
By providing a successful alternative to traditional metallic implant-based fixation, our technique offers the potential for a significant reduction in the need for reoperations.
Dr. Amyn M Rajani, OAKS Clinic, 707, Panchshil Plaza, N S Patkar Marg, Opposite Ghanasingh Fine Jewels, Next to Dharam Palace, Gamdevi, Mumbai- 400007, Maharashtra, India. E-mail: dramrajani@gmail.com
Introduction: Unicondylar knee replacement (UKR) is a surgical procedure frequently performed to treat medial compartment osteoarthritis, offering advantages such as quicker recovery and preservation of knee kinematics. However, complications can arise, including periprosthetic fractures. Patella fractures in the context of UKR are particularly challenging due to the presence of the implant. Traditional fixation methods often involve metallic implants, which can be associated with complications and the need for reoperations. This report introduces a novel technique for patella fracture fixation using suture tapes, highlighting its potential benefits in reducing reoperation rates and improving patient outcomes.
Case Report: A 68-year-old female patient, with a history of right-sided UKR for medial compartment osteoarthritis and left-sided total knee replacement for grade 4 osteoarthritis, presented with acute right knee pain and swelling after a fall while climbing stairs. An X-ray revealed a displaced transverse patella fracture, although the unicondylar knee implant remained well-fixed. Given the unique complication of a patella fracture in the presence of UKR prosthesis, the patient underwent surgery using a novel fixation technique with suture tapes. This method aimed to provide stable fixation, facilitate early mobilization, and minimize the risks associated with traditional metallic implants.
Conclusion: The successful application of suture tape fixation for a patella fracture in a UKR patient demonstrates an effective alternative to metallic implants. This innovative technique has the potential to reduce reoperation rates, minimize complications, and enhance early mobilization, thereby improving the overall quality of life for patients.
Keywords: Unicondylar knee replacement, patella fracture, suture tape, prosthesis, case report.
Patella fractures are relatively uncommon, accounting for only a small percentage of all fractures. The prevalence of these fractures is between 0.68 and 2.1% [1]. Patella fracture is the second most common periprosthetic fracture of the knee joint after femur fracture [2]. These fractures can present a unique challenge, especially when they occur in patients who have previously undergone joint replacement procedures, such as unicondylar knee replacement (UKR). UKR, a surgical technique designed to replace only one compartment of the knee joint, has gained popularity for the management of isolated unicompartmental knee osteoarthritis. While it offers several advantages, including reduced surgical invasiveness and quicker post-operative recovery, it also introduces a set of complexities in managing complications, particularly fractures of the patella [3]. The patella plays a crucial role in the biomechanics of the knee joint. It articulates with the femur and serves to protect the underlying joint surface while enhancing the mechanical advantage of the quadriceps muscle [4,5]. Patella fractures are typically the result of high-energy trauma, such as a fall or a direct blow to the knee. The management of un-displaced patella fractures has traditionally involved conservative measures, such as immobilization and physiotherapy. However, in some cases, displaced fractures with disruption of extensor mechanism surgical intervention becomes necessary to restore the patellofemoral joint’s function and stability. Patella fractures in the context of UKR represent a unique and intricate clinical scenario that requires careful evaluation and intervention. The mechanism of patella fracture in these patients is multifactorial. It can result from altered biomechanics following UKR, implant design and positioning, and patient-related factors such as bone quality and activity level [6]. This case report aims to shed light on the clinical course, diagnostic challenges, and management of patella fractures post-trauma in a patient of UKR. There is sufficient literature on patella fracture post-total knee replacement (TKR) with well-described classification systems and surgical management but there is a dearth of literature on patella fracture following trauma post-UKR. The significance of this case report lies in its contribution to the growing body of literature on patella fractures in patients with prior UKR. Such cases, although infrequent, underscore the importance of vigilance in assessing the risk of fractures, especially in patients who have undergone joint replacement surgery. Furthermore, the treatment strategies and outcomes in these cases may differ from those in primary patella fractures. Our aim with this case report is to present a novel technique for patella fracture fixation in UKR patients with suture tapes.
Case presentation
A 68-year-old female patient with a medical history of well-controlled diabetes and hypertension who underwent right-sided UKR for medial compartment osteoarthritis and left-sided TKR for grade 4 osteoarthritis presented with a chief complaint of acute right knee pain and swelling following a fall while climbing stairs. The fall rendered her unable to bear weight on the right leg without support. On examination, the right knee was noted to be swollen, red, and tender, with a significantly restricted range of motion (ROM) and an inability to actively extend the knee.
Imaging
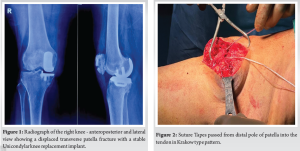
An X-ray of the right knee revealed a displaced transverse patella fracture (Fig. 1). Remarkably, the unicondylar knee implant remained well-fixed, emphasizing the unique nature of this complication in the presence of an implanted prosthesis. The fracture’s displacement and the proximity of the implant posed diagnostic and management challenges.
Management
Given the patient’s discomfort and limited mobility, surgical intervention was deemed necessary. A multidisciplinary team, including orthopedic surgeons and anesthesiologists, carefully planned the procedure. The surgical approach involved open reduction and internal fixation (ORIF) of the patella fracture, taking into account the stability of the unicondylar knee implant.
Surgical technique
The transverse patella fracture was fixed using the following technique:
- Krakow-type sutures
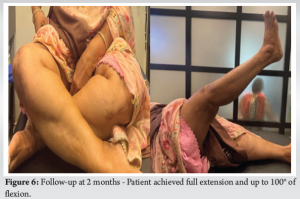
- Initially, we utilized Krakow-type sutures to secure the proximal end of the patellar tendon. Two suture tapes were employed for this purpose. Sutures were passed from the distal pole of the patella into the tendon in a Krakow-type pattern (Fig. 2).
- The four free ends of these suture tapes were organized into a specific configuration, comprising one medial, two central, and one lateral component.
- Creation of tunnels
- Subsequently, we proceeded to address the fracture by drilling three parallel tunnels through the proximal fragment in a distal to proximal-fashion. A 1.8 mm beath pin was employed for this purpose (Fig. 3).

- The previously prepared fiber tapes were then passed through these drilled holes using a suture relay technique. The lateral fiber tape was directed through the lateral tunnel, the medial fiber tape through the medial tunnel, and the two central fiber tapes through the central tunnel.
- Reduction and fixation [7] (Figs. 4 and 5)
- With the fiber tapes in place, we initiated the reduction of the fracture fragments by pulling the ends of the fiber tapes through the proximal fragment. This reduction maneuver was essential for maintaining the integrity of the articular surface.
- Verification of the reduction was performed under the guidance of an image intensifier to ensure the optimal alignment of the fracture fragments.
- Subsequently, we tied the lateral and one of the central fiber tapes with half hitches, with the knee positioned at a 30° angle of flexion. During this process, traction was applied to the remaining two free tapes to maintain the proximity of the fracture fragment.
- The remaining central tendon and the medial tape were then securely tied with half hitches, completing the fixation process.
- The patellar retinaculum was then sutured with a 2–0 fiber wire.
Periprosthetic patella fractures, particularly following knee replacement, present a unique clinical challenge [8]. These fractures can be traumatic or atraumatic, with resurfaced patellae being more commonly involved. While management approaches for such fractures are well-established post-TKR, there is a noticeable paucity of literature addressing periprosthetic patella fractures in patients with UKR. Various techniques for fracture fixation have been described, such as tension band wiring, mesh plates, cannulated screws, and cerclage wiring. However, it’s important to note that these approaches are not without complications, and periprosthetic patella fractures remain associated with high rates of adverse outcomes, necessitating reoperations. Keating et al. reported non-unions in patients treated with ORIF for transverse displaced patella fractures [1], and Chun et al. identified cases of osteonecrosis, patellar subluxation, persistent pain, and extensor lag in patients treated operatively for displaced patella fractures [9].
In light of the complications associated with conventional treatment methods and with a focus on restoring the extensor mechanism and achieving early recovery of ROM, we present a novel technique for patella fracture fixation involving the use of suture tapes.
Current management strategies for transverse patella fractures primarily rely on metallic implants. While they have shown good clinical results, complications related to symptomatic hardware are not uncommon. The use of suture tapes along with a tensioning device has emerged as an effective alternative for the surgical treatment of transverse patellar fractures. Patients have reported minimal discomfort related to the presence of suture tape, in contrast to the pain and discomfort often associated with metallic implants, which can lead to requests for removal surgery in some cases. The tensioning device allows for precise control over the tension applied to the suture tape and knots. It enables uniform cerclage around the patellar bone, offering enhanced resistance to fracture reduction and optimal compression of fracture fragments when compared to the use of traditional stainless steel wire. Suture tape’s radiolucency properties provide improved visibility for radiographic fracture reduction assessment during both intraoperative and post-operative follow-up, minimizing potential interposition and artifacts that can occur with metallic hardware [10]. Although the use of this technique may be limited by patient comfort due to the need for a knee immobilizer in extension for 6 weeks post-surgery as in our case, the advantages outweigh the disadvantages. In comparison with traditional stainless steel wire cerclage, suture tape and the specialized tensioner device are more expensive. However, the reduction in the risk of reoperations, particularly in arthroplasty cases (TKR or UKR), justifies this cost.
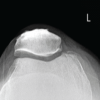
In our specific patient, who had an intact UKR implant, our primary goals were to prevent overstuffing of the knee joint with metallic implants, facilitate fracture consolidation, and promote early mobilization to prevent knee stiffness. Sutures were removed at 2 weeks, and the knee brace was strictly maintained for 6 weeks post-surgery. At the 6th week, we initiated full weight-bearing and ROM exercises. By the end of the 8th week, we had achieved full extension and achieved up to 100° of flexion (Fig. 6).
This innovative technique for patella fracture fixation offers significant promise in reducing complications and reoperations, particularly in the context of UKR. Further research and follow-up studies are warranted to assess the long-term outcomes and overall benefits of this approach.
Traumatic patella fractures occurring in the context of UKR present a notable challenge, primarily due to the associated extension lag, and the limited use of metallic implants in these scenarios. In such cases, the primary objectives should include achieving fracture consolidation with a stable construct, minimizing the need for multiple surgeries, and enabling early mobilization through effective rehabilitation protocols. Our case report introduces a novel and effective technique for the fixation of periprosthetic patella fractures in UKR patients, without relying on metallic implants. This innovative approach, which incorporates suture tapes and a tensioning device, not only ensures fracture consolidation but also reduces the risk of symptomatic hardware complications. Our results demonstrate a favorable functional outcome, with the fracture consolidating within 8 weeks post-surgery. By providing a successful alternative to traditional metallic implant-based fixation, our technique offers the potential for a significant reduction in the need for reoperations. This innovative approach aligns with the broader goal of optimizing patient care, minimizing complications, and facilitating early mobilization, ultimately improving the overall quality of life for patients with periprosthetic patella fractures following UKR.
Our technique presents a successful alternative to traditional metallic implant-based fixation, potentially reducing the need for reoperations significantly. This innovative approach aims to optimize patient care by minimizing complications and facilitating early mobilization, ultimately enhancing the overall quality of life for patients with periprosthetic patella fractures following UKR.
References
- 1.Keating EM, Haas G, Meding JB. Patella fracture after post total knee replacements. Clin Orthop Relat Res 2003;416:93-7. [Google Scholar | PubMed]
- 2.Chalidis BE, Tsiridis E, Tragas AA, Stavrou Z, Giannoudis PV. Management of periprosthetic patellar fractures. A systematic review of literature. Injury 2007;38:714-24. [Google Scholar | PubMed]
- 3.Bourne RB. Fractures of the patella after total knee replacement. Orthop Clin North Am 1999;30:287-91. [Google Scholar | PubMed]
- 4.Masoni V, Giustra F, Bosco F, Lo Carmine L, Capella M, Cacciola G, et al. Periprosthetic patella fractures in total knee replacement and revision surgeries: How to diagnose and treat this rare but potentially devastating complication-a review of the current literature. Eur J Orthop Surg Traumatol 2023;33:2765-72. [Google Scholar | PubMed]
- 5.Desouza C, Shetty V. Beyond one step: Unveiling optimal approach for bilateral knee arthroplasty - a comprehensive meta-analysis. Arch Orthop Trauma Surg 2024;144:3631-9. [Google Scholar | PubMed]
- 6.Nan SK, Li HF, Zhang D, Lin JN, Hou LS. Internal fixation and unicompartmental knee arthroplasty for an elderly patient with patellar fracture and anteromedial osteoarthritis: A case report. World J Clin Cases 2021;9:3919-26. [Google Scholar | PubMed]
- 7.Rajani AM, Punamiya MS, Rajani K, Rajani K. Modified technique for patellar tendon repair post-total knee arthroplasty: A case report. J Orthop Case Rep 2020;10:15-8. [Google Scholar | PubMed]
- 8.Desouza C, Antao N. Potpourri - Recent and relevant literature in periprosthetic fractures around the knee. J Clin Orthop 2024;9:52-6. [Google Scholar | PubMed]
- 9.Chun KA, Ohashi K, Bennett DL, El-Khoury GY. Patellar fractures after total knee replacement. AJR Am J Roentgenol 2005;185:655-60. [Google Scholar | PubMed]
- 10.Monaco E, Bruni G, Daggett M, Saithna A, Cardarelli S, Proietti L, et al. Patellar fracture fixation using suture tape cerclage. Arthrosc Tech 2020;9:e783-9. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Single Peg Patellar Component Fracture in Total Knee Replacement: A Case Report
March 1, 2026 Single Peg Patellar Component Fracture in Total Knee Replacement: A Case Report March 1, 2026 Salvage of a Broken Magnetic Tibia Nail with Plate Fixation Without Nail Removal: A Case Report
March 1, 2026 Salvage of a Broken Magnetic Tibia Nail with Plate Fixation Without Nail Removal: A Case Report March 1, 2026 Clavicle Fracture Non-Union in a 3-Year-Old Child: A Case Report and Literature Review
March 1, 2026 Clavicle Fracture Non-Union in a 3-Year-Old Child: A Case Report and Literature Review February 1, 2026 Intraoperative Diagnosis and Management of Testicular Dislocation During Pelvic Fracture Fixation: A Report of Two Cases and Literature Review
February 1, 2026 Intraoperative Diagnosis and Management of Testicular Dislocation During Pelvic Fracture Fixation: A Report of Two Cases and Literature Review