Blood investigations were within normal levels and without any evidence of infection. Of note, metal ion levels are still in process. A MARS scan was conducted which revealed a subfascial 7cm × 7 cm × 10 cm collection posterior to the THA (Fig. 3.)
This case was discussed at the orthopedic department trauma MDT and a revision hip arthroplasty surgeon took lead on the case. Initially, a full revision of all components was planned in a one-stage fashion, however, the extent of metallosis noted intraoperatively prompted a change in plan to a 2-stage style revision with early implantation of final components on the condition of negative culture swabs from the affected hip.
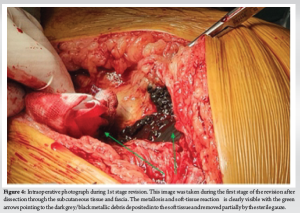
The operation was carried under general anesthetic due to difficulty in spinal anesthesia. The patient was placed laterally on the operating table with front and back supports and given 1 g IV tranexamic acid and 1.5 g IV cefuroxime before skin incision. Skin preparation and draping were done in the standard fashion and a posterior approach was used to expose the hip joint. Extensive metallosis was noted covering muscle and fascial tissue (Fig. 4) which was carefully debrided during the surgery. Examination of the stem revealed asymmetrical wear patterns of the trunnion and oxidation of the neck and body of the stem (Fig. 5). All original components were explanted, and a non-articulating cement spacer was inserted into the joint. Although no pus was noted in the joint, the concern of infection remained, and multiple samples of tissue and fluid were taken for culture and sensitivity throughout the procedure.

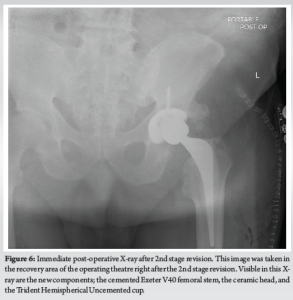
The surgical wound was closed in layers in a standard fashion with PDS sutures and skin clips. Following a confirmation of negative tissue samples and cultures swabs from the microbiology laboratories, opinion was sought from the infectious diseases team regarding 2nd stage revision. Given that the patient had negative culture swabs and pre-operative inflammatory markers were normal, decision was made to proceed with early 2nd stage revision 1 week after the 1st stage procedure. The same surgical incision was used to regain access to the hip joint. The cement spacer was removed and the final components (cemented Exeter v40 stem size 1 with 50 mm offset, 36 mm standard ceramic head, 58 mm Trident Hemispherical Uncemented cup with 36 mm 10° eccentric insert) were implanted (Fig. 6). The hip was stable in all ranges of motion, and leg lengths were equal. The surgical wound was closed again in a similar fashion to the 1st stage procedure with PDS sutures and skin clips.
Postoperatively the patient was mobilized on Day 1 and had a short, uncomplicated stay in the hospital.
Over the last few decades, modular THA systems have gained popularity and now are widely in as they allow the surgeon to tailor the final components based on the joint in question. Advantages include improved soft-tissue tensioning, restoration of the femoral offset, and more accurate restoration of leg lengths. Despite the advantages, there are also downsides to the modular THA systems being used today. In addition to the known complications of THA, modular systems have an additional complication of dissociation between the modular components [10]. Failure of components at the head-neck junction occurs due to fretting and corrosion which in turn are affected by the material combination, implantation time, and flexural rigidity. Mixed alloy couples display a higher incidence of corrosion and longer implantation times allow for more fretting and corrosion to occur [11]. Multiple other factors that play a role in trunnion failure have also been described including trunnion flexibility, trunnion design, and trunnion surface finish [12]. In addition, a high BMI which puts a greater load on the femoral head-trunnion interface can to faster rates of corrosion and subsequent failure. Male gender and age over 65 are also potential risk factors, however, the reason for this is unknown [8]. The THA may fail for reasons other than trunnionosis; however, MoM articulations were seen to have catastrophic failures. MoM hips generate metal debris over time and these particles can cause a host of adverse reactions. These reactions are collectively known as adverse reaction of metal debris and include aseptic lymphocyte-dominant vasculitis-associated lesions, pseudotumors, metallosis, and immunotoxicity [13]. Interestingly in a retrieval study conducted by Lanting et al. MoM hips were found to have a 5 times higher amount of material loss from the trunnion, compared to MoP hips independent of the head diameter [12]. As a result, it is likely that the bearing surface (MoM) contributed to the trunnionosis in the case presented in this article. Classically, using large-diameter heads was thought to improve the stability of the prosthesis, however, in the context of MoM articulations, using large-diameter heads led to increased wear rates and eventual failure. Elkins et al. investigated the relationship between head size and stability as well as wear of the trunnion in MoM hips. They presented their findings at American Academy of Orthopedic Surgeons conference in 2013 and concluded that although stability was improved with larger diameter heads, the rate of trunnion wear was significantly increased. The patient in this case report also had a large diameter femoral head implanted in his index procedure which likely contributed to the eventual failure of his prosthesis [14]. Despite the volume of research performed on THA failures, the exact cause of trunnionosis remains unclear. In addition to MoM articulation, taper design and material have been suggested as causes of trunnionosis. Although the incidence of metallosis and trunnionosis in MoM articulations is well published in the literature, there has been no evidence to suggest that the V40 taper design or the Exeter stem used in this case result in increased metal ions levels or increased rates of trunnionosis. Therefore, the finding of corrosion, trunnion fretting and significant metallosis in this case is unusual and represents an interesting case finding [15].
Stem fractures in the Exeter V40, despite being exceedingly rare, have been well documented. However, this case represents the first incidence of head-stem dissociation of the Exeter V40 stem reported in the literature. Although previous stems, particularly the Accolade I, have been reported to have trunnion failure with resultant head-stem dissociation, the Exeter v40 stem is not known to have this particular complication. The patient in this case had a number of risk factors for trunnionosis and head-stem dissociation including high BMI, MoM implant, age over 65, and male gender. However, despite these risk factors, this remains an extremely rare and unusual complication. As a result, we believed publication of this case report would allow guidance to surgeons on the management of patients with this complication. This case sheds light on how trunnionosis presents clinically. The intraoperative images provided serve as a valuable resource, aiding surgeons in gaining insight and familiarity with potential scenarios they may face during the surgical treatment of similar patients.
This article details a previously undocumented complication of the very popular Exeter v40 cemented femoral stem. Although this stem has been in use for over 20 years, there have been no documented head-stem dissociations with this stem in that time period. As a result, this case report provides readers with a novel complication in this femoral stem and gives insight into the successful management of this exceeding rare issue.
References
- 1.Fingar KR, Stocks C, Weiss AJ, Steiner CA. Most frequent operating room procedures performed in U.S. Hospitals, 2003-2012. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville, MD: Agency for Healthcare Research and Quality (US); 2014. [Google Scholar | PubMed]
- 2.Patel I, Nham F, Zalikha AK, El-Othmani MM. Epidemiology of total hip arthroplasty: Demographics, comorbidities and outcomes. Arthroplasty 2023;5:2. [Google Scholar | PubMed]
- 3.Schwartz AM, Farley KX, Guild GN, Bradbury TL. Projections and epidemiology of revision hip and knee arthroplasty in the United States to 2030. J Arthroplasty 2020;35:S79-85. [Google Scholar | PubMed]
- 4.Park CW, Lim SJ, Park YS. Modular stems: Advantages and current role in primary total hip arthroplasty. Hip Pelvis 2018;30:147-55. [Google Scholar | PubMed]
- 5.Chethan KN, Bhat NS, Zuber M, Satish Shenoy B. Evolution of different designs and wear studies in total hip prosthesis using finite element analysis: A review. Cogent Eng 2022;9:2027081. [Google Scholar | PubMed]
- 6.McMinn D, Daniel J. History and modern concepts in surface replacement. Proc Inst Mech Eng H 2006;220:239-51. [Google Scholar | PubMed]
- 7.Mancino F, Finsterwald MA, Jones CW, Prosser GH, Yates PJ. Metal-on-metal hips: Ten-year clinical and radiographic outcomes of the ADEPT metal-on-metal hip resurfacing and modular total hip arthroplasty. J Clin Med 2023;12:889. [Google Scholar | PubMed]
- 8.Wylde CW, Jenkins E, Pabbruwe M, Bucher T. Catastrophic failure of the accolade I hip arthroplasty stem: A retrieval analysis study. Hip Int 2020;30:481-7. [Google Scholar | PubMed]
- 9.Garala K, Laios T, Lawrence T. A report of 3 cases of Exeter V40 stem fracture and explanation of possible causes. Hip Int 2018;28:NP1-5. [Google Scholar | PubMed]
- 10.Parker SJ, Khan W, Mellor S. Late Nontraumatic dissociation of the femoral head and trunnion in a total hip arthroplasty. Case Rep Orthop 2015;2015:738671. [Google Scholar | PubMed]
- 11.Goldberg JR, Gilbert JL, Jacobs JJ, Bauer TW, Paprosky W, Leurgans S. A multicenter retrieval study of the taper interfaces of modular hip prostheses. Clin Orthop Relat Res 2002;401:149-61. [Google Scholar | PubMed]
- 12.Lanting BA, Teeter MG, Howard JL, MacDonald SJ, Van Citters DW. Metal-on-metal compared with metal-on-polyethylene: The effect on trunnion corrosion in total hip arthroplasty. J Arthroplasty 2017;32:2574-9. [Google Scholar | PubMed]
- 13.Davis TP. Metal-on-metal hip arthroplasty: A comprehensive review of the current literature. Cureus 2023;15:e48238. [Google Scholar | PubMed]
- 14.Pastides PS, Dodd M, Sarraf KM, Willis-Owen CA. Trunnionosis: A pain in the neck. World J Orthop 2013;4:161-6. [Google Scholar | PubMed]
- 15.Singh R, Manoharan G, Craig P, Collier S, Shaylor P, Sinha A. Blood metal ions after hybrid metal-on-polyethylene Exeter-trident total hip replacement. J Orthop Traumatol 2016;17:149-53. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2025 Progressive Loosening in Metal-on-Metal Total Hip Arthroplasty after Fifteen Years of Effective Function: Two Case Reports
August 1, 2025 Progressive Loosening in Metal-on-Metal Total Hip Arthroplasty after Fifteen Years of Effective Function: Two Case Reports September 1, 2024 Metallosis Following Non-Metal-on-Metal Hip Arthroplasty: A Case Report and Review
September 1, 2024 Metallosis Following Non-Metal-on-Metal Hip Arthroplasty: A Case Report and Review January 1, 2026 Severe Metallosis-Induced Osteolysis and Polyethylene Liner Dissociation as a Cause of Total Knee Replacement Failure
January 1, 2026 Severe Metallosis-Induced Osteolysis and Polyethylene Liner Dissociation as a Cause of Total Knee Replacement Failure August 1, 2025 Unexplained Pseudotumor Formation in Ceramic-on-ceramic Hip Bearings: A Case Report
August 1, 2025 Unexplained Pseudotumor Formation in Ceramic-on-ceramic Hip Bearings: A Case Report