
Reduction of complications of metal tension band wiring using fibre tape having equal strength and lesser damage to retinaculum while passing under the fragment plus a low profile MRI compatible implant.
Dr. Ravi Modi, Department of Orthopaedic Surgery, Dr. D Y Patil Hospital, Nerul, Navi Mumbai - 400706, Maharashtra, India. E-mail: modiravi1997@yahoo.co.in
Introduction: Post-operative complications related to hardware, particularly symptoms caused by it, such as implant impingement, wire breakage, and skin infection are frequently reported following surgical management of patellar fractures with stainless steel wires. As a potential solution, some researchers have advocated for the use of non-absorbable sutures for fracture fixation. This study aims to investigate the clinical and radiological outcomes of patients treated with fiber taping as an alternative technique.
Materials and Methods: We conducted a retrospective evaluation of 20 patients diagnosed radiographically with displaced patellar fractures (including transverse, poles, and severely comminuted). These patients underwent tension band technique with the help of high strength polyethylene fiber tape. Clinical and radiological outcomes were meticulously assessed, with specific attention to union time, complications, and functional outcome assessed by the Lysoholm scoring system, all of which were carefully observed and documented.
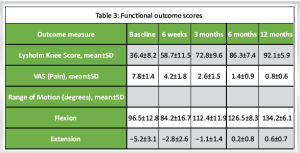
Results: The mean age of the patients was 42.5 ± 14.3 years, and the majority were male (70%). The mean operative time was 68.5 ± 22.4 min. All fractures achieved union without any reported cases of wound complications, infections, loss of reduction, or implant failure. The mean Lysholm Knee Score improved from 36.4 ± 8.2 at baseline to 92.1 ± 5.9 at 12-month post-surgery. The visual analogue scale for pain decreased from 7.8 ± 1.4 at baseline to 0.8 ± 0.6 at 12 months. The mean range of motion improved from 96.5° ± 12.8° of flexion and −5.2° ± 3.1° of extension at baseline to 134.2° ± 6.1° of flexion and 0.6° ± 0.7° of extension at 12 months.
Conclusion: Our investigation into a modified tension band technique using fiber tape sutures revealed encouraging clinical outcomes, marked by minimal complications. The adoption of fiber tape as a substitute for metal wire counterparts in patellar fracture treatment shows potential for reducing hardware related symptoms and shows lesser morbidity.
Keywords: Fiber tape, patellar fracture, tension band technique, stainless-steel wire.
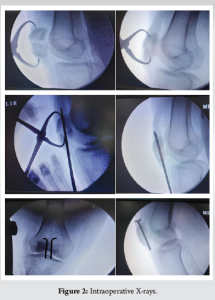
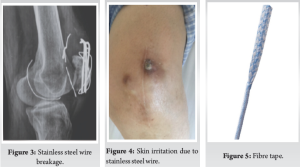
The patella serves as a pivotal component in the biomechanical function of the knee extensor apparatus [1]. Fractures of the patella have the potential to disrupt this mechanism, particularly when combined with incongruent posterior articular surfaces, leading to persistent issues like discomfort arising from femoropatellar arthritis [2,3]. Patellar fractures commonly stem from two primary mechanisms: Direct impact on the anterior knee or indirect injury resulting from eccentric contraction of the quadriceps muscle [4]. Surgical intervention becomes necessary in about one-third of patients affected by these fractures. Tension band wiring using stainless-steel wires has long been considered the gold standard for surgically managing displaced patellar fractures (Fig. 1 and 2) This technique effectively converts tension from muscle pull into compression at the fracture’s articular side, promoting improved fracture union by providing absolute stability through interfragmentary compression in bending fractures. However, its widespread use has been subject to debate due to the high incidence of resurgery rates attributed to issues such as implant impingement, skin infection, and wire breakage [5,6] (Fig. 3 and 4). Also for multifragmented stellate fracture, where encircle is required, SS wires require multiple passes through retinaculum with 4-mm-thick wire passer which is more traumatic. An alternative to traditional metal wire for patellar fracture fixation is non-absorbable suture, such as fiber tape (Fig. 5), which has been shown to yield similar outcomes with a reduced complication rate and comparable strength in biomechanical studies. Multiple passes in encirclage method for comminuted fractures with fiber tape is less traumatic with 2-mm needle. Research conducted by Arthrex found that fibreTape exhibited significant strength at 3 mm elongation and shows good loop integrity [7].

This study, conducted at a sole tertiary care teaching hospital in Navi-Mumbai, India, employed an open-label, retrospective study All procedures adhered strictly to ethical standards outlined by both the institutional and national committees on human experimentation, in alignment with the Helsinki Declaration of 1975, with revisions in 2013. The Institutional Ethics Committee granted approval for this study, denoted by the reference number DYP/IECBH/2023/249. Informed consent was duly obtained from every individual participant enrolled in the study. Over the period from October 2022 to October 2023, a cohort of 20 patients diagnosed with a patella fracture was enlisted. The study encompassed individuals with patella fracture treated with fiber tape aged 18 years or above, and of either gender. Exclusion criteria for this study encompassed individuals aged 18 years or below, those with open injuries, neurovascular deficit, or chronic kidney disease. Before initiating the treatment, the investigators thoroughly assessed the clinical condition, conducted relevant investigations, and examined radiological scans to understand the fracture pattern and overall clinical profile of the patients. Following surgery, a long knee brace was given, before progressing to mobilization exercises with a hinge-knee brace. At follow-ups, the functional outcome was assessed with the Lysholm scoring system, visual analogue scale (VAS) range of motion with a goniometer, along with bone healing status from radiographs.
Operative steps
The procedural steps closely resemble those of the classic tension band wiring technique, with no specialized instruments required beyond the standard orthopedic trauma instruments set and a fiber tape alongside two 2.0-mm Kirshner wires. Carefully anatomically reduce the transverse fracture and secure it using a pointed reduction forceps, ensuring confirmation of reduction through fluoroscopy.
- Insert two parallel Kirschner wires across and proximal and distal fragments (Fig. 6).

- Thread the fiber tape in a figure of 8 manner across quadriceps tendon or patellar tendon and below the two K wires.
- After crossing over the anterior surface of patella in figure of 8 manner, Fiber tape is tied tightly with multiple reverse half hitches at superolateral region of patella, until the desired compression is achieved at the fracture site. This is followed by burying the knot under retinaculum. The torn retinaculum is repaired with absorbable suture.
- Trim the ends of the K-wires.
- Bend the ends of the K wires posteriorly.
- Conclude the procedure by suturing the retinaculum.
In comminuted fractures where encirclage is preferred, the fiber tape is initially threaded beneath the patellar tendon before being wrapped circumferentially around the patella bone. Utilizing a tensioner, the fiber tape is then tensioned to a force of 70–90 pound force (Fig. 6). Subsequently, the reduction is assessed intraoperatively, knots are securely buried under the retinaculum, and excess is trimmed after checking the stability of the reduction by performing flexion and extension movements of the knee (Fig. 7).
Rehabilitation
Following the surgical procedure, the knee is secured in a long knee brace for 4 weeks, with suture removal scheduled at 14 days. Partial weight bearing with assistance is permitted after 2 weeks. Subsequent check-ups occur at 3-week and 6-week post-surgery. At 4 weeks, range of motion exercises is commenced with a focus on restoring active knee flexion. Rehabilitation progresses with active flexion movements at 5 weeks, culminating in the conclusion of care at 12-week post-surgery (Fig. 8-10).
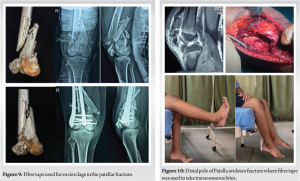
Table 1 provides an overview of the study population’s key demographic characteristics, including age, gender, body mass index (BMI), mechanism of injury (direct impact or indirect), and fracture patterns (transverse, pole, or severely comminuted).
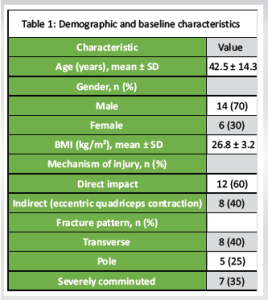
Table 2 summarizes the surgical parameters, such as the type of suture material used (polyethylene fiber tape), the average number of sutures employed, the surgical approach (open in all cases), and the mean duration of the procedure.

Table 3 presents the functional outcome scores at various time points, including baseline (pre-operative) and follow-up assessments at 6-week, 3-month, 6-month, and 12-month post-surgery. The outcome measures included are the Lysholm Knee Score (a widely used knee-specific functional assessment tool), VAS for pain, and range of motion (flexion and extension) measured in degrees. There were no reported complications or revisions such as wound complications, infections, loss of reduction, implant failure, or required revision surgery.
Operative intervention is necessary for every unstable patellar fracture. Tension band wiring, aligning with AO principles, stands as the most widely accepted technique for treating displaced patellar fractures. However, various other methods combining fixation techniques such as K-wires, screws, and cerclage wiring have been documented. Internal fixation is crucial for maintaining fracture reduction until complete healing is achieved, while conventional stainless-steel wires can offer stability, their use often leads to symptomatic hardware and other complications [8]. Consequently, alternative materials with superior tensile strength, as demonstrated in biomechanical studies, have been investigated. Fiber tape, a braided tape shaped polyblend suture, exhibits a tensile strength exceeding 540N, surpassing the 494 N strength of 18 gauge steel wires. Furthermore, testing with cadaveric tendons revealed a pull through force of approximately 189 N for fiber tape, Notably displacement of hardware with stainless-steel wires, resulting in hardware prominence [9,10]. Utilizing fiber tape eliminates the need for implant removal due to skin impingement, addressing a common issue associated with metallic wires. Furthermore, fiber tape exhibits resilience without fatigue, lesser tissue damage, minimizing the risk of implant failure often observed with metal wire breakage and if encirclage is the treatment of choice then it is MRI compatible also [10,11]. Moreover, unlike fixation with metallic wires, fiber tape can be employed not only for simple or comminuted patellar fractures but also as an effective fixation method for distal pole avulsion fractures (Fig. 10-12). However, it is worth noting that the tightness of the fixation knot is surgeon dependent, posing a potential drawback. This issue can be addressed by implementing multiple sequential tightening of 3–4 reverse half hitches on alternating post knots to ensure optimal fixation [12,13]. In our study, we observed a notable decrease in the number of patients requiring re operation, resulting in reduced strain on resources and financial benefits for the patients.

Complications
There were no medical complications encountered during surgery or the immediate post-operative period [14]. None of the patients experienced any symptomatic hardware, skin complications, delayed, or non-union.
Limitations of the study
This study has inherent limitations, such as its single-center setting and relatively small sample size. To overcome these limitations, future studies should aim to include a larger and more diverse sample size, implement an extended follow-up period, and employ a rigorous study design. These measures will help to further validate the potential benefits of utilizing fiber tape for the treatment of patellar fractures.
Despite the constraints of our small cohort, our findings indicate that employing a fiber tape offers a viable alternative for treating patellar fractures. It circumvents the complications associated with stainless steel wire fixation, potentially diminishing the requirement for revision surgeries due to implant failure or impingement.
Fiber tape for tension and wiring is advantageous as it lessens soft-tissue complications like damaged to retinaculum skin irritation wire breakage and infection. Fiber tape is MRI compatible thus no need of implant removal after Bony union. Individual smaller fragments can be addressed in fiber tape especially in communited fracture.
References
- 1.Loudon JK. Biomechanics and pathomechanics of the patellofemoral joint. Int J Sports Phys Ther 2016;11:820-30. [Google Scholar | PubMed]
- 2.Vedel JO, Vistrup S, Larsen P, Elsoe R. Altered long-term health-related quality of life in patients following patella fractures: A long-term follow-up study of 49 patients. Eur J Trauma Emerg Surg 2018;44:707-16. [Google Scholar | PubMed]
- 3.Dy CJ, Little MT, Berkes MB, Ma Y, Roberts TR, Helfet DL, et al. Meta-analysis of re-operation, nonunion, and infection after open reduction and internal fxation of patella fractures. J Trauma Acute Care Surg 2012;73:928-32. [Google Scholar | PubMed]
- 4.Kruse M, Wolf O, Mukka S, Brüggemann A. Epidemiology, classification and treatment of patella fractures: An observational study of 3194 fractures from the Swedish fracture register. Eur J Trauma Emerg Surg 2022;48:4727-34. [Google Scholar | PubMed]
- 5.Jirangkul P, Kosiyatrakul A. Abstaining from symptomatic implants of modified tension band wiring by nonabsorbable suture fixation for transverse patella fractures. J Orthop Surg Res 2021;16:367. [Google Scholar | PubMed]
- 6.Weber MJ, Janecki CJ, McLeod P, Nelson CL, Thompson JA. Efficacy of various forms of fixation of transverse fractures of the patella. J Bone Joint Surg Am 1980;62:215-20. [Google Scholar | PubMed]
- 7.Smith ST, Cramer KE, Karges DE, Watson JT, Moed BR. Early complications in the operative treatment of patella fractures. J Orthop Trauma 1997;11:183-7. [Google Scholar | PubMed]
- 8.Tissue Pull-through Resistance of FiberTape® Suture and ... Available from: https://www.arthrex.com/resources/la1-00031-en/tissue-pull-through-resistance-of-fibertape-suture-and-ultratape-side-by-side-biomechanical-comparison-testing [Last accessed on 2024 Jun 08]. [Google Scholar | PubMed]
- 9.Camarda L, La Gattuta A, Butera M, Siragusa F, D’Arienzo M. FiberWire tension band for patellar fractures. J Orthopaed Traumatol 2016;17:75-80. [Google Scholar | PubMed]
- 10.Arthrex Research and Development. Knotted with FiberWire® #2 Versus Knotless with FiberWire® #2 and Knotless with FiberTape®-a Biomechanical Study. United States: Arthrex GmbH; 2016. [Google Scholar | PubMed]
- 11.Camarda L, La Gattuta A, Butera M, Butera M, Siragusa F, D’Arienzo M. FiberWire tension band for patellar fractures. J Orthopaed Traumatol 2016;17:75-80. [Google Scholar | PubMed]
- 12.Najibi S, Banglmeier R, Matta JM, Tannast M. Material properties of common suture materials in orthopaedic surgery. Iowa Orthop J 2010;30:84-8. [Google Scholar | PubMed]
- 13.Gwinner C, Märdian S, Schwabe P, Schaser KD, Krapohl BD, Jung TM. Current concepts review: Fractures of the patella. GMS Interdiscip Plast Reconstr Surg DGPW 2016;5:Doc01. [Google Scholar | PubMed]
- 14.Monaco E, Bruni G, Daggett M, Saithna A, Cardarelli S, Proietti L, et al. Patellar fracture fixation using suture tape cerclage. Arthrosc Tech 2020;9:e783-9. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 6, 2024 Avascular Necrosis of Proximal Tibia Associated with Pathological Fracture – A Rare Entity – A Case Report
August 6, 2024 Avascular Necrosis of Proximal Tibia Associated with Pathological Fracture – A Rare Entity – A Case Report December 1, 2025 Functional and Radiological Outcomes Following Volar Locking Plate Fixation for Distal Radius Fractures: A Prospective Analytical Study
December 1, 2025 Functional and Radiological Outcomes Following Volar Locking Plate Fixation for Distal Radius Fractures: A Prospective Analytical Study January 1, 2026 Early Outcomes of Screwless Press-fit Acetabular Cups in Uncemented Total Hip Arthroplasty: A Prospective Study from Eastern India
January 1, 2026 Early Outcomes of Screwless Press-fit Acetabular Cups in Uncemented Total Hip Arthroplasty: A Prospective Study from Eastern India February 10, 2021 Exchange Nailing as Revision Surgery for Post-operative Non-union of Atypical Femoral Fractures: A Case Report and Treatment Strategy
February 10, 2021 Exchange Nailing as Revision Surgery for Post-operative Non-union of Atypical Femoral Fractures: A Case Report and Treatment Strategy