
An unusual presentation of anterior osteochondroma knee at an unusual site causing mechanical disruption, associated with Patella fractures or tears of the Quadriceps.
Dr. Harsh Mander, Senior Resident, Department of Orthopaedics, Fortis Hospital Mohali, Sector 62, S.A.S. Nagar, Mohali, Punjab, India. E-mail: harshmander@live.com
Abstract
Introduction: Despite osteochondromas being fairly common around the knee, cases causing mechanical disruption and being associated with fractures or tears of the Quadriceps are rare.
Case Report: A 27-year-old male presented after a fall under the influence of alcohol, along with pain in the knee and inability to bend it. Radiographs revealed an undisplaced vertical split type of Patellar fracture with an osteochondroma of the distal femur located anteriorly, and growing towards the knee joint. Patient had a previous history of mechanical symptoms, occasional knee pain, limited range of motion and repeated falls. Computed tomography and magnetic resonance imaging showed an associated incomplete, non-insertional quadriceps rupture. The patella fracture eventually healed conservatively in the cylindrical cast before the patient underwent surgery for mechanical problems around his knee. Patient consented to undergo surgical intervention after a period 1 month since injury in the form of exostosis excission en bloc, extra-periosteally, followed by repair of the quadriceps tendon, with an uneventful post-surgery rehabilitation phase.
Conclusion: The unusual location of the osteochondroma along with the fact that it was directly impinging on the upper part of the Patella and the distal quadriceps tendon makes this an interesting case. The long history of “pseudo locking” and instability in this cases should have prompted earlier diagnostic interventions, which were delayed due to his alcohol dependence. The anterior location of the osteochondroma at the knee may have relevance in causing patellar degeneration and instability and lead to associated tears of the quadriceps even with lesser trauma.
Keywords: Osteochondroma knee, patella fracture, quadriceps tendon rupture, locked knee.
Osteochondromas around the knee are fairly common developmental bone lesions and usually presenting in adolescence. The majority are solitary and occur due to sporadic mutations, which is different from multiple osteochondromatosis which is an autosomal dominant trait [1]. Most of these are asymptomatic, are usually growing away from the joint and tend to migrate away from it with growth. A large number can be on the posterior aspect of the knee where occasional cases could either cause Popliteal artery compression [2] or Deep vein thrombosis (DVT) [1]. Some have been linked with limb deformities [3], fractures, bursitis [4], neurologic symptoms and occasionally there maybe malignant transformation [5]. Proximal tibia osteochondromas can mimic Ossgood Schlatter disease [6] or involve the Hoffa’s fat pad [7]. Mechanical symptoms have been reported, mostly with proximal tibia medial growths [8], but distal femoral osteochondromas causing mechanical symptoms has not been reported. Problems related to instability or occurrence of patellar fractures or even ruptures of the tendons with minor trauma are not documented in the literature. Anterior osteochondroma of the distal femur causing features of instability and mechanical block has not been reported; we present one case who came with fracture of the patella, and previous mechanical symptoms due to the anterior osteochondroma; an associated quadriceps tendon rupture was attributed to the unique location of the growth.
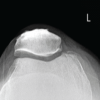
A 27-year-old male presented to our emergency department with pain, swelling, and a restriction of knee motion range after a fall. Physical examination revealed tenderness, swelling and local rise of temperature over the left knee; he was unable to lift his leg unaided (Fig. 1a). The distal neurovascular status was intact. Radiographs revealed an undisplaced fracture of the left patella, along with an anterior femoral exostosis, impinging against the patella (Fig. 1b). The patient was an alcoholic and did not want any surgical intervention at that time; an above-knee Plaster of Paris cylindrical cast was applied with the knee in extension; computed tomography scan (Fig. 2a and b) of the knee showed anterior osteochondroma of the knee facing the patella articular surface alongwith a vertical split type patella fracture. The patient left the hospital against medical advise with cast in situ.


After 1 month, the patient presented with Coronavirus disease 2019 (COVID-19) infection, with the plaster cast in place. He was explained about the problems being caused by the knee osteochondroma, and its prognosis if the exostosis was not excised. Magnetic resonance imaging showed more details of the anterior exostosis, with a cartilage cap of <1 cm; it also revealed a partial rupture of the the lateral half of quadriceps tendon away from its insertion at the patella (Fig. 2c and d). Psychiatric consultation for alcohol de-addiction was taken and appropriate treatment was initiated; patient consented to undergo surgical treatment as he had a long history of mechanical problems around the knee.
Procedure
Under regional anesthesia, in a supine position, a vertical midline incision was given and a medial parapatellar approach was established. Patella fracture was found to be united and was retracted to expose the osteochondroma. Extra periosteal resection of osteochondroma was performed and the specimen was sent for histopathology. The Quadriceps tendon found ruptured away from its insertion, was repaired end to end suture technique with Krackow suture using a No. 5 Ethibond suture and no suture anchors were used (Fig. 3). The wound was closed in layers, and the limb was immobilized in a cylindrical slab applied for 4 weeks.

The size of the excised exostosis was 3 × 2 × 1.8 cm; was sent for histopathology evaluation which revealed an outer cap of mature hyaline cartilage cap, measuring 0.5 cm and no atypical nuclei. These histopathologic findings were consistent with osteochondroma (Fig. 4).

After 2 weeks of partial weight bearing, the patient was allowed to progressively bear weight over the left lower limb. Closed knee chain exercises were started at 6 weeks, subsequently followed by open chain knee exercises. Psychiatric follow-up was continued for 6 weeks. Range of motion was near normal at the end of the 1-year postoperatively with pain-free movement at the knee (Fig. 5).

Solitary osteochondroma is not so uncommon in the general population, with many cases reported around the knee; what is uncommon is an anterior intra articular location and the mechanical symptoms caused by it in relation to the patella. Normally these bony swellings are located posteromedially in the distal femur, where they could cause neurovascular compression and even masquerade as DVT [1]. Less commonly these maybe located anterolaterally, but anterior intra articular location, with obstruction at the patello-femoral joint is extremely rare. In addition, the usual direction of the exostosis growth is away from the joint, which was not the case here as it was directly facing the patella. The mechanical symptoms of the exostosis were probably responsible for the repeated falls of the patient, which could be aggravated by his alcohol addiction; the associated quadriceps tendon rupture with the undisplaced patella fracture could have been due the prominent exostosis under it, or by repeated attrition over the years. Another few known causes of quadriceps rupture can be classified as either traumatic or atraumatic. Atraumatic causes include eccentric contraction of the quadriceps during a simple fall or no trauma at all in patients who have predisposing factors such as chronic tendinopathy, prior anterior cruciate ligament surgery using an autologous patellar tendon graft, or conditions such as diabetes mellitus, chronic renal failure, secondary hyperparathyroidism, gout, rheumatoid arthritis, systemic lupus erythematosus, calcium pyrophosphate deposition disease, obesity, and a history of quinolone or steroid use [9]. In our case, each of these conditions, except repititve trauma due to the lesion, had been ruled out. These lesions are more often managed conservatively due to their benign nature with a minimal chance of transforming into malignancy [10]. Malignant transformation occurs in 1% of solitary lesions and 3–5% in Hereditary Multiple Exostosis, with the commonest malignant transformation to chondrosarcoma [11,12]. Nevertheless large tumours and those causing significant compression and symptoms need to be excised. The standard excision protocol involves excision of a large base of sessile osteochondroms, with good long term outcomes [10]. For intra-articular smaller lesions arthroscopic procedures have also been used [13] but the indications are limited.
We present an anterior distal femoral osteochondroma, which presented with symptoms due to impingement at the patello-femoral joint associated with falls. The long history of “pseudo locking” and instability in this case should have prompted earlier diagnostic interventions, which were delayed due to his alcohol dependence. The patella fracture and quadriceps tendon rupture occurred due to plausible consequences of the lesion. Surgical management of the osteochondroma, lead to an uneventfull recovery in our case, manifests the need for adequate early diagnosis and management of such lesions.
Large tumours including osteochondromas and those causing mechanical symptoms or compression need to be excised, especially the ones that occur in an anterior intra articular location, causing obstruction at the patello-femoral joint.
References
- 1.Dhillon M, Kumar V, Bachhal V, Bali K. Distal femoral osteochondroma masquerading as deep vein thrombosis in an adolescent male. J. Knee Surg. 2013 Dec;26(S 01):S011-5. doi 10.1055/s-0031-1280974. [Google Scholar | PubMed | CrossRef]
- 2.Mihoubi M, Sayed W, Barkallah O, Mbarek M. Popliteal artery entrapment syndrome secondary to a femoral osteochondroma. Tunis Med. 2020 Dec;98(12):1039-41. [Google Scholar | PubMed]
- 3.Oh S, Won SH, Kim WS, Park MS, Sung KH. Lower extremity deformity and its risk factors in patients with solitary osteochondromas. J Orthop Surg Res. 2024 Jul 19;19(1):415. https://doi.org/10.1186/s13018-024-04908-4. [Google Scholar | PubMed | CrossRef]
- 4.Saglam F, Serttas MF. Solitary medial proximal tibial osteochondromas cause pes anserinus syndrome in adolescents. J Child Orthop. 2024 Sep 8;18(5):477-85. doi:10.1177/18632521241276323. [Google Scholar | PubMed | CrossRef]
- 5.Sułko J, Lejman T. Chondrosarcoma na podłozu pojedynczej wyrośli chrzestno-kostnej--opis chorego i przeglad piśmiennictwa [Chondrosarcoma arising in a solitary osteochondroma--case report and literature review]. Chir Narzadow Ruchu Ortop Pol. 1998;63(2):179-84. DOI: 10.1007/bf02564786. [Google Scholar | PubMed | CrossRef]
- 6.Balaji G, Palaniappan P, Nema S, Menon J. Solitary Osteochondroma of the Tibial Tuberosity Mimicking Osgood-Schlatter Lesion: A Rare Cause of Anterior Knee Pain in Adolescents: A Case Report. Malays Orthop J. 2016 Jul;10(2):47-9. doi: 10.5704/MOJ.1607.009. [Google Scholar | PubMed | CrossRef]
- 7.Hashimoto K, Nishimura S, Yamagishi K, Tsukamoto I, Nakagawa K, Inoue S, Asada S, Kakinoki R, Akagi M. Extra-articular synovial osteochondroma of the Hoffa's fat pad involving the patellar tendon: A case report and literature review. Mol Clin Oncol. 2020 Apr;12(4):355-7. https://doi.org/10.3892/mco.2020.1998. [Google Scholar | PubMed | CrossRef]
- 8.Kairy RR, Bari MM, Islam MA, Alam MJ, Barna B. An epiphyseal osteochondroma causing mechanical symptoms in the knee. Mymensingh Med J. 2012 Jul;21(3):550-2. [Google Scholar | PubMed]
- 9.Bottner F, Rodl R, Kordish I, Winkelmann W, Gosheger G, Lindner N. Surgical treatment of symptomatic osteochondroma: a three-to eight-year follow-up study. J Bone Joint Surg Br. 2003 Nov;85(8):1161-5. doi:10.1302/0301-620X.85B8.14059. [Google Scholar | PubMed | CrossRef]
- 10.Bernard SA, Murphey MD, Flemming DJ, Kransdorf MJ. Improved differentiation of benign osteochondromas from secondary chondrosarcomas with standardized measurement of cartilage cap at CT and MR imaging. Radiology. 2010 Jun;255(3):857-65. https://doi.org/10.1148/radiol.10082120. [Google Scholar | PubMed | CrossRef]
- 11.Murphey MD, Robbin MR, McRae GA, Flemming DJ, Temple HT, Kransdorf MJ. The many faces of osteosarcoma. Radiographics. 1997 Sep;17(5):1205-31. https://doi.org/10.1148/radiographics.17.5.9308111. [Google Scholar | PubMed | CrossRef]
- 12.Kulkarni S, Patil VS, Naik S, Bhansali Y. Arthroscopic Excision of a Solitary Intra-articular Osteochondroma Manifesting as a Loose Body: A Presentation of an Extremely Rare Medical Condition. Cureus. 2024 Aug 3;16(8):e66083. doi: 10.7759/cureus.66083. [Google Scholar | PubMed | CrossRef]





Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Single Peg Patellar Component Fracture in Total Knee Replacement: A Case Report
March 1, 2026 Single Peg Patellar Component Fracture in Total Knee Replacement: A Case Report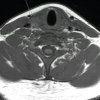 November 1, 2025 Bilateral Distal Quadriceps Tendon Rupture in a Young Male Following Minimal Trauma: First Presentation of Primary Hyperparathyroidism Due to a Parathyroid Adenoma
November 1, 2025 Bilateral Distal Quadriceps Tendon Rupture in a Young Male Following Minimal Trauma: First Presentation of Primary Hyperparathyroidism Due to a Parathyroid Adenoma July 1, 2025 Locked Knee and Inferior Patellar Dislocation in an Elderly Patient: A Case Report and Review of the Literature
July 1, 2025 Locked Knee and Inferior Patellar Dislocation in an Elderly Patient: A Case Report and Review of the Literature January 1, 2025 Novel Technique for Fracture Fixation of the Patella Following Unicondylar Knee Replacement: A Clinical Case Report
January 1, 2025 Novel Technique for Fracture Fixation of the Patella Following Unicondylar Knee Replacement: A Clinical Case Report